Page 9 of 22
PA8.6 | HIV & AIDS — SDL Guide
Learning Objectives
- Describe the structure and virology of HIV as a retrovirus
- Explain the routes of HIV transmission
- Detail the molecular mechanisms of HIV entry into CD4+ T cells, macrophages, and dendritic cells
- Outline the natural history of HIV infection across its three phases (acute, chronic latency, AIDS)
- Identify the major opportunistic infections stratified by CD4+ T-cell count
- List AIDS-defining malignancies and their viral co-factors
- Describe the laboratory diagnosis of HIV including screening, confirmatory tests, and monitoring parameters
- Explain the principles of antiretroviral therapy (ART)
INSTRUCTIONS
HIV/AIDS remains the paradigm immune-deficiency disease — understanding its pathogenesis illuminates how the immune system works and fails. By Year 2, you have studied immunity in Physiology and microbiology basics; this module uses that foundation to explain why a single virus dismantles host defence systematically, producing a predictable cascade of infections and malignancies that map precisely onto CD4+ T-cell count. Mastering this prepares you for clinical microbiology, medicine, and surgery postings where AIDS presentations are frequent and high-stakes.
References
- Robbins & Kumar — Basic Pathology, 11th ed., Ch 5 (Diseases of Immunity) (textbook)
- Harsh Mohan — Textbook of Pathology, 8th ed., Ch 12 (Immunopathology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old man presents with a three-week history of fever, sore throat, generalised lymphadenopathy, and a fleeting maculopapular rash. His ELISA for HIV is negative. Six weeks later, repeat ELISA is positive. How can someone with active HIV infection test negative — and what was happening inside his CD4+ T cells during those six weeks?
WHY THIS MATTERS
HIV is the most consequential immunodeficiency syndrome in human history. India has approximately 2.4 million people living with HIV, ranking third globally. As a clinician you will encounter AIDS-related opportunistic infections across every specialty — a CD4 count of 50 and bilateral pulmonary infiltrates on a chest X-ray is a life-threatening emergency that demands immediate pattern recognition. Understanding the mechanism of CD4 depletion explains why each infection appears at its characteristic threshold, and why ART can reverse seemingly irreversible immunosuppression.
RECALL
Before proceeding, consolidate three concepts from Year 1:
- CD4+ T helper cells orchestrate adaptive immunity — they activate macrophages (Th1) and help B cells produce antibodies (Th2 / Tfh). Loss of this axis has consequences in every arm of the immune system.
- Reverse transcriptase — recall from Biochemistry that retroviruses carry RNA and use this enzyme to copy RNA → DNA (the reverse of the central dogma). This is the molecular Achilles heel exploited by ART.
- Opportunistic infection — a pathogen that causes disease only (or far more severely) when host defences are compromised. Understanding which defences are lost predicts which pathogens emerge.
HIV Structure and Virology
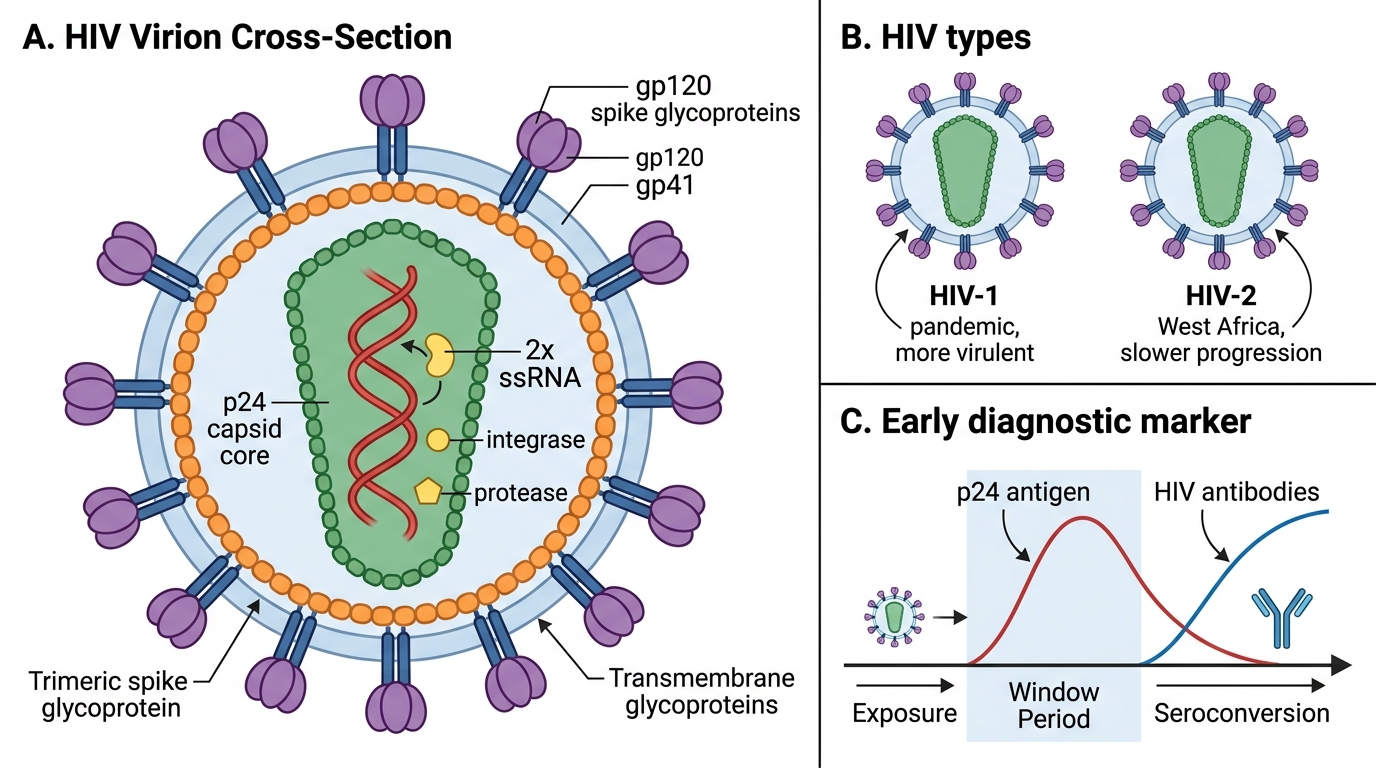
HIV (Human Immunodeficiency Virus) belongs to the Lentivirus genus of the family Retroviridae. Two types exist: HIV-1 (pandemic; most virulent) and HIV-2 (West Africa; slower progression).
Genome and structure:
• Enveloped spherical virion, ~120 nm diameter
• Two copies of single-stranded (+)RNA genome (~9.8 kb)
• Enzymes packaged in the virion: reverse transcriptase (RT), integrase, and protease — all drug targets
• Matrix (MA/p17) inside the lipid envelope; cone-shaped capsid (CA/p24) core
Envelope glycoproteins — the entry machinery:
• Outer trimeric spikes formed by non-covalent association of gp120 (surface unit) and gp41 (transmembrane unit)
• gp120 binds host CD4 and co-receptors; gp41 drives membrane fusion
IMPORTE: the p24 antigen is the earliest serological marker detected in the window period — a concept you will use in diagnosis.
HIV Structure, Types, and Early Marker
Transmission Routes
HIV Transmission Routes
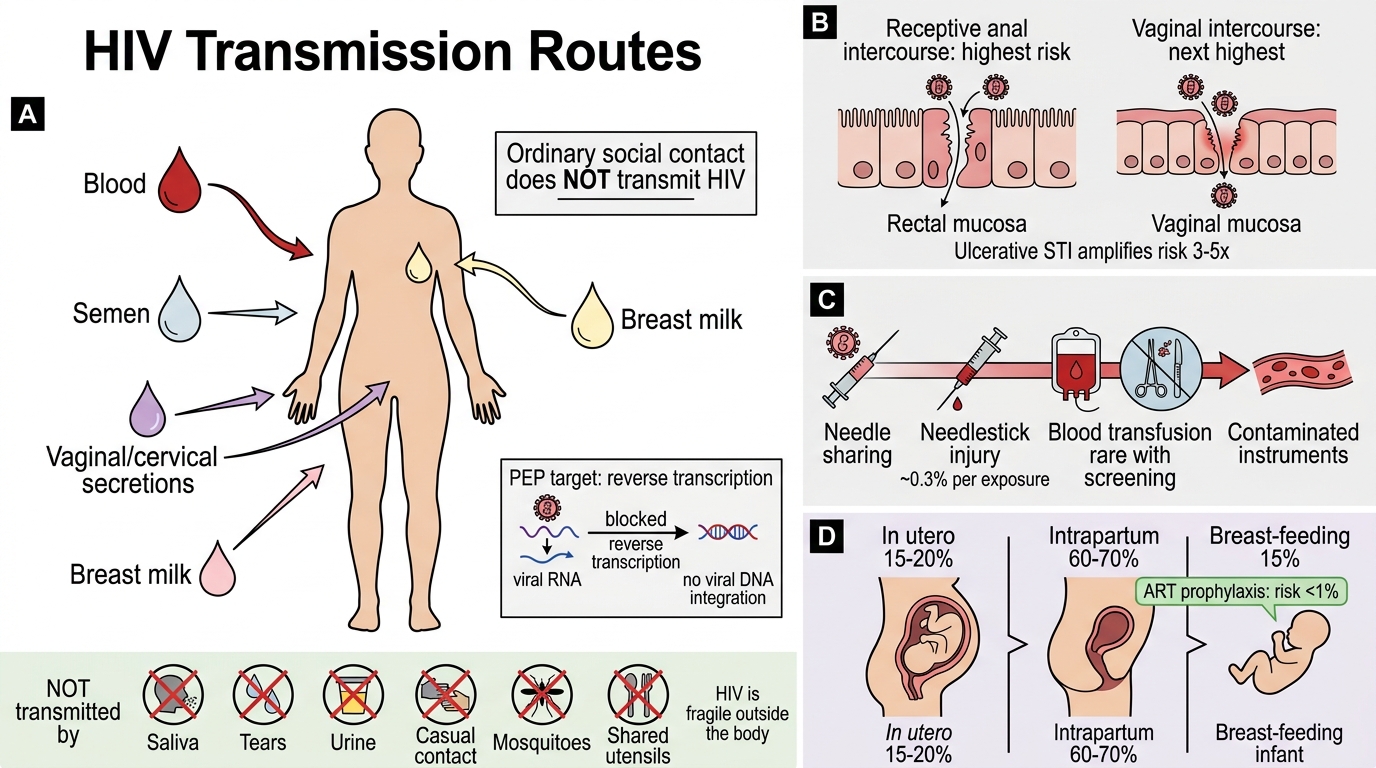
HIV is transmitted exclusively through specific body fluids containing free virus or infected cells: blood, semen, vaginal/cervical secretions, and breast milk. Ordinary social contact does NOT transmit HIV.
Three main routes:
- Sexual transmission — most common globally; risk highest for receptive anal intercourse (rectal mucosa thin, trauma-prone); vaginal intercourse next; co-existing STIs (especially ulcerative — HSV, syphilis) amplify risk 3–5×
- Parenteral transmission — needle sharing among intravenous drug users; needlestick injuries (healthcare workers, ~0.3% per exposure); blood transfusions (now rare with screening); contaminated surgical instruments
- Mother-to-child (vertical) transmission — in utero (15–20%), intrapartum (60–70%), breast-feeding (15%); ART prophylaxis reduces risk to < 1%
NOT transmitted by: saliva, tears, urine, casual contact, mosquitoes, or shared utensils. HIV is fragile outside the body.
SELF-CHECK
A healthcare worker sustains a needlestick injury from a known HIV-positive patient. Which step in the HIV life cycle does post-exposure prophylaxis (PEP) target to prevent viral integration?
A. Reverse transcription of viral RNA into DNA
B. Glycoprotein gp120 binding to CD4 on the host cell
C. Budding of new virions from the infected cell
D. Cleavage of viral polyproteins by HIV protease
Reveal Answer
Answer: A. Reverse transcription of viral RNA into DNA
PEP regimens include a nucleoside reverse transcriptase inhibitor (NRTI) as the backbone. RT is the key early step after viral entry — blocking RNA→DNA conversion prevents the provirus from forming and the virus from establishing latent infection. Entry inhibitors (blocking gp120/CD4) and protease inhibitors are also used but the NRTI backbone is what makes PEP effective against early integration.
HIV Entry and Pathogenesis — Molecular Mechanisms
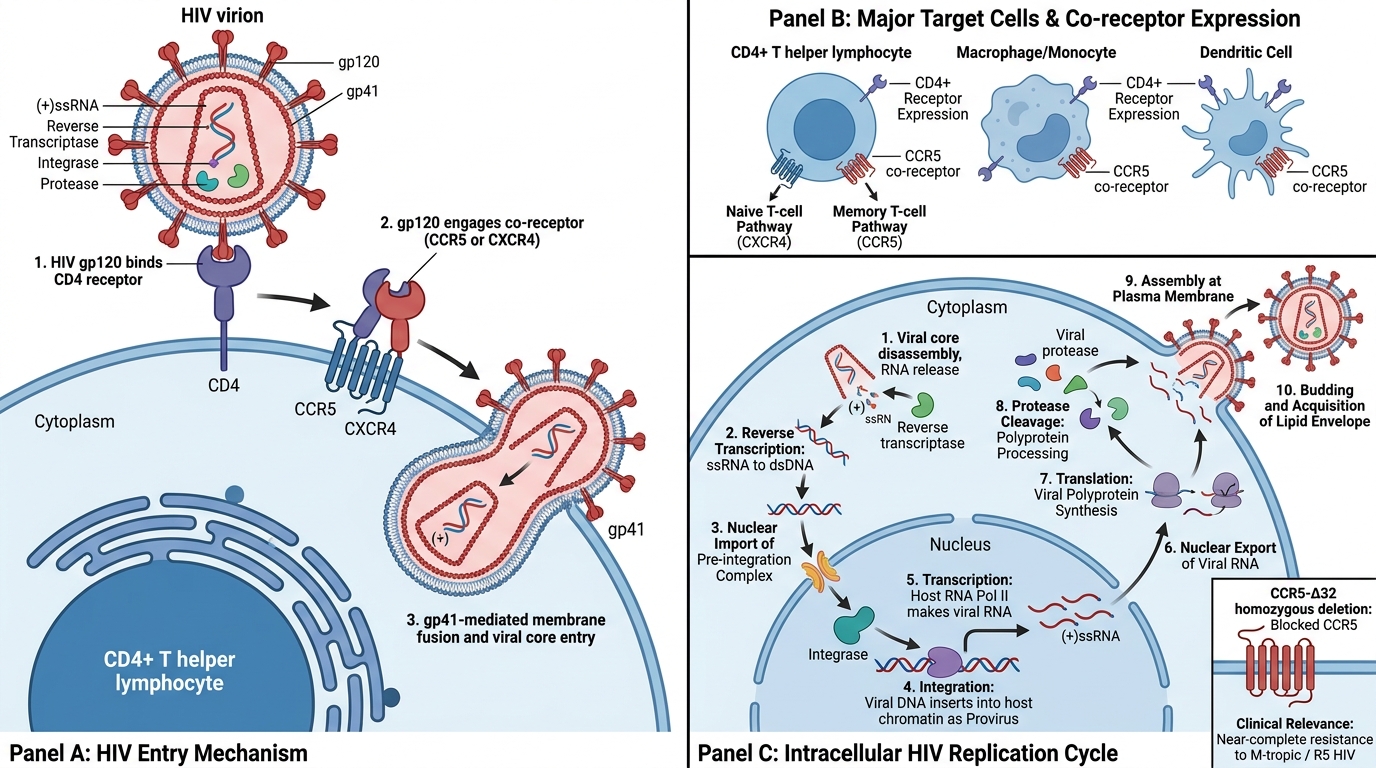
Target cells: CD4+ T helper lymphocytes (primary target), macrophages/monocytes, and dendritic cells (DCs). The common thread is expression of CD4 as the primary receptor.
Entry: a two-receptor lock-and-key:
1. gp120 binds CD4 → conformational change exposes the co-receptor binding site
2. gp120 then engages a chemokine co-receptor — CCR5 (on macrophages and memory T cells; used by M-tropic / R5 strains) or CXCR4 (on naïve T cells; used by T-tropic / X4 strains, emerge late in infection)
3. Binding triggers gp41-mediated membrane fusion → viral core enters cytoplasm
Clinical relevance: Individuals homozygous for the CCR5-Δ32 deletion (1% of Northern Europeans) are nearly completely resistant to M-tropic HIV infection.
Intracellular replication cycle:
1. Reverse transcription: RT converts (+)ssRNA → dsDNA (prone to errors → genetic diversity, drug-resistance mutations)
2. Nuclear import of pre-integration complex
3. Integration: viral integrase inserts dsDNA into host chromatin as provirus — permanent; replicates with every cell division
4. Transcription/translation: host RNA polymerase II transcribes provirus; viral proteins synthesised and cleaved by protease
5. Assembly and budding: new virions bud at plasma membrane, acquiring lipid envelope
HIV Entry and Replication in CD4+ Cells