Page 10 of 22
PA8.6 | HIV & AIDS — SDL Guide (Part 2)
Mechanisms of CD4+ T-Cell Depletion
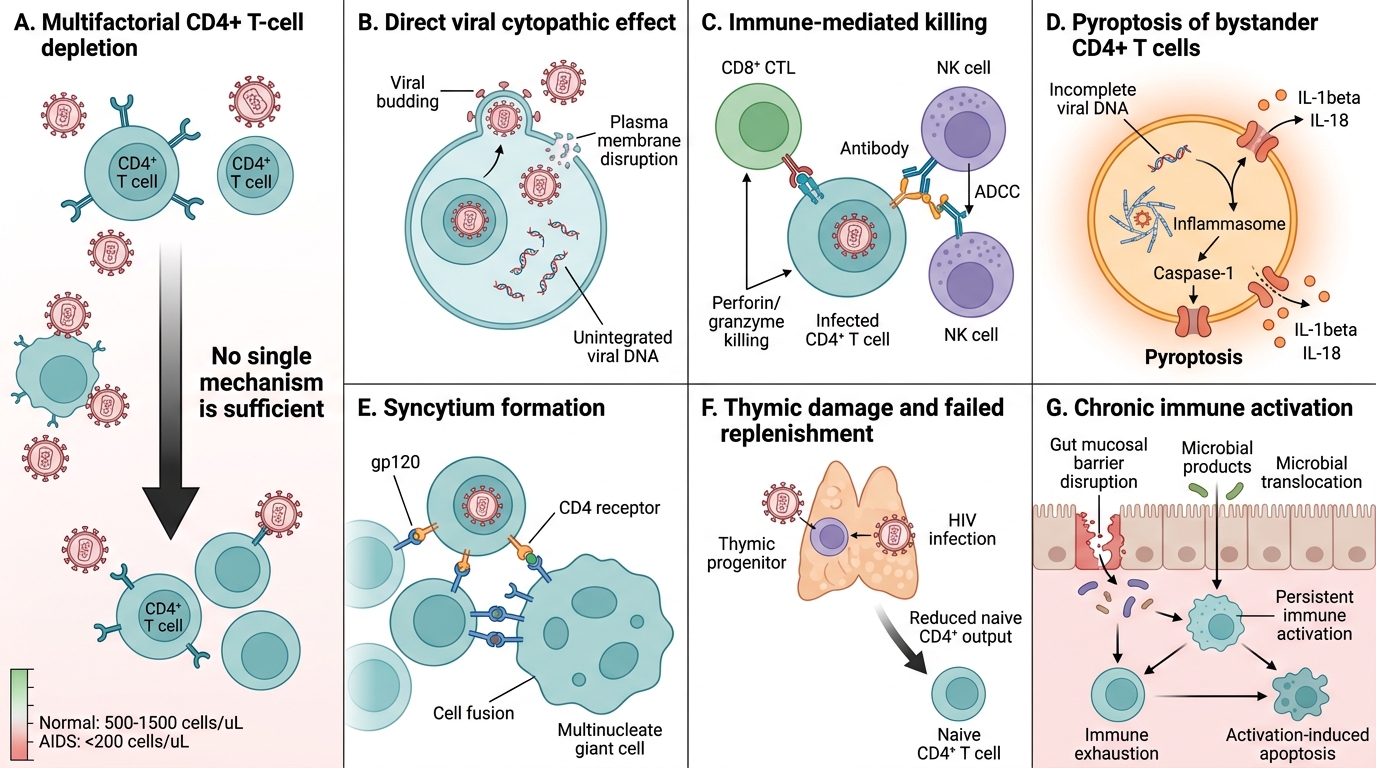
Mechanisms of CD4+ T-Cell Depletion in HIV
CD4+ T-cell destruction is multifactorial — no single mechanism is sufficient:
- Direct viral cytopathic effect — viral budding disrupts plasma membrane; accumulation of unintegrated viral DNA is toxic
- Immune-mediated killing — CD8+ cytotoxic T cells (CTLs) kill HIV-infected CD4+ cells; ADCC (antibody-dependent cellular cytotoxicity) by NK cells
- Pyroptosis (major mechanism for abortive infection): CD4+ bystander T cells ingest incomplete viral DNA → inflammasome activation (caspase-1) → inflammatory programmed death → releases IL-1β and IL-18 (fuelling immune activation)
- Syncytium formation — gp120 on infected cells binds CD4 on uninfected neighbours → multinucleate giant cells, killed by fusion
- Thymic damage and failure — HIV infects thymic progenitors, reducing naïve CD4+ replenishment
- Chronic immune activation — persistent microbial translocation (gut mucosal barrier disruption) drives immune exhaustion and activation-induced apoptosis
Normal CD4+ count: 500–1500 cells/µL. AIDS is defined by CD4 < 200 cells/µL.
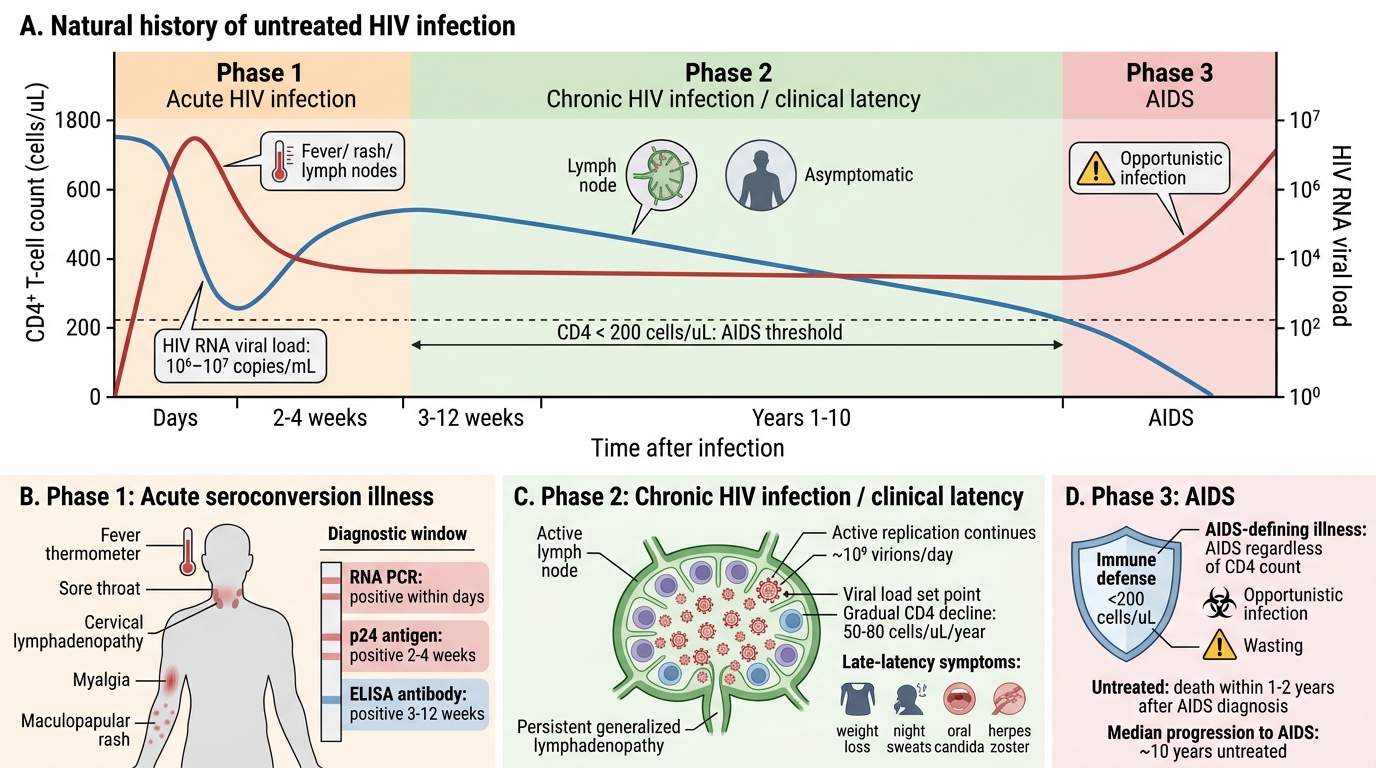
Natural History of HIV Infection — Three Phases
HIV infection follows a predictable natural course over years to decades if untreated.
Phase 1 — Acute HIV Infection (Acute Seroconversion Illness):
• 2–4 weeks post-infection; presents as a flu/infectious-mononucleosis-like illness: fever, sore throat, lymphadenopathy, myalgia, maculopapular rash
• Viraemia peaks at 10⁶–10⁷ copies/mL; CD4 count drops sharply (may fall below 200 transiently)
• Host immune response (CTLs + antibodies) partially controls virus; CD4 count recovers but not to baseline
• Window period: ELISA becomes positive 3–12 weeks post-infection; p24 antigen positive 2–4 weeks (earlier); RNA PCR positive within days — explains the hook scenario
Phase 2 — Chronic HIV Infection / Clinical Latency:
• Lasts 8–10 years (untreated average); virus is NOT truly latent — active replication continues (~10⁹ virions produced daily)
• Gradual CD4 decline (~50–80 cells/µL per year); patient may be asymptomatic or have persistent generalised lymphadenopathy (PGL)
• Viral load settles at a set point (individual viral load plateau) — predictor of progression speed
• Late in latency: constitutional symptoms (weight loss, night sweats, oral candida, herpes zoster) as CD4 approaches 200
Phase 3 — AIDS (Acquired Immune Deficiency Syndrome):
• CD4 < 200 cells/µL OR presence of an AIDS-defining illness (regardless of CD4 count)
• Without treatment, progression to AIDS: median 10 years; death within 1–2 years of AIDS diagnosis
Natural History of Untreated HIV Infection
CLINICAL PEARL
The set point viral load after acute infection is the single best predictor of the rate of CD4 decline and time to AIDS — more predictive than the CD4 count at that time. A patient with a set point of 30,000 copies/mL will progress ~3× faster than one with a set point of 1,000. This is why clinicians check both CD4 count and viral load at every HIV visit: CD4 tells you where the patient is now; viral load tells you how fast they're travelling.
SELF-CHECK
A 34-year-old woman is diagnosed with HIV. Her CD4 count is 420 cells/µL and viral load is 85,000 copies/mL. She feels well. Which statement best characterises her current stage?
A. AIDS — she should be started on prophylaxis for Pneumocystis jirovecii pneumonia immediately
B. Chronic HIV infection / clinical latency — active viral replication ongoing despite apparent wellness
C. Acute seroconversion illness — the high viral load indicates she was infected within the last 4 weeks
D. Undetectable HIV — the CD4 count is normal so she does not require ART yet
Reveal Answer
Answer: B. Chronic HIV infection / clinical latency — active viral replication ongoing despite apparent wellness
A CD4 count > 200 with symptoms absent places her in chronic (clinical latency) phase. However, 'latency' is a misnomer — ~10⁹ new virions are produced daily. Her high viral load (85,000 copies/mL) indicates fast progression; current guidelines recommend ART for all HIV+ individuals regardless of CD4 count, urgently so with high viral load. PCP prophylaxis is not yet indicated (CD4 > 200). Acute seroconversion presents much earlier (weeks).
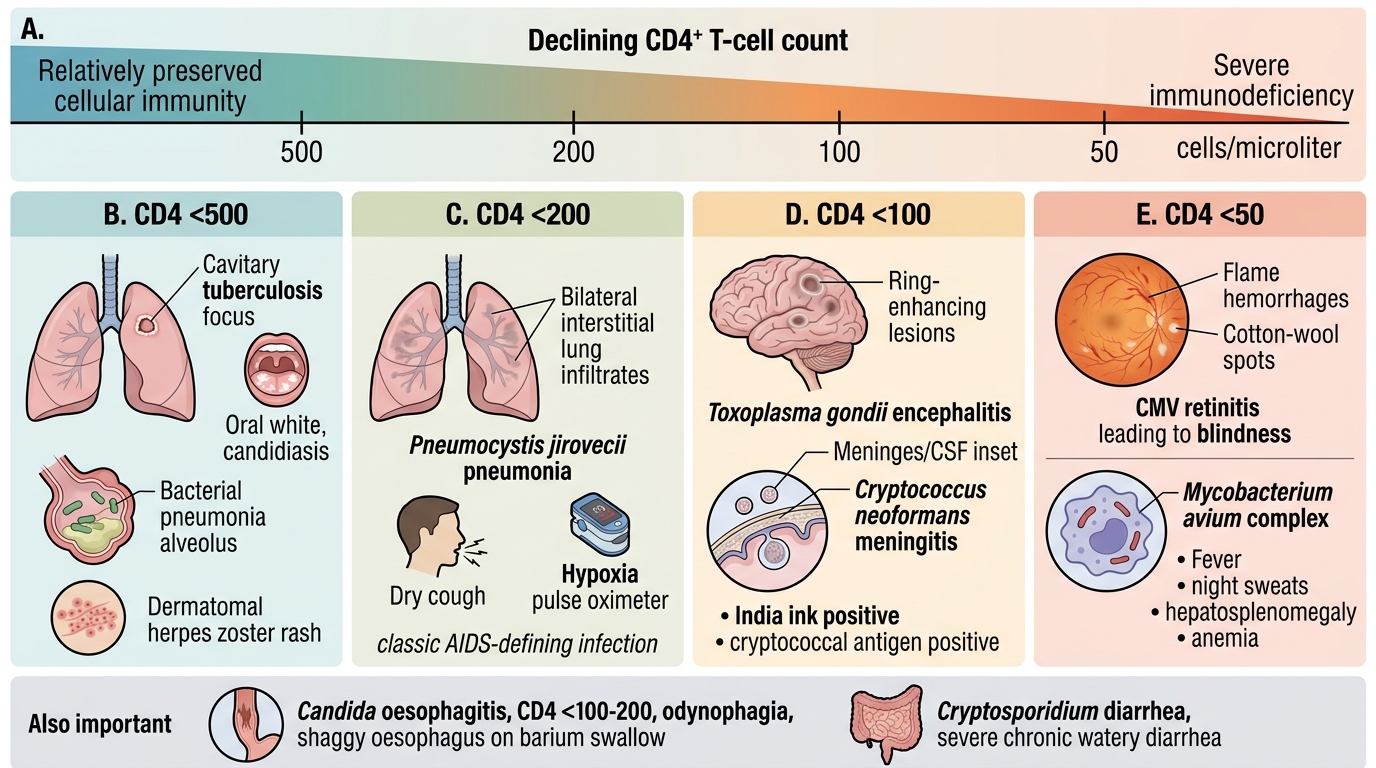
Opportunistic Infections Stratified by CD4+ Count
As CD4+ T-cell count falls, the immune deficiencies manifest in a characteristic sequence. Knowing the CD4 threshold for each infection is essential for clinical diagnosis and prophylaxis decisions.
| CD4 range | Pathogens / infections |
|---|---|
| < 500 | Tuberculosis (all forms, may reactivate at any CD4), oral candidiasis, recurrent bacterial pneumonia, herpes zoster |
| < 200 | Pneumocystis jirovecii pneumonia (PCP) (formerly P. carinii) — bilateral interstitial infiltrates, dry cough, hypoxia; classic AIDS-defining infection |
| < 100 | Toxoplasma gondii encephalitis (ring-enhancing brain lesions, seizures); Cryptococcus neoformans meningitis (India ink stain, cryptococcal antigen) |
| < 50 | Cytomegalovirus (CMV) retinitis (flame haemorrhages + cotton-wool spots → blindness); Mycobacterium avium complex (MAC) (fever, night sweats, hepatosplenomegaly, anaemia) |
Also important:
• Candida oesophagitis (CD4 < 100–200): odynophagia, barium swallow shows shaggy oesophagus
• Cryptosporidium diarrhoea: severe, watery, chronic (CD4 < 100)
• Progressive multifocal leukoencephalopathy (PML): JC virus reactivation → demyelination (CD4 < 100)
Opportunistic Infections by CD4+ Count