Page 11 of 22
PA8.6 | HIV & AIDS — SDL Guide (Part 3)
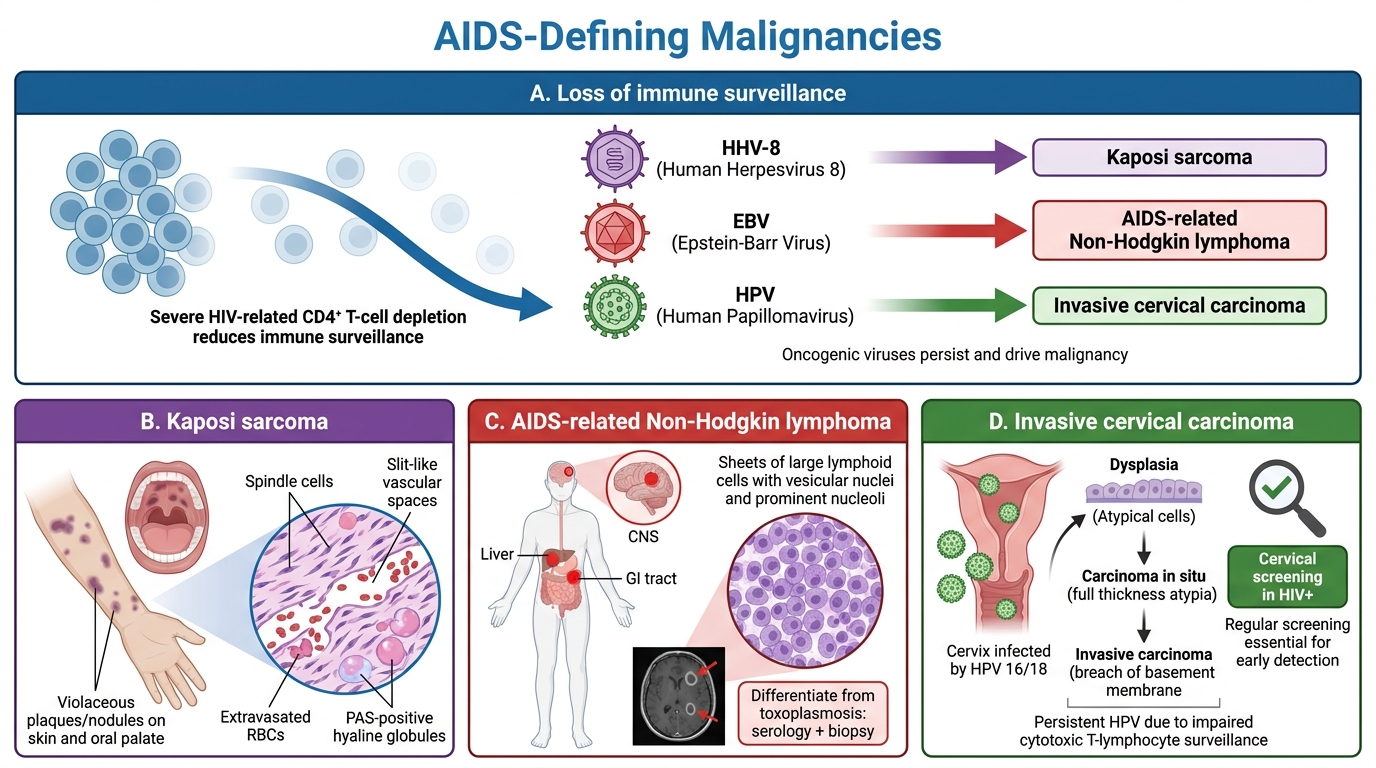
AIDS-Defining Malignancies
Immune surveillance normally eliminates cells transformed by oncogenic viruses. Profound CD4 depletion allows these viruses to drive malignancy.
Kaposi Sarcoma (KS):
• Caused by HHV-8 (Human Herpesvirus-8 / Kaposi sarcoma-associated herpesvirus)
• Endothelial-derived vascular tumour; most common AIDS malignancy
• Presents as violaceous (purple-brown) patches/plaques/nodules on skin, mucous membranes, viscera
• Histology: spindle cells, slit-like vascular spaces, RBCs extravasated, PAS-positive hyaline globules
AIDS-related Non-Hodgkin Lymphoma (NHL):
• Usually high-grade B-cell lymphomas (diffuse large B-cell lymphoma, Burkitt lymphoma)
• Frequently EBV-associated; extranodal sites predominant (CNS, GI tract, liver)
• CNS primary lymphoma: solitary or multiple ring-enhancing lesions (must distinguish from toxoplasmosis — serology + biopsy)
Invasive Cervical Carcinoma:
• Associated with HPV (types 16, 18) — impaired CTL surveillance allows HPV persistence and malignant transformation
• An AIDS-defining illness in women; highlights importance of cervical screening in HIV+
AIDS-Defining Malignancies
SELF-CHECK
A 31-year-old HIV-positive man presents with painless violaceous nodules on his palate and forearm, and a CD4 count of 45 cells/µL. Biopsy shows spindle cells with slit-like vascular channels. What is the causative oncogenic virus?
A. Epstein-Barr virus (EBV)
B. Human Papillomavirus (HPV) type 16
C. Human Herpesvirus-8 (HHV-8)
D. Cytomegalovirus (CMV)
Reveal Answer
Answer: C. Human Herpesvirus-8 (HHV-8)
The clinical picture (violaceous lesions in an AIDS patient) combined with the histology (spindle cells, slit-like vascular channels, extravasated RBCs) is classic Kaposi sarcoma. KS is driven by HHV-8 (Kaposi sarcoma-associated herpesvirus), which infects endothelial cells and prevents their apoptosis via viral FLICE-inhibitory protein (vFLIP). EBV is associated with B-cell lymphomas in AIDS; HPV with cervical cancer; CMV with retinitis, not KS.
HIV Encephalopathy, Wasting, and Other Systemic Manifestations
Systemic Manifestations of Advanced HIV Infection
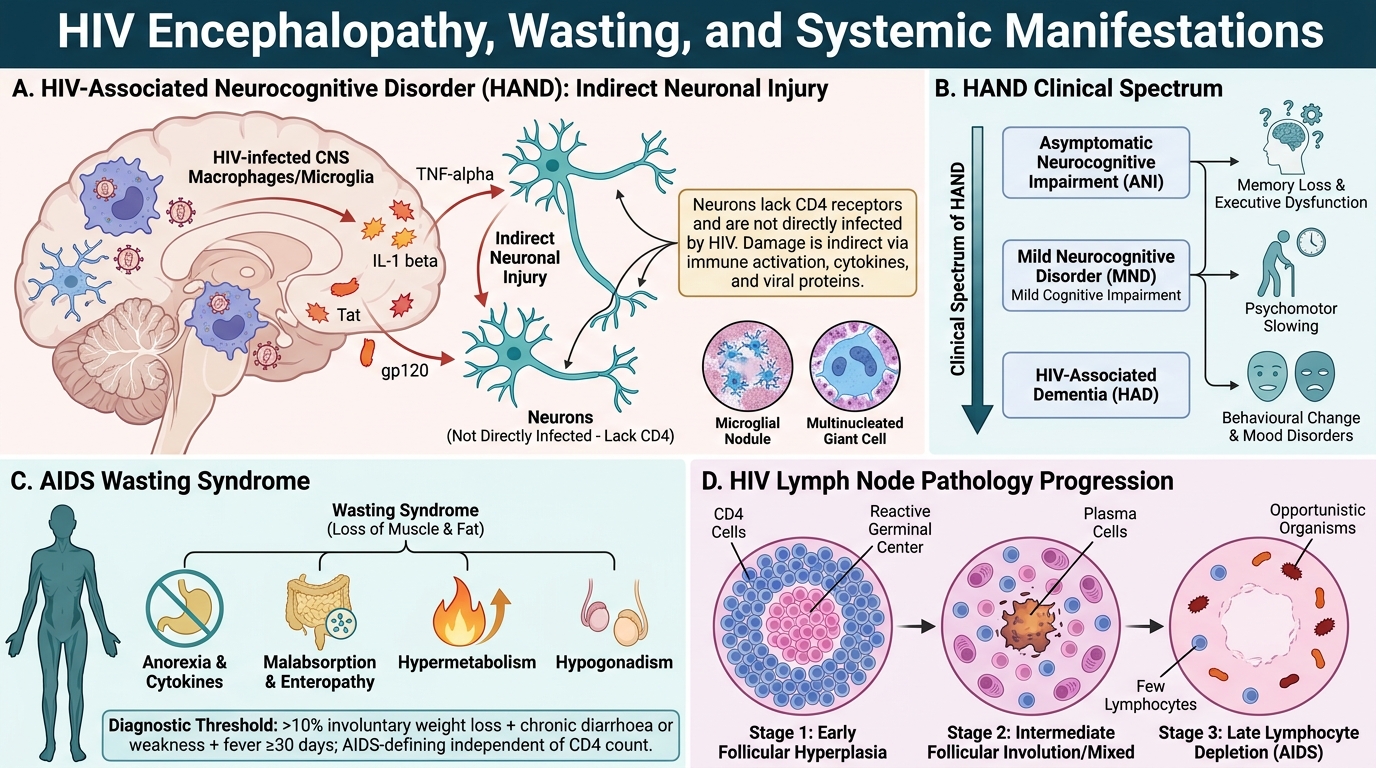
HIV-associated neurocognitive disorder (HAND) / HIV encephalopathy:
• Direct infection of CNS macrophages and microglia (not neurons directly, which lack CD4)
• Macrophages release neurotoxic cytokines (TNF-α, IL-1β), viral proteins (gp120, Tat) that damage neurons indirectly
• Clinical spectrum: mild cognitive impairment → HIV-associated dementia (HAD) — memory loss, psychomotor slowing, behavioural changes
• Pathology: microglial nodules, multinucleated giant cells (fused HIV-infected macrophages), vacuolar myelopathy of the spinal cord
AIDS wasting syndrome:
• Involuntary weight loss > 10% body weight + chronic diarrhoea or weakness + fever for ≥ 30 days
• Mechanisms: anorexia (cytokines), malabsorption (enteropathy), hypermetabolism, hypogonadism
• An AIDS-defining diagnosis independent of CD4 count
Lymph node pathology in HIV (three sequential stages):
1. Follicular hyperplasia (early): reactive germinal centres, CD4 cells around follicles
2. Follicular involution/mixed pattern (intermediate): burnt-out follicles, plasma cells
3. Lymphocyte depletion (late/AIDS): ghost follicles, few lymphocytes, opportunistic organisms visible
Laboratory Diagnosis of HIV
Laboratory Diagnosis of HIV
A systematic approach prevents missed diagnoses and false positives.
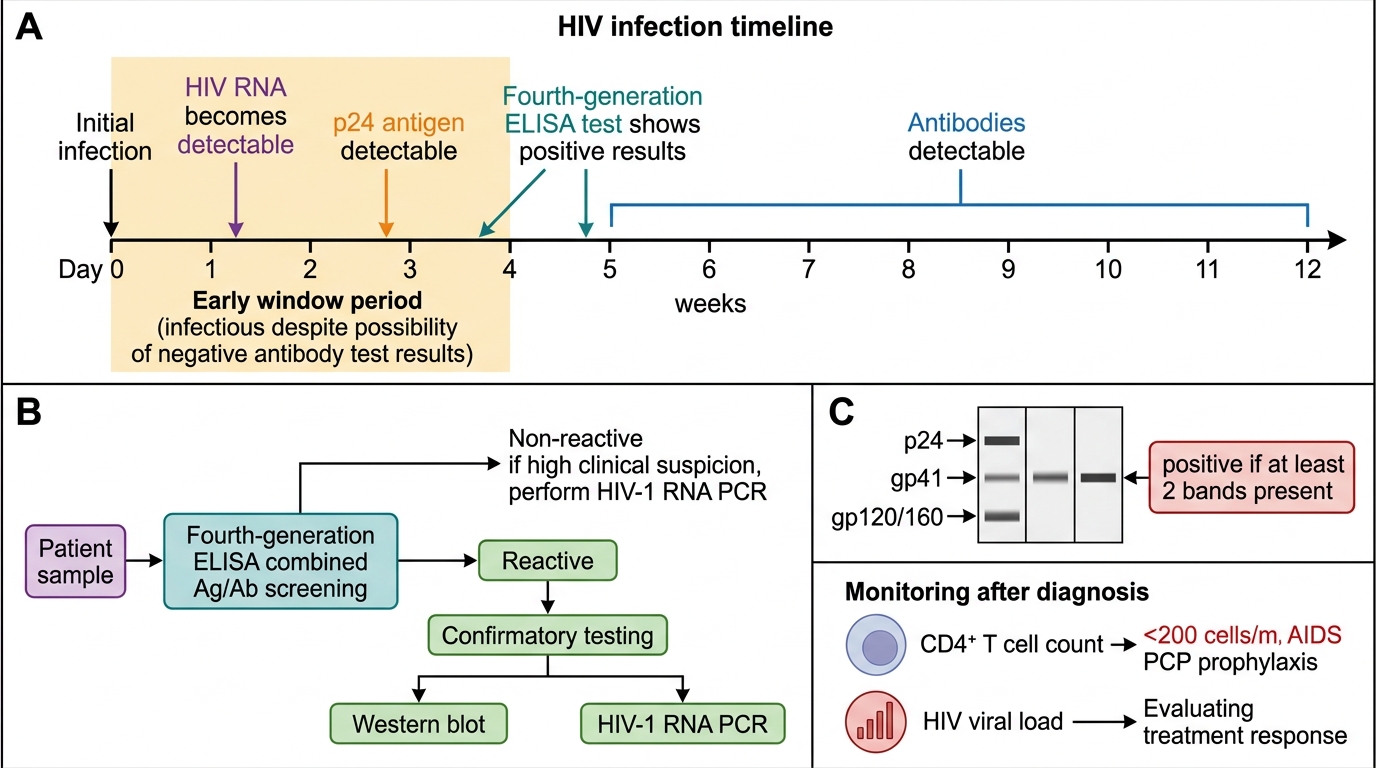
Screening — Fourth-generation ELISA (combined Ag/Ab test):
• Detects HIV-1/2 antibodies AND p24 antigen simultaneously
• Becomes positive ~2 weeks post-infection (earlier than 3rd-gen Ab-only ELISA)
• High sensitivity (~99.9%); used for initial screening
• Reactive result requires confirmation
Confirmatory tests:
• Western blot (gold standard): viral proteins separated by gel electrophoresis, probed with patient serum; positive if ≥ 2 of: p24, gp41, gp120/160 bands present
• HIV-1 RNA PCR (viral load): qualitative PCR used for confirmation in acute/window period infection when antibodies absent; also used to diagnose perinatal HIV in infants (maternal antibodies persist to 18 months)
The window period:
• Interval between infection and detectable antibody (~3–12 weeks, 4th-gen ELISA detects earlier at ~2 weeks)
• During window: patient is infectious but ELISA may be negative
• Nucleic acid tests (NAT) detect RNA within days — used for blood bank screening and suspected acute infection
Monitoring parameters:
| Test | Purpose | Target / threshold |
|---|---|---|
| CD4+ count | Staging, prophylaxis timing | < 200 → AIDS; < 200 → start PCP prophylaxis |
| Viral load (HIV RNA PCR) | Assess replication, ART response | Goal: undetectable (< 20–50 copies/mL) |
| CD4:CD8 ratio | Immune recovery | Normal ≈ 2:1; inverts in HIV (< 1) |
Principles of ART:
• Combination antiretroviral therapy (cART) uses ≥ 3 drugs from ≥ 2 classes to prevent resistance
• Drug classes: NRTIs (tenofovir, emtricitabine), NNRTIs (efavirenz), protease inhibitors (atazanavir), integrase inhibitors (dolutegravir, raltegravir), CCR5 antagonists (maraviroc)
• Goal: viral load undetectable → immune reconstitution → prevention of OIs
• 'U=U': Undetectable = Untransmittable (no sexual transmission when viral load < 200 copies/mL)
SELF-CHECK
A 26-year-old man was tested for HIV 3 weeks after a high-risk exposure. His 4th-generation combined Ag/Ab ELISA is non-reactive. Which statement is most accurate?
A. He is definitively HIV-negative and no further testing is required
B. He may be in the window period; HIV RNA PCR should be performed and repeat ELISA at 6 weeks
C. A non-reactive 4th-generation ELISA at 3 weeks fully excludes acute seroconversion illness
D. Western blot should be performed immediately as it has higher sensitivity than ELISA in early infection
Reveal Answer
Answer: B. He may be in the window period; HIV RNA PCR should be performed and repeat ELISA at 6 weeks
Although 4th-gen ELISA detects p24 antigen earlier than antibody-only tests (positive from ~2 weeks), the window period can extend to 6 weeks for this assay. A single negative test at 3 weeks does not exclude infection. HIV RNA PCR (qualitative NAT) would detect viraemia within days of infection and should be done if acute HIV is suspected clinically. A repeat ELISA at 6 weeks (and optionally 12 weeks) is recommended. Western blot is a confirmatory test for reactive screens, not a more sensitive primary test.
Putting It Together — Clinico-Pathological Correlations
HIV Clinico-Pathological Correlations
The table below integrates the key pathological mechanisms with clinical presentations you will encounter on the wards:
| Pathological event | Clinical consequence |
|---|---|
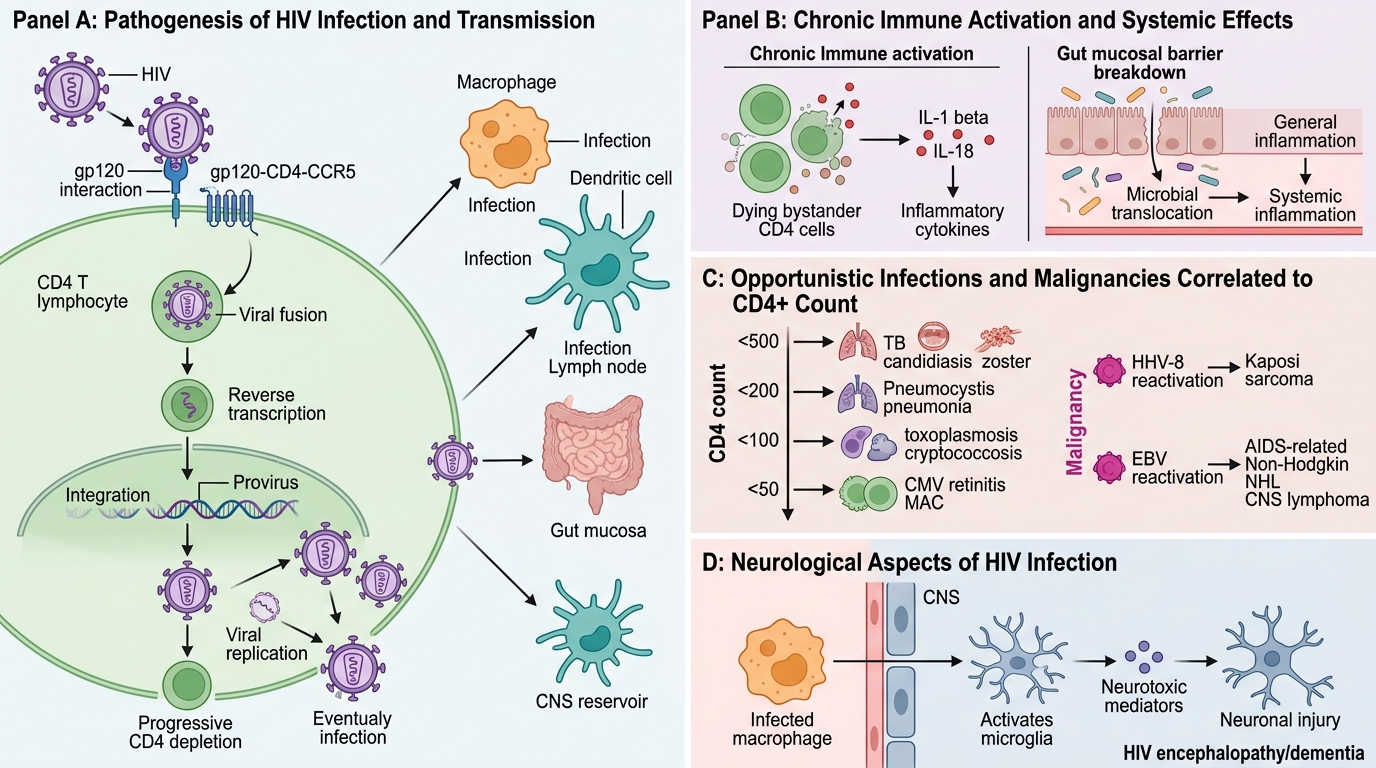
| gp120–CD4–CCR5 binding → CD4 depletion | Progressive immunosuppression, stage-specific OIs |
| Provirus integration into host chromatin | Lifelong infection; impossible to eradicate; ART suppresses, not cures |
| Macrophage/DC infection | Virus spreads to tissues; CNS reservoir established early |
| Pyroptosis-driven IL-1β/IL-18 release | Chronic immune activation, accelerated ageing phenotype |
| HHV-8 reactivation | Kaposi sarcoma |
| EBV reactivation | AIDS-NHL, CNS lymphoma |
| Microglial activation, neurotoxic mediators | HIV encephalopathy, dementia |
| Gut mucosal breakdown | Microbial translocation → chronic activation + wasting |
Key numbers for MCQ/clinical use:
• CD4 < 500: TB, oral candida, zoster
• CD4 < 200: PCP prophylaxis (co-trimoxazole); AIDS diagnosis threshold
• CD4 < 100: Toxoplasma, Cryptococcus, candida oesophagitis
• CD4 < 50: CMV retinitis, MAC