Page 5 of 22
PA8.3-5 | HLA, Transplantation, Autoimmunity & SLE — SDL Guide
Learning Objectives
- Describe the structure and function of MHC class I and class II molecules and explain how HLA typing governs transplant matching.
- Classify transplant rejection into hyperacute, acute, and chronic types; outline the mechanisms of each and of graft-versus-host disease.
- Define autoimmunity and explain how central and peripheral tolerance fail; enumerate organ-specific and systemic autoimmune diseases.
- Describe the pathogenesis of SLE including the roles of autoantibodies, immune-complex deposition, and complement consumption; correlate pathogenesis with multisystem clinical features and diagnostic criteria.
INSTRUCTIONS
The immune system must distinguish self from non-self precisely enough to destroy pathogens yet spare the body's own tissues. When this precision fails — whether during transplantation, where a foreign organ is recognised as enemy, or in autoimmunity, where self-tissue is mistakenly targeted — the clinical consequences can be devastating. Mastering HLA biology, rejection mechanisms, and autoimmune pathogenesis will let you reason through conditions from a kidney rejection to SLE to rheumatoid arthritis using a single, coherent framework.
References
- Robbins & Kumar Basic Pathology, 11th ed., Ch 5 (Diseases of the Immune System) (textbook)
- Harsh Mohan Textbook of Pathology, 7th ed., Ch 4 (Immunopathology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 42-year-old man receives a kidney transplant from his brother. Within 24 hours the transplanted kidney turns dusky and fails to produce urine — it is surgically removed within the day. Meanwhile, across the ward, a 28-year-old woman with joint pain, a facial rash, and foamy urine has an ANA titre of 1:640. Both patients share one underlying theme: their immune systems are attacking biological tissue that should not have been destroyed. What does the body use to tell friend from foe, and when does that system go wrong?
WHY THIS MATTERS
HLA typing and rejection mechanisms underpin all of transplant medicine — one of surgery's most remarkable achievements. Autoimmunity explains a wide spectrum of disorders you will encounter in every clinical posting: nephrology (lupus nephritis), rheumatology (SLE, RA), endocrinology (Hashimoto thyroiditis, Type 1 DM), neurology (myasthenia gravis), and gastroenterology (pernicious anaemia). PA8.3-8.5 form the mechanistic spine for the entire immunopathology block, and these concepts appear consistently in university and PG entrance examinations.
RECALL
Before going further, briefly recall:
• What is an antigen-presenting cell (APC), and what surface molecule does it use to present peptides?
• What is the difference between a T-helper (CD4+) and a cytotoxic T (CD8+) lymphocyte?
• What is the complement system, and which pathway does antigen–antibody complex activate?
• What are Type II and Type III hypersensitivity reactions?
If any of these feel shaky, revisit the previous SDL on Hypersensitivity before continuing.
The MHC / HLA System — Structure and Function
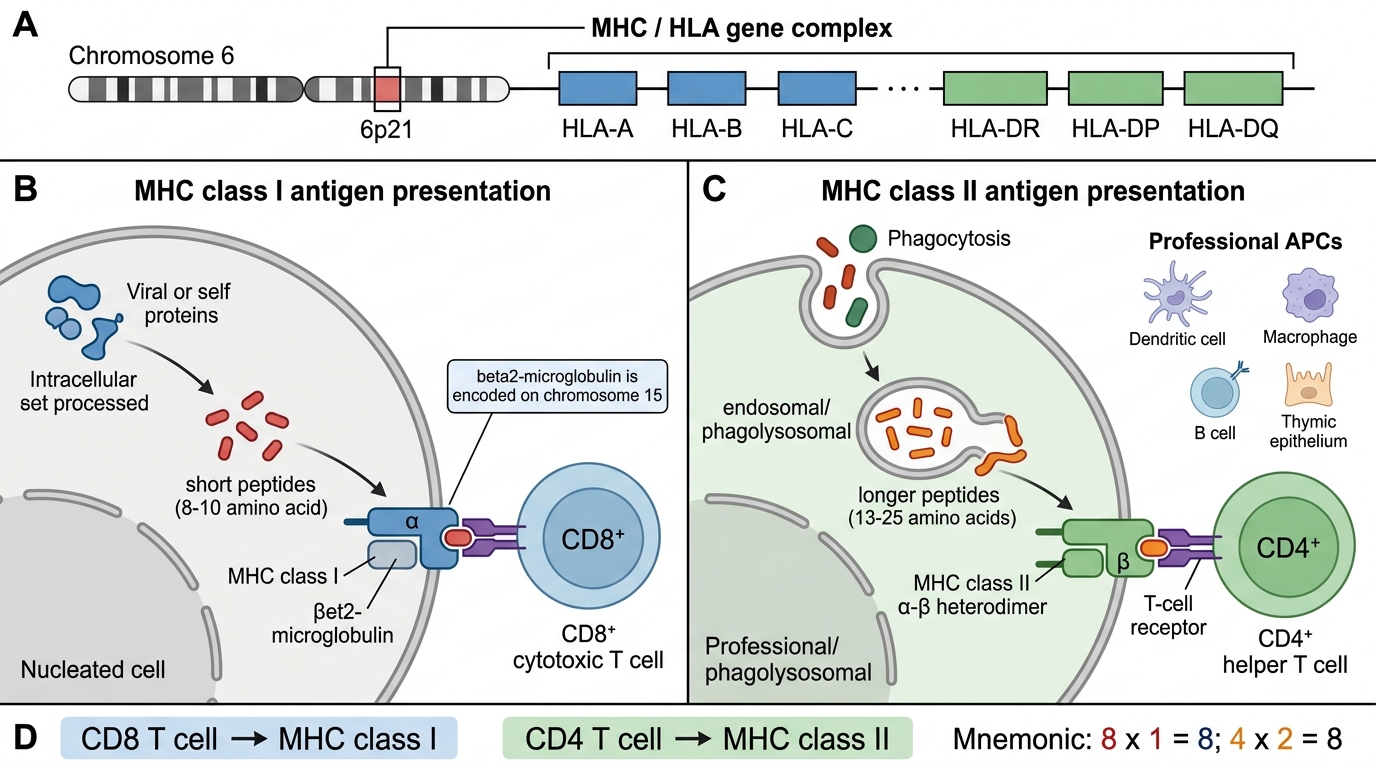
The major histocompatibility complex (MHC) is a cluster of genes on chromosome 6p21 that encodes cell-surface glycoproteins whose primary function is to display peptide fragments for T-lymphocyte surveillance. In humans these proteins are called human leukocyte antigens (HLA) because they were first identified on white blood cells.
There are two classes:
MHC class I (HLA-A, HLA-B, HLA-C)
• Expressed on virtually all nucleated cells.
• Structure: a heavy α-chain non-covalently associated with β₂-microglobulin (encoded outside the MHC on chromosome 15).
• Presents endogenous (intracellular) peptides — typically 8–10 amino acids — derived from self-proteins or viral/intracellular pathogens.
• Recognised by CD8+ cytotoxic T cells (CTLs).
• Function: allows CTLs to patrol for infected or malignant cells and destroy them.
MHC class II (HLA-DR, HLA-DP, HLA-DQ)
• Expressed only on professional APCs: dendritic cells, macrophages, B cells, and thymic epithelium.
• Structure: α- and β-chains forming a membrane-bound heterodimer.
• Presents exogenous (extracellular) peptides — 13–25 amino acids — from phagocytosed material.
• Recognised by CD4+ helper T cells (T_H).
• Function: orchestrates adaptive immune responses by activating helper T cells, which in turn stimulate B cells and macrophages.
IMPORTANT: CD8 T cells = class I; CD4 T cells = class II. A useful mnemonic: 8 × 1 = 8 (both single digits); 4 × 2 = 8 also, but remember CD4 responds to class II because there are two chains in the dimer.
IMPORTANT: The HLA locus is highly polymorphic — there are thousands of allelic variants at each locus across the human population. This diversity is the evolutionary reason pathogens cannot evade immunity in all individuals, but it is also why donor–recipient matching is challenging.
MHC / HLA System: Structure and Function
SELF-CHECK
Which HLA class presents exogenous antigens to CD4+ helper T cells?
A. HLA class I (HLA-A, B, C)
B. HLA class II (HLA-DR, DP, DQ)
C. Both class I and class II equally
D. Neither — CD4+ T cells are activated by B-cell receptors directly
Reveal Answer
Answer: B. HLA class II (HLA-DR, DP, DQ)
MHC class II molecules (HLA-DR, DP, DQ) are expressed on professional APCs and present exogenous peptides to CD4+ helper T cells. MHC class I presents endogenous peptides to CD8+ cytotoxic T cells.
HLA Typing, Disease Associations, and Transplant Matching
HLA Typing, Disease Associations, and Transplant Matching
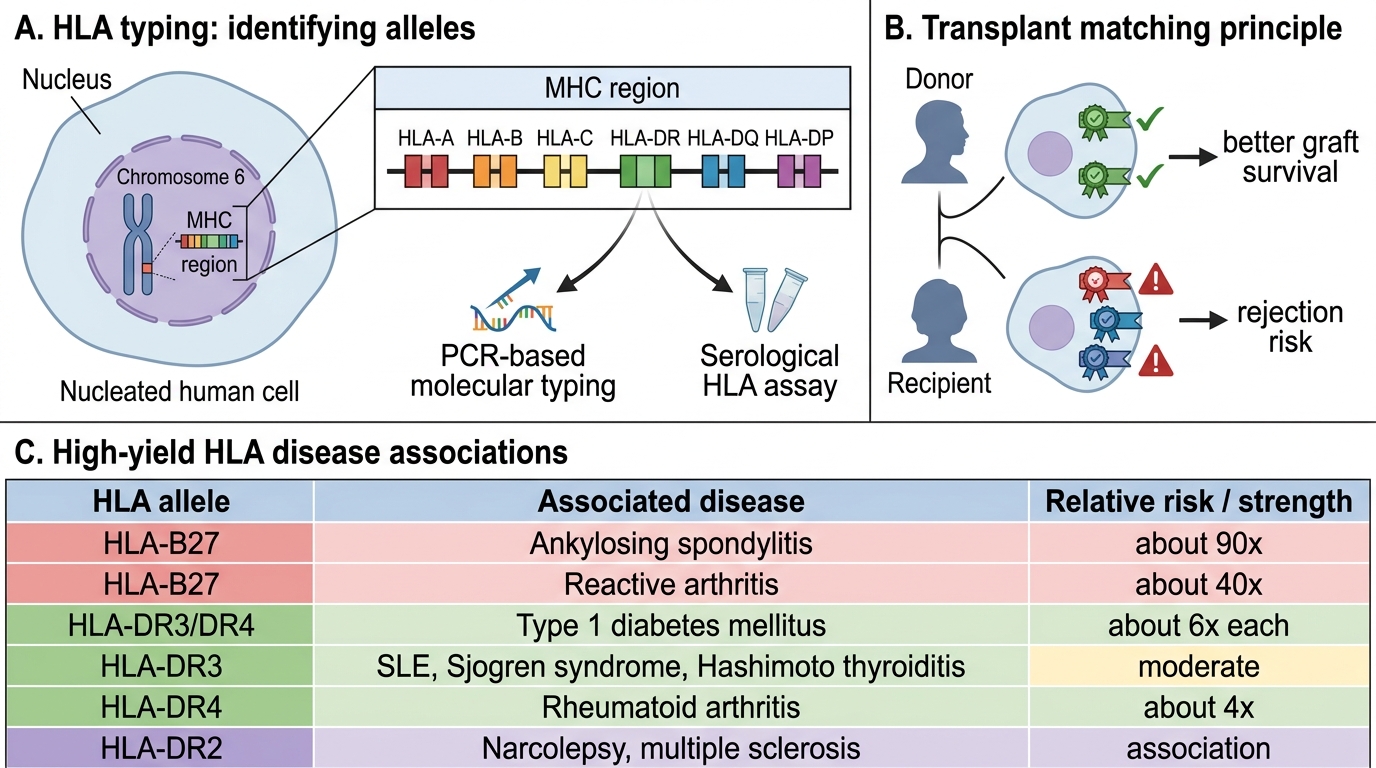
HLA typing determines the specific HLA alleles an individual carries at each locus. In transplantation, typing is done by molecular (PCR-based) methods and serological assays.
Key HLA–disease associations (for examination and clinical practice):
| HLA allele | Disease | Relative risk |
|---|---|---|
| HLA-B27 | Ankylosing spondylitis | ~90× |
| HLA-B27 | Reactive arthritis (Reiter syndrome) | ~40× |
| HLA-DR3/DR4 | Type 1 diabetes mellitus | ~6× each |
| HLA-DR3 | SLE, Sjögren syndrome, Hashimoto | Moderate |
| HLA-DR4 | Rheumatoid arthritis | ~4× |
| HLA-DR2 | Narcolepsy, multiple sclerosis | Variable |
The association does not imply causation; the HLA allele may present a self-peptide that triggers an autoreactive T-cell response, or the gene may be in linkage disequilibrium with the true causal variant.
Transplant matching principles:
• Ideally match at HLA-A, B, and DR loci (6-antigen match in kidney transplant scoring).
• A higher degree of mismatch → greater alloreactive T-cell and antibody response → higher rejection risk.
• Crossmatch test: recipient serum is tested against donor lymphocytes. A positive crossmatch (recipient has pre-formed anti-donor HLA antibodies) predicts hyperacute rejection → transplant is contraindicated.
• Blood-group (ABO) compatibility is mandatory in addition to HLA matching.
• Identical twins: zero MHC mismatch, no immunosuppression needed (syngeneic graft).
• Related donors (e.g., siblings): ~25% chance of HLA identity (one haplotype inherited per parent from a pool of 4 combinations).
Transplant Rejection — Hyperacute, Acute, and Chronic
Rejection occurs when the recipient's immune system recognises the graft as foreign. There are three distinct types, each with a different mechanism and time course.
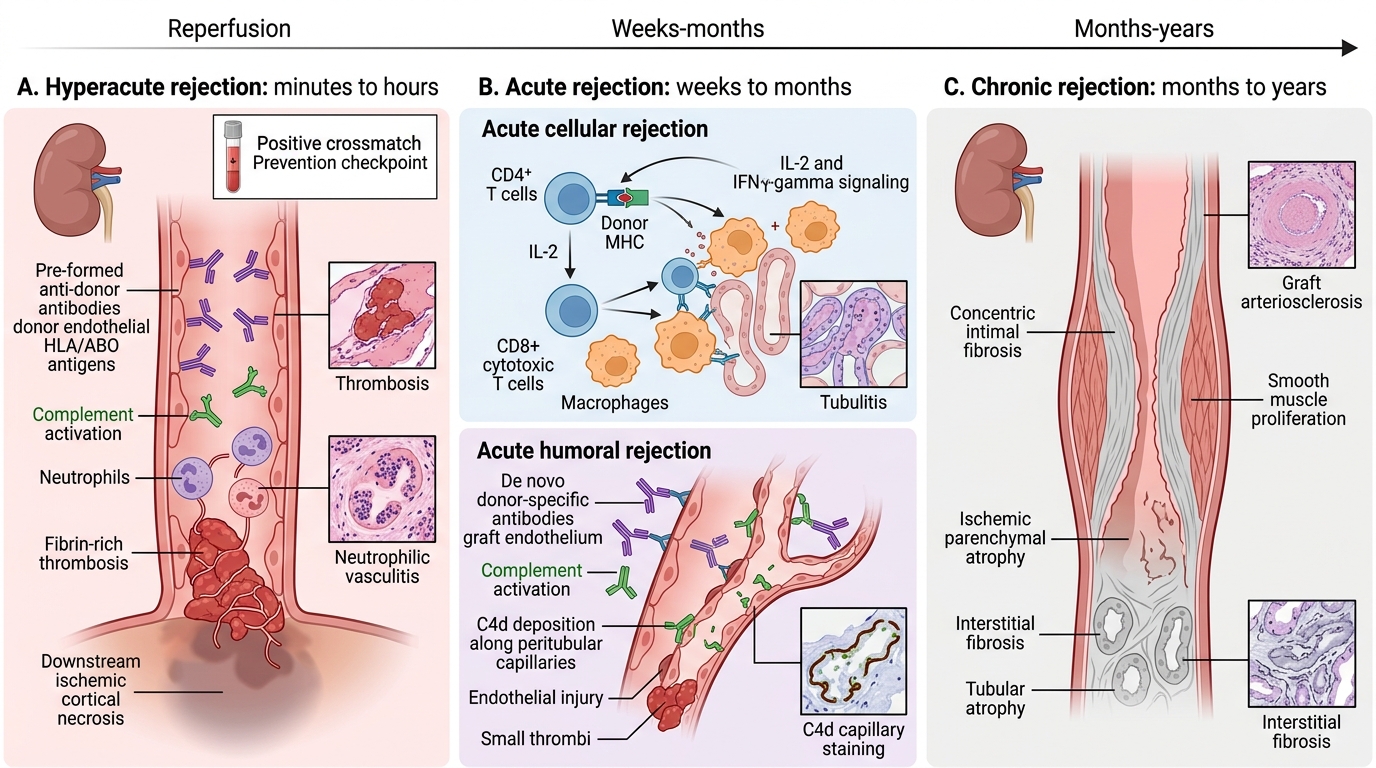
1. Hyperacute rejection
• Timing: Minutes to hours after reperfusion.
• Mechanism: Recipient has pre-formed circulating antibodies against donor HLA or ABO antigens (from prior blood transfusions, pregnancies, or failed transplants). These antibodies bind donor endothelial antigens → activate complement → trigger thrombosis within graft vessels → ischaemic necrosis.
• Histology: Widespread thrombosis, neutrophilic vasculitis, ischaemic cortical necrosis (in kidney).
• Prevention: Crossmatch testing before transplant.
• Treatment: None effective; graft must be removed.
2. Acute rejection
Occurs weeks to months post-transplant (or later if immunosuppression is reduced).
Acute cellular (T-cell-mediated) rejection:
• CD4+ T cells recognise donor MHC class II (directly or via recipient APCs presenting processed donor peptides — indirect pathway) → secrete IL-2, IFN-γ → activate CD8+ CTLs and macrophages → graft tubulitis, interstitial infiltrate.
Acute humoral (antibody-mediated) rejection:
• De novo donor-specific antibodies (DSA) bind donor endothelium → complement activation (C4d deposition is a marker) → endothelial injury, intravascular thrombosis.
3. Chronic rejection (chronic allograft dysfunction)
• Timing: Months to years.
• Mechanism: Persistent low-grade immune injury (both cellular and humoral) + ischaemia + drug toxicity → TGF-β-driven fibrosis and intimal smooth-muscle proliferation (transplant arteriopathy) → progressive vascular occlusion → graft fibrosis.
• Histology (kidney): Interstitial fibrosis, tubular atrophy, arterial intimal thickening (onion-skin pattern), glomerulosclerosis.
• Treatment: No specific therapy; the dominant cause of late graft loss.
Graft-versus-host disease (GVHD)
• Occurs in haematopoietic stem cell (bone marrow) transplants, NOT solid organ transplants.
• Donor T cells (the graft) attack the recipient's (host's) tissues — liver, skin, gut.
• Acute GVHD: within 100 days — maculopapular rash, cholestatic jaundice, bloody diarrhoea.
• Chronic GVHD: after 100 days — fibrosis of skin, liver, lung (resembles autoimmune disease).
Types of Transplant Rejection
SELF-CHECK
A kidney transplant recipient develops rising creatinine on day 10. Biopsy shows dense interstitial lymphocytic infiltrate and tubulitis. C4d staining is negative. What is the most likely diagnosis?
A. Hyperacute rejection due to preformed antibodies
B. Acute cellular (T-cell-mediated) rejection
C. Chronic rejection with transplant arteriopathy
D. Calcineurin inhibitor nephrotoxicity
Reveal Answer
Answer: B. Acute cellular (T-cell-mediated) rejection
Interstitial lymphocytic infiltrate and tubulitis on day 10, with negative C4d, is the classic histological picture of acute cellular (T-cell-mediated) rejection. Hyperacute rejection occurs within minutes to hours. Chronic rejection takes months to years. C4d positivity would indicate the antibody-mediated form.
CLINICAL PEARL
C4d is a split product of complement that covalently binds to peritubular capillary endothelium and persists even after the complement cascade has resolved. Positive C4d staining on biopsy is therefore a footprint of antibody-mediated (humoral) rejection — even if the acute episode is over. In practice, C4d positivity plus donor-specific antibodies in serum plus histological changes = antibody-mediated rejection (Banff classification criterion).