Page 7 of 22
PA8.3-5 | HLA, Transplantation, Autoimmunity & SLE — SDL Guide (Part 3)
SLE — Multisystem Clinical Features and Diagnosis
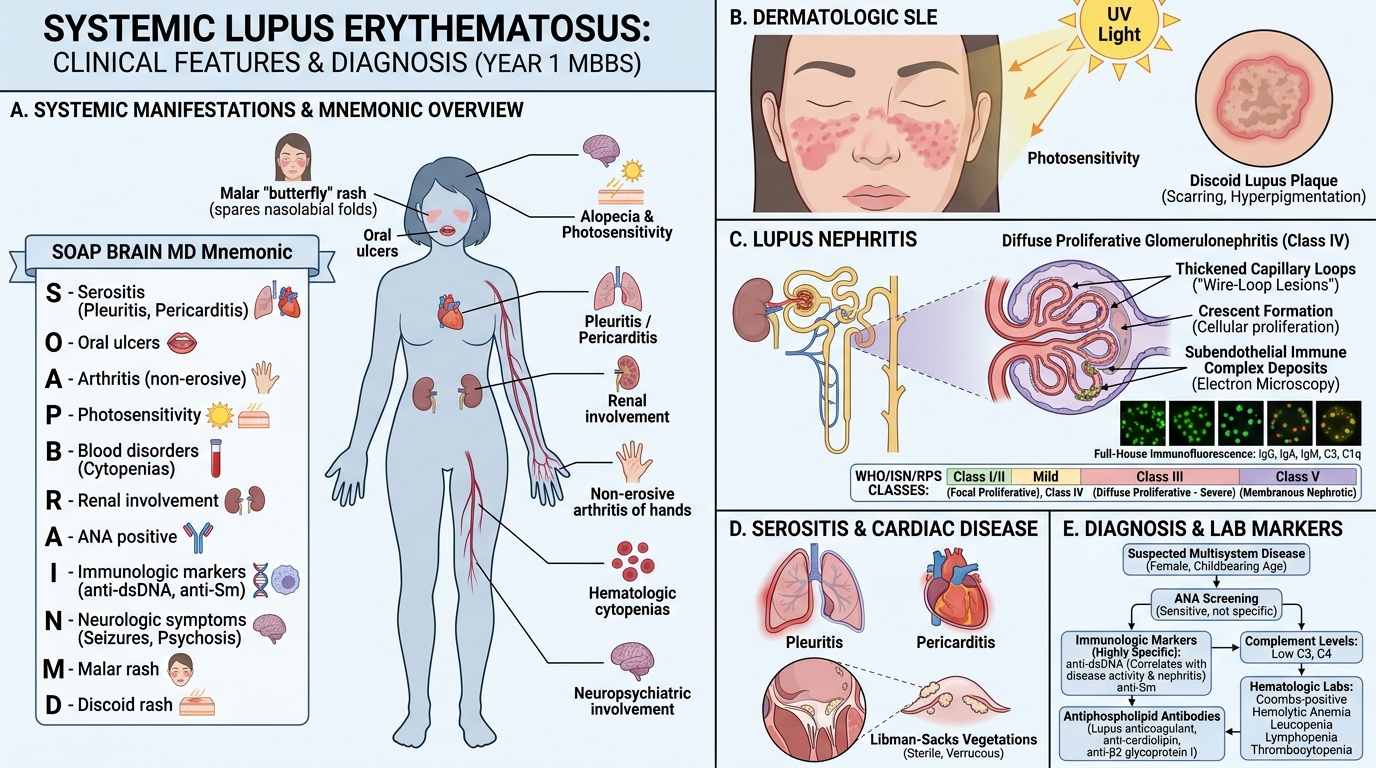
SLE predominantly affects women of childbearing age (F:M = 9:1). It is characterised by remissions and flares. The classic mnemonic for organ involvement is SOAP BRAIN MD (Serositis, Oral ulcers, Arthritis, Photosensitivity, Blood disorders, Renal, ANA, Immunologic markers, Neuropsychiatric, Malar rash, Discoid rash).
Key organ manifestations:
Skin:
• Malar (butterfly) rash — erythema over cheeks and nose bridge, sparing nasolabial folds; triggered by UV exposure.
• Discoid lupus — scarring, hyperpigmented plaques.
• Photosensitivity, oral ulcers, alopecia.
Joints:
• Non-erosive arthritis/arthralgia — most common feature; synovitis without joint destruction (unlike RA).
Kidneys — Lupus nephritis (WHO/ISN classification):
• Class I/II: minimal or mesangial — mild, often asymptomatic.
• Class III (focal proliferative) and Class IV (diffuse proliferative) — most severe; crescentic GN, nephrotic + nephritic syndrome, wire-loop lesions on EM (subendothelial deposits), full-house IF pattern (IgG, IgA, IgM, C3, C1q).
• Class V: membranous — nephrotic syndrome.
• Wire-loop lesions on light microscopy are characteristic of Class IV (thickened glomerular capillary walls due to large subendothelial immune complex deposits).
Serositis: Pleuritis, pericarditis (Libman–Sacks endocarditis — sterile verrucous vegetations on valve leaflets, pathognomonic).
Haematologic: Haemolytic anaemia (Coombs+), leucopenia, lymphopenia, thrombocytopenia.
Neuropsychiatric SLE: Psychosis, seizures, cranial neuropathies (from vasculitis or antiphospholipid antibody-related thrombosis).
Laboratory investigations:
• ANA (antinuclear antibody) — screening test; positive in >95% of SLE but not specific (also positive in other CTDs, drugs, healthy individuals at low titre).
• Anti-dsDNA — titre correlates with disease activity; marker of nephritis risk.
• Anti-Sm — highly specific, less sensitive.
• Complement levels (C3, C4, CH50) — consumed during active disease → fall in active SLE; monitoring C3/C4 tracks flares.
• LE cell — neutrophil that has phagocytosed an opsonised nuclear material (anti-histone antibody coated nucleus); historically important but replaced by ANA testing.
• Urinalysis: proteinuria, RBC casts (indicate nephritis).
Diagnostic approach: The 2019 EULAR/ACR classification criteria use a scoring system across domains (ANA as entry criterion + weighted points for clinical and immunological features, total ≥10 = SLE). Know the concept rather than memorising all point values for undergraduate purposes.
Systemic Lupus Erythematosus: Multisystem Features and Diagnosis
SELF-CHECK
Which of the following serology findings is MOST SPECIFIC for the diagnosis of SLE?
A. Positive ANA at titre 1:160
B. Elevated ESR and CRP
C. Anti-dsDNA and anti-Sm antibodies
D. Reduced serum complement C3 and C4
Reveal Answer
Answer: C. Anti-dsDNA and anti-Sm antibodies
Anti-dsDNA and anti-Sm antibodies are the most specific markers for SLE. ANA is sensitive but non-specific (positive in many other conditions). Elevated ESR/CRP occur in any inflammatory state. Reduced C3/C4 reflects active disease and complement consumption but is not specific to SLE.
CLINICAL PEARL
In the USMLE and Indian PG entrance examinations, the following SLE associations are high-yield:
• Wire-loop lesions = Class IV diffuse proliferative lupus nephritis (worst prognosis; treat aggressively).
• Libman–Sacks endocarditis = non-infective, can be on either valve surface (unlike rheumatic fever which is on atrial surface of mitral valve).
• Drug-induced lupus = anti-histone antibodies; caused by procainamide, hydralazine, isoniazid, minocycline; spares kidneys and CNS; resolves on drug withdrawal.
• Neonatal lupus = maternal anti-Ro (SSA) antibodies cross placenta → congenital heart block in neonate.
Immunosuppression in Transplantation — Key Principles
Immunosuppression in Transplantation: Key Targets and Clinical Balance
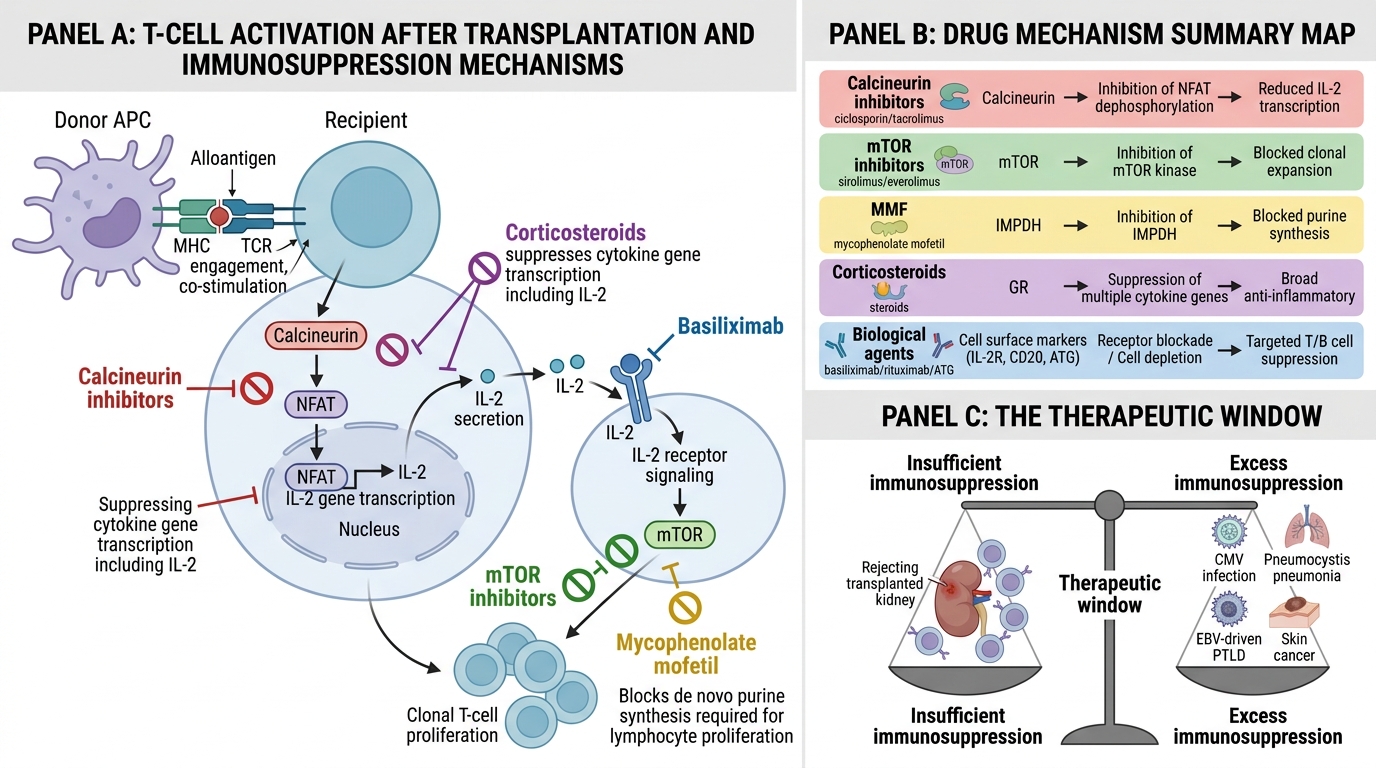
Immunosuppressive therapy is essential in all solid organ transplants to prevent rejection. The principal drugs act at different steps of T-cell activation:
- Calcineurin inhibitors (ciclosporin, tacrolimus) — inhibit calcineurin → block NFAT transcription factor → suppress IL-2 gene expression → prevent T-cell proliferation. Main side effects: nephrotoxicity, hypertension, diabetes (tacrolimus), gingival hyperplasia + hirsutism (ciclosporin).
- mTOR inhibitors (sirolimus, everolimus) — block mTOR → inhibit IL-2-driven T-cell clonal expansion; also anti-proliferative for endothelial cells (useful in chronic rejection).
- Mycophenolate mofetil (MMF) — inhibits inosine monophosphate dehydrogenase → blocks de novo purine synthesis → selective inhibition of lymphocyte proliferation (lymphocytes depend more on de novo pathway than other cells).
- Corticosteroids — broad anti-inflammatory; suppress cytokine gene transcription; used as induction and rescue therapy in acute rejection.
- Biological agents — anti-IL-2 receptor (basiliximab) for induction; anti-CD20 (rituximab) for antibody-mediated rejection; anti-thymocyte globulin (ATG) for severe acute rejection.
Balance: insufficient immunosuppression → rejection; excess → opportunistic infections (CMV, Pneumocystis), post-transplant lymphoproliferative disorder (PTLD, driven by EBV), and skin cancers.
SELF-CHECK
Tacrolimus exerts its immunosuppressive effect primarily by:
A. Blocking purine synthesis and inhibiting lymphocyte proliferation
B. Inhibiting calcineurin, thereby preventing IL-2 transcription
C. Targeting mTOR to block IL-2-driven T-cell clonal expansion
D. Depleting CD20-positive B cells via antibody-dependent cytotoxicity
Reveal Answer
Answer: B. Inhibiting calcineurin, thereby preventing IL-2 transcription
Tacrolimus (like ciclosporin) is a calcineurin inhibitor. By blocking calcineurin, it prevents dephosphorylation of NFAT, so the transcription factor cannot enter the nucleus, and IL-2 gene expression is suppressed — halting T-cell proliferation. MMF blocks purine synthesis; sirolimus targets mTOR; rituximab depletes CD20+ B cells.