Page 1 of 22
PA8.1-2 | Immunity & Hypersensitivity Reactions — SDL Guide
Learning Objectives
- Describe the components and mechanisms of innate and adaptive immunity
- Explain antigen presentation via MHC class I and II molecules
- Distinguish primary from secondary immune responses
- Classify hypersensitivity reactions using the Gell & Coombs system (Types I–IV)
- Describe the pathological mechanisms and clinical examples of each hypersensitivity type
- Compare the four types of hypersensitivity reactions in terms of mediator, mechanism, timing, and representative diseases
INSTRUCTIONS
Almost every organ-system disease you will encounter in clinical years has an immune component — whether it is a protective response gone right (clearing infection) or a hypersensitivity reaction gone wrong (destroying host tissue). This module builds the conceptual scaffold that links basic immunology to disease. Mastering the Gell & Coombs classification now will let you instantly categorise the mechanism of autoimmune, allergic, and transplant-rejection disorders you will study in every organ block.
References
- Robbins & Kumar: Basic Pathology, 11th ed., Ch 5 — Diseases of the Immune System (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch 3 — Immunopathology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old medical student eats a peanut-based snack at a canteen and within 10 minutes develops generalised urticaria, wheezing, and hypotension. Her friend, who has systemic lupus erythematosus (SLE), asks: "My disease is also immune-mediated — are they the same mechanism?" They are not. Both are hypersensitivity reactions — but they operate through entirely different arms of the immune system, different timescales, and different tissue targets. By the end of this module you will be able to explain exactly why these two patients have such different presentations, and place them precisely on the Gell & Coombs classification.
WHY THIS MATTERS
Hypersensitivity mechanisms underlie a striking proportion of Year-2 and clinical-year pathology — allergic asthma, autoimmune haemolytic anaemia, SLE, Goodpasture disease, myasthenia gravis, Graves disease, contact dermatitis, granulomatous diseases, and transplant rejection all map to one of four mechanistic types. Once the classification is internalised, a mechanistic diagnosis ("this is a Type II antibody-mediated reaction") precedes and predicts the histology, the serology, and the treatment strategy.
RECALL
From Year-1 Physiology and Biochemistry, you should be comfortable with:
• Immunoglobulin classes — IgG, IgM, IgA, IgD, IgE and their basic properties
• Complement system — classical vs alternative vs lectin pathways; C3a/C5a as anaphylatoxins
• T-cell and B-cell lineages — thymic education, clonal selection, affinity maturation
• MHC molecules — Class I on all nucleated cells; Class II on antigen-presenting cells
• Cytokines as signalling molecules — concept of autocrine/paracrine/endocrine action
If any of these feel unfamiliar, a 10-minute review of your Year-1 notes before proceeding will pay dividends.
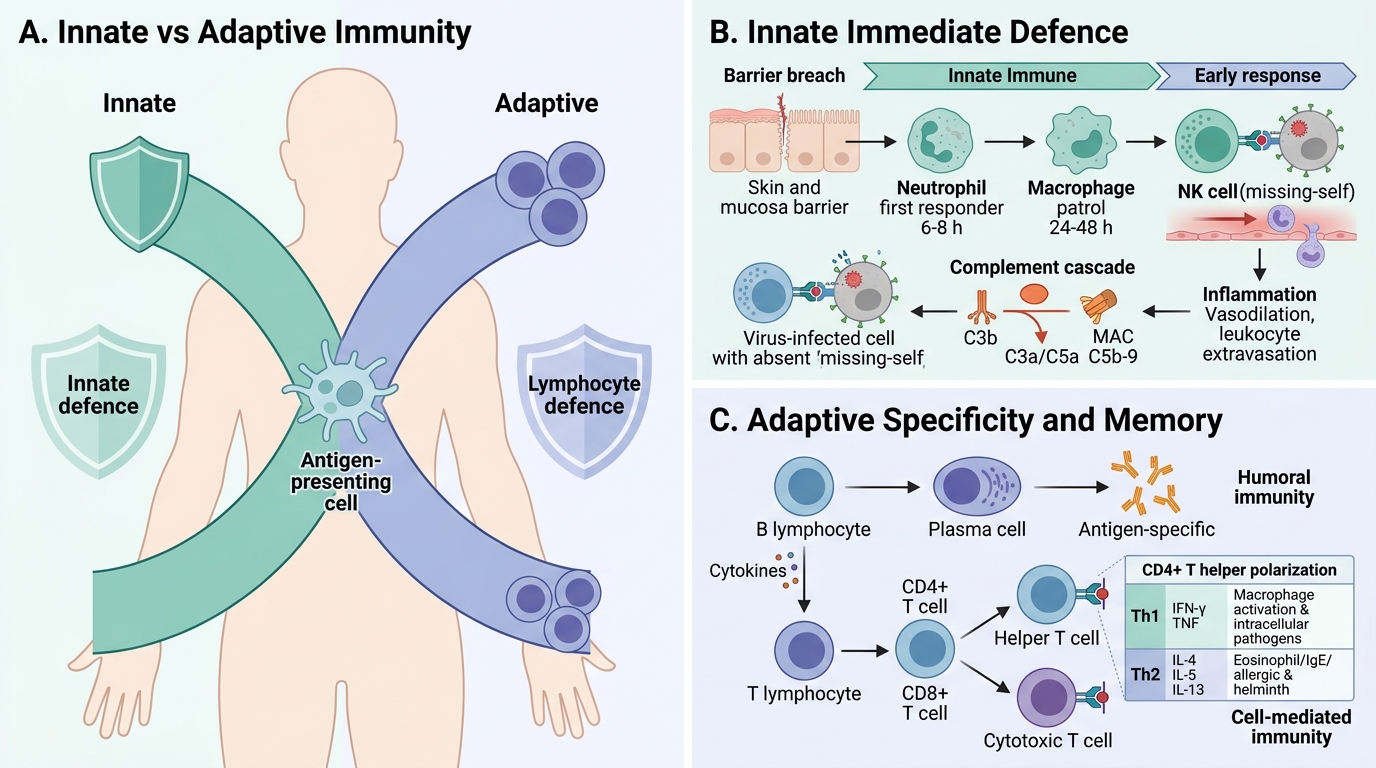
Overview of the Immune System: Innate vs Adaptive
The immune system operates through two overlapping arms that differ in speed, specificity, and memory.
Innate immunity provides immediate, non-specific defence. Its components include:
• Physical barriers — intact skin and mucosae, mucociliary clearance, gastric acid
• Phagocytes — neutrophils (first responders, 6–8 h) and macrophages (patrol, 24–48 h)
• Natural killer (NK) cells — kill virus-infected and tumour cells without prior sensitization; recognise absence of MHC I ("missing-self" hypothesis)
• Complement system — generates opsonins (C3b), anaphylatoxins (C3a, C5a), and the membrane attack complex (MAC, C5b-9)
• Inflammation — the vascular and cellular response that concentrates effectors at the injury site
Adaptive immunity develops over days but is exquisitely specific and generates immunological memory:
• Humoral branch — B lymphocytes differentiate into plasma cells that secrete antigen-specific antibodies
• Cell-mediated branch — T lymphocytes (CD4⁺ helper and CD8⁺ cytotoxic) recognise peptide–MHC complexes
CD4⁺ T helper cells polarise into functional subsets depending on the cytokine milieu:
| Subset | Key cytokines produced | Main function |
|---|---|---|
| Th1 | IFN-γ, TNF | Macrophage activation; intracellular pathogens |
| Th2 | IL-4, IL-5, IL-13 | B-cell help; IgE class switching; eosinophils; allergy |
| Th17 | IL-17, IL-22 | Neutrophil recruitment; extracellular fungi/bacteria |
| Treg | IL-10, TGF-β | Peripheral tolerance; suppress excess responses |
CD8⁺ cytotoxic T lymphocytes (CTL) kill target cells via perforin/granzyme and Fas–FasL pathways. They recognise peptides presented on MHC class I (expressed on all nucleated cells).
Innate and Adaptive Immunity Overview
Antigen Presentation and the Immune Response
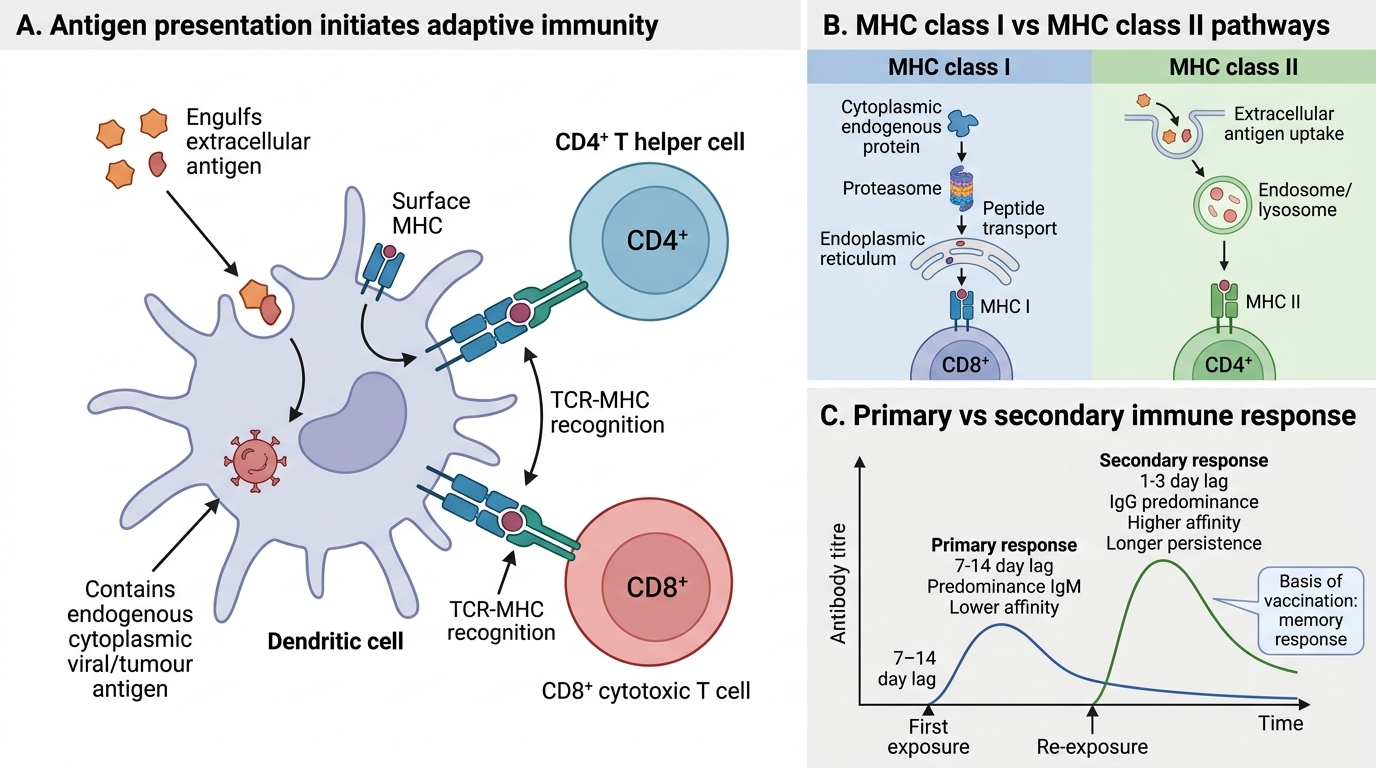
Antigen Presentation and Adaptive Immune Response
Adaptive immunity is initiated when antigen-presenting cells (APCs) — primarily dendritic cells, but also macrophages and B cells — process and display peptide fragments to T lymphocytes.
MHC class I (HLA-A, -B, -C):
• Expressed on all nucleated cells
• Presents endogenous peptides (cytoplasmic — e.g., viral proteins, tumour antigens)
• Recognised by CD8⁺ T cells → CTL activation
MHC class II (HLA-DR, -DP, -DQ):
• Expressed on professional APCs (dendritic cells, macrophages, B cells) — can be upregulated on other cells by IFN-γ
• Presents exogenous peptides (endosomal — e.g., bacteria, ingested antigen)
• Recognised by CD4⁺ T helper cells → lymphokine secretion, B-cell help
Primary vs secondary immune response:
• Primary response — first exposure; 7–14 day lag; IgM predominates; lower titre; lower affinity (no affinity maturation yet)
• Secondary (anamnestic) response — re-exposure; 1–3 day lag; IgG predominates; higher titre; higher affinity; persists longer. This is the principle exploited by vaccination.
SELF-CHECK
A patient with HIV has a CD4 count of 50 cells/μL. A viral peptide from cytomegalovirus (CMV) is processed inside a dendritic cell. Which MHC molecule presents this peptide, and to which T-cell subset?
A. MHC class I → CD8⁺ cytotoxic T cell
B. MHC class II → CD4⁺ helper T cell
C. MHC class I → CD4⁺ helper T cell
D. MHC class II → CD8⁺ cytotoxic T cell
Reveal Answer
Answer: B. MHC class II → CD4⁺ helper T cell
CMV is processed exogenously within the endosomal pathway of the dendritic cell and presented on MHC class II to CD4⁺ T helper cells. (Endogenous/cytoplasmic peptides — e.g., from virus replicating inside the APC itself — would use MHC class I → CD8⁺.) The clinical corollary: with a CD4 count of 50, this patient cannot mount an adequate helper response, explaining reactivation of opportunistic infections like CMV retinitis.
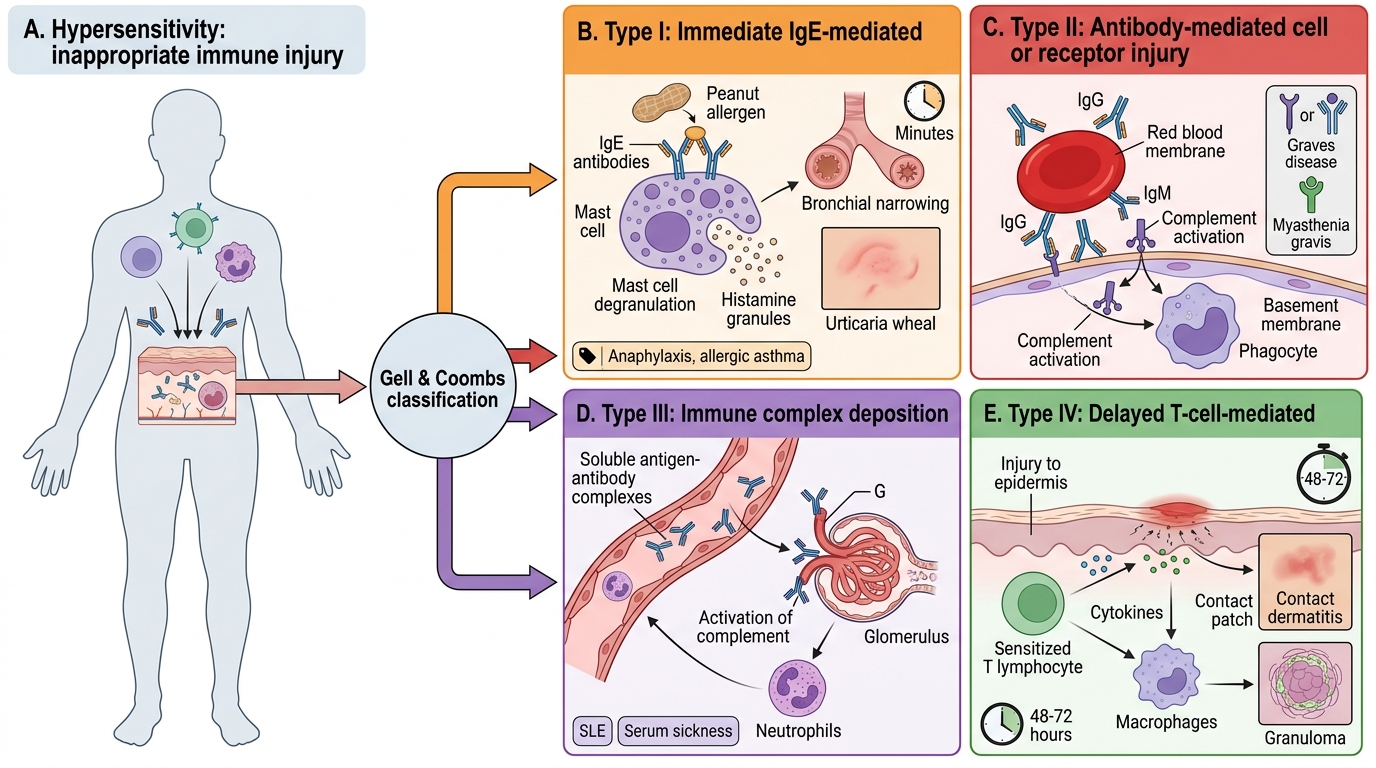
Introduction to Hypersensitivity — The Gell & Coombs Classification
Hypersensitivity is tissue-damaging or functionally disruptive immune reactivity — an immune response that, instead of protecting, causes pathology. The Gell & Coombs classification (1963) organises these reactions into four types based on the effector mechanism rather than the antigen:
| Type | Name | Mediator | Onset | Prototypic Example |
|---|---|---|---|---|
| I | Immediate / Anaphylactic | IgE + mast cells | Minutes | Anaphylaxis, atopy |
| II | Antibody-mediated / Cytotoxic | IgG/IgM vs cell-surface antigens | Hours | Autoimmune haemolytic anaemia |
| III | Immune-complex | IgG/IgM antigen-antibody complexes | Hours–days | SLE, serum sickness |
| IV | Delayed / Cell-mediated | T lymphocytes (no antibody) | 48–72 h | TB granuloma, contact dermatitis |
Types I–III are antibody-mediated; Type IV is purely T-cell-mediated (hence "delayed" — cellular responses take longer to mobilise than pre-formed antibody).
Gell & Coombs Classification of Hypersensitivity