Page 3 of 22
PA8.1-2 | Immunity & Hypersensitivity Reactions — SDL Guide (Part 3)
Type IV Hypersensitivity — Delayed/Cell-Mediated
Type IV Hypersensitivity: Delayed T-Cell Mediated Injury
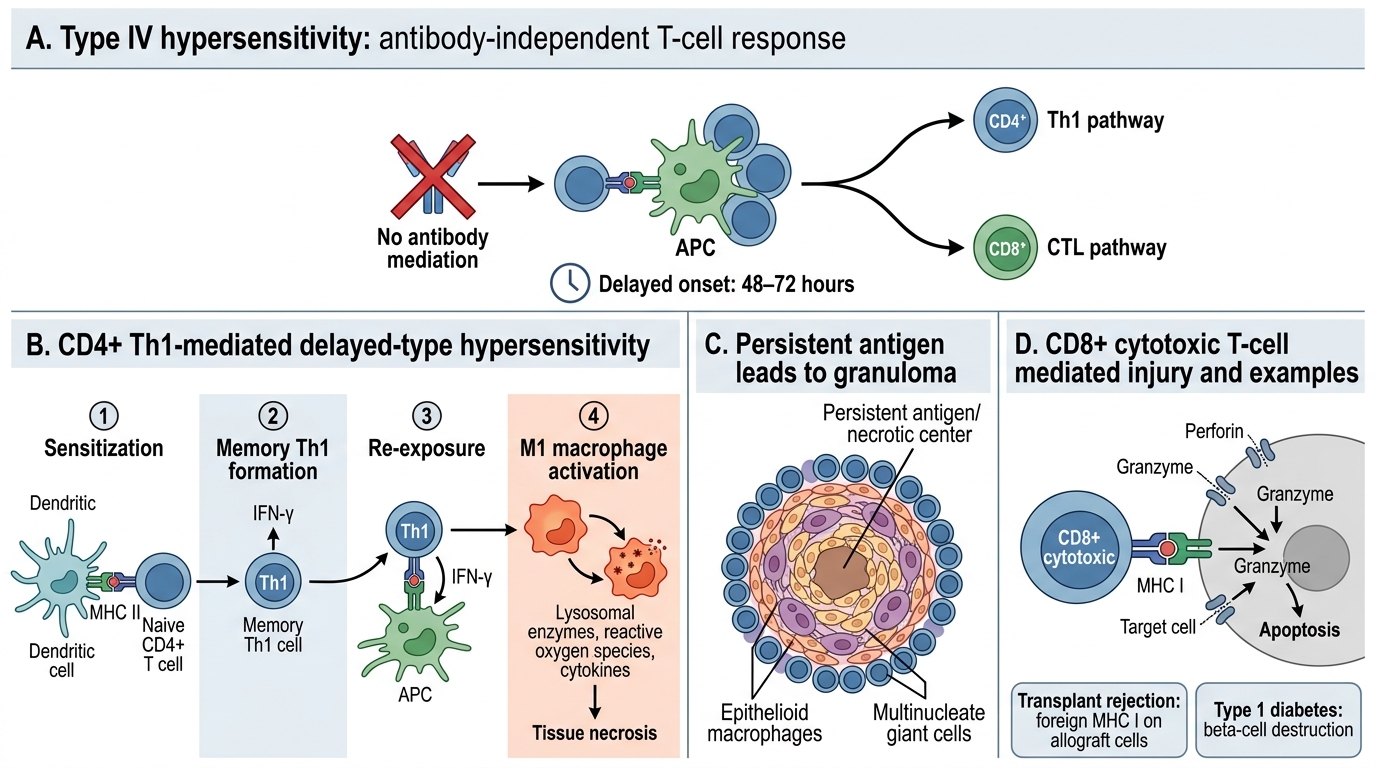
Type IV is the only hypersensitivity type that is antibody-independent — it is mediated entirely by T lymphocytes. It is called "delayed" because it takes 48–72 hours to develop (time required to recruit and activate antigen-specific T cells and macrophages).
Two major subtypes:
A. CD4⁺ T helper–mediated (Th1-driven, "classical" delayed-type hypersensitivity — DTH):
1. Sensitization: First antigen exposure → dendritic cells present via MHC II → naive CD4⁺ T cells differentiate into Th1 memory cells (IFN-γ producers)
2. Elicitation: Re-exposure → Th1 cells recognise antigen on local APCs → secrete IFN-γ → macrophage activation (classical activation: M1 phenotype)
3. Tissue damage: Activated macrophages release lysosomal enzymes, reactive oxygen species, and cytokines → tissue necrosis
4. Persistence: Inability to clear antigen → granuloma formation (epithelioid macrophages + multinucleate giant cells + rim of lymphocytes)
B. CD8⁺ cytotoxic T lymphocyte (CTL)–mediated:
1. CD8⁺ T cells recognise antigen on MHC class I of target cells
2. Release perforin/granzymes → direct killing of target cell
3. Examples: Transplant rejection (allograft cells display foreign MHC I), type 1 diabetes (CTL destroy pancreatic β cells)
Clinical examples of Type IV:
| Disease | Antigen | Key mechanism |
|---|---|---|
| Tuberculin (Mantoux) test | PPD (mycobacterial protein) | CD4 Th1 → macrophage activation; induration at 48–72 h |
| Contact dermatitis | Haptens (nickel, poison ivy/urushiol, latex) | Hapten binds skin proteins; CD8 + CD4 response; vesicular rash |
| Tuberculosis granuloma | Mycobacterium tuberculosis (not cleared) | Persistent Th1 → macrophage activation → caseous necrosis granuloma |
| Transplant rejection (acute cell-mediated) | Allogeneic MHC | CD8⁺ CTL + CD4⁺ Th1 → graft cell destruction |
| Type 1 diabetes mellitus | Islet β-cell antigens (GAD, IA-2) | CD8⁺ CTL → β-cell destruction → absolute insulin deficiency |
| Crohn disease | Luminal microbial antigens | Th1/Th17 granulomatous transmural inflammation |
Why 48–72 hours? Pre-formed antibody acts within minutes to hours (Types I–III). T-cell–mediated responses require antigen recognition, T-cell mobilisation, and cytokine-driven macrophage recruitment from bone marrow — this cellular cascade is inherently slower.
SELF-CHECK
A nurse who had BCG vaccination as a child has a Mantoux (tuberculin) test placed. She returns 72 hours later and has a firm, indurated area of 18 mm. This reaction is BEST described as:
A. Type I — IgE-mediated mast cell response to PPD antigen
B. Type II — IgG-mediated cytotoxic destruction of dermal cells
C. Type IV — CD4⁺ Th1 memory cell activation and macrophage-mediated induration
D. Type III — immune complex deposition in the dermis causing vasculitis
Reveal Answer
Answer: C. Type IV — CD4⁺ Th1 memory cell activation and macrophage-mediated induration
The Mantoux test is the textbook example of Type IV (delayed-type) hypersensitivity. PPD antigens are presented via MHC class II to CD4⁺ Th1 memory cells (created during BCG vaccination or prior TB exposure). Over 48–72 hours, Th1 cells release IFN-γ, activating macrophages that accumulate at the site, producing the firm induration (not just erythema). The firmness distinguishes DTH (cellular infiltrate + fibrosis) from the transient wheal-and-flare of Type I (which resolves in < 1 hour).
Comparison of the Four Hypersensitivity Types
Four Types of Hypersensitivity Reactions
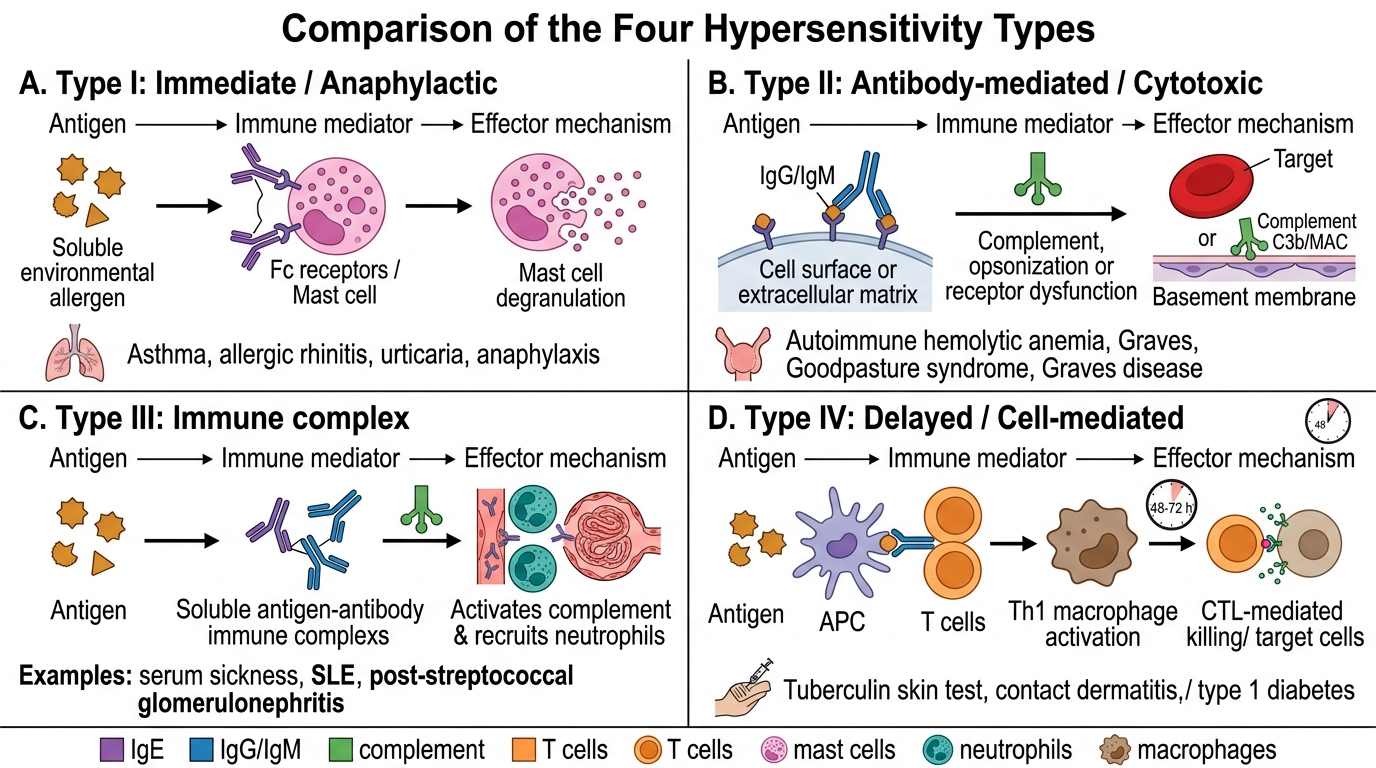
| Feature | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|
| Alternate name | Immediate / Anaphylactic | Antibody-mediated / Cytotoxic | Immune complex | Delayed / Cell-mediated |
| Mediator | IgE | IgG, IgM | IgG, IgM | T cells (Th1, CTL) |
| Antigen location | Soluble environmental | Cell surface / ECM | Soluble, in circulation | Intracellular / cell surface |
| Effector mechanism | Mast cell degranulation | Opsonization, lysis, receptor dysfunction | IC deposition → complement → neutrophil | Th1 → macrophage activation; CTL → cytotoxicity |
| Key mediators | Histamine, leukotrienes | Complement, ADCC | Complement (C3a, C5a), neutrophil enzymes | IFN-γ, TNF, perforin/granzymes |
| Onset | Minutes (early); 4–8 h (late) | Hours | Hours–days | 48–72 hours |
| Prototypic examples | Anaphylaxis, asthma, atopy | AIHA, Graves, MG, Goodpasture | SLE, serum sickness, post-strep GN | TB, contact dermatitis, transplant rejection |
| Transfer via | Serum (IgE) | Serum (IgG/IgM) | Serum (IC) | Cells (T cells) |
| Complement involved? | Yes (minor — C3a, C5a) | Yes (major — MAC + opsonins) | Yes (major — C3a, C5a) | No |
| Histological pattern | Eosinophils, mucosal oedema | Variable; specific (e.g., haemolysis) | Neutrophilic vasculitis, granular IF | Mononuclear cells, granulomas (Type IV-A) |