Page 10 of 20
PA12.1-3 | Environmental & Nutritional Diseases — SDL Guide
Learning Objectives
- Explain the pathological mechanisms by which air pollution and tobacco cause respiratory, cardiovascular, and oncological disease (PA12.1)
- Distinguish kwashiorkor from marasmus based on pathophysiology, clinical features, and morphological changes; describe the major vitamin deficiency disorders (PA12.2)
- Define obesity and metabolic syndrome, outline the role of adipokines and insulin resistance in their pathogenesis, and enumerate systemic consequences (PA12.3)
INSTRUCTIONS
Environmental and nutritional diseases account for a disproportionate share of preventable mortality worldwide — tobacco alone kills ~8 million people annually and kwashiorkor remains a major cause of under-5 deaths in low-income regions. For a Year-2 pathologist-in-training, understanding the morphological and biochemical bridges between exposure and disease is the foundation of both clinical diagnosis and public-health reasoning. This module covers three tightly linked domains: pollution and tobacco toxicity, protein-calorie and vitamin deficiency, and the obesity–metabolic syndrome axis.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 9 (Environmental and Nutritional Diseases) (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 10 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old retired coal-miner presents with progressive breathlessness, a barrel chest, and a 35-pack-year smoking history. Chest X-ray shows bilateral upper-lobe opacities and hyperinflated lungs. His 7-year-old granddaughter in the same household is brought in separately — she has oedematous legs, sparse reddish hair, and a protuberant abdomen despite appearing younger than her age. In a busy ward round you encounter both extremes of the environmental-nutritional disease spectrum: one shaped by decades of inhaled toxins, the other by a single deficient macronutrient. Understanding both requires the same pathologist's toolkit — exposure history, morphological change, and molecular mechanism.
WHY THIS MATTERS
India carries a dual burden: among the world's highest outdoor air-pollution levels (PM2.5 well above WHO guidelines in most cities) and the largest absolute number of underweight children. Tobacco is the single most preventable cause of death globally, responsible for cancers of the lung, mouth, larynx, bladder, and cervix. Nutritional disorders — from kwashiorkor in rural populations to metabolic syndrome in urban ones — now represent opposite ends of a single socio-economic arc. As an MBBS graduate and future clinician, you will diagnose and counsel patients across this entire spectrum.
RECALL
Before proceeding, recall from Year-1:
• Collagen synthesis requires vitamin C as a cofactor for hydroxylation of proline and lysine.
• The cytochrome P450 system in the liver activates many carcinogens (relevant to tobacco and occupational toxins).
• Insulin promotes glucose uptake in muscle and fat; resistance to insulin leads to hyperglycaemia.
• B12 and folate are required for DNA synthesis (you covered this in H4 — megaloblastic anaemia).
Air Pollution — Outdoor and Indoor
Outdoor air pollution is a mixture of particulates and gases. The key pollutants and their main effects are:
| Pollutant | Source | Primary target organ | Key pathological effect |
|---|---|---|---|
| PM2.5 / PM10 (particulate matter) | Vehicles, industry | Lung, cardiovascular | Alveolar inflammation → fibrosis; platelet activation → thrombosis |
| Sulphur dioxide (SO₂) | Coal combustion | Airways | Bronchoconstriction, mucus hypersecretion |
| Nitrogen oxides (NOₓ) | Vehicles | Airways / alveoli | Oxidant injury, ozone precursor |
| Ozone (O₃) | Photochemical smog | Airway epithelium | Lipid peroxidation, epithelial necrosis |
Respiratory effects: chronic bronchitis, accelerated decline in FEV₁, pulmonary hypertension.
Cardiovascular effects: systemic inflammation (raised CRP, IL-6), endothelial dysfunction, accelerated atherosclerosis, arrhythmias.
Indoor air pollution — chiefly from biomass combustion (wood, dung, crop residue) in poorly ventilated kitchens — is a major cause of COPD and lower respiratory infections in rural Indian women who have never smoked.
Pneumoconioses (occupational dust diseases) form a closely related group: coal-worker's pneumoconiosis (coal macules → progressive massive fibrosis), silicosis (silica → activated macrophages → nodular fibrosis), and asbestosis (asbestos fibres → diffuse interstitial fibrosis + risk of mesothelioma). These will be covered in depth in the respiratory pathology module; note the mechanistic link to air pollution here.
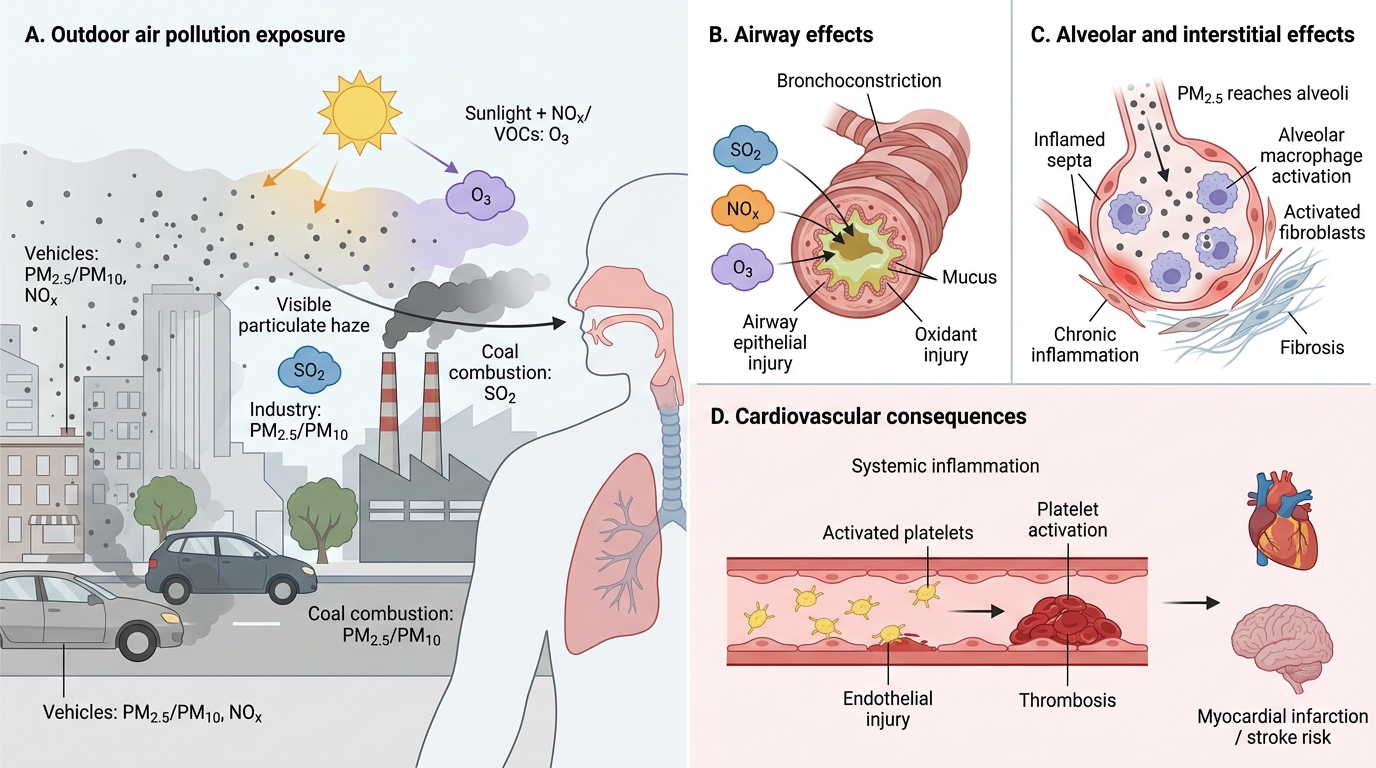
Pathological Effects of Outdoor Air Pollution
Tobacco — Mechanisms of Disease
Tobacco smoke contains >7,000 chemicals. Three categories matter most:
- Carcinogens — polycyclic aromatic hydrocarbons (PAH), nitrosamines, benzene. These are activated by CYP450 in the liver and bronchial epithelium to form DNA adducts, causing point mutations (notably in TP53 and KRAS).
- Carbon monoxide (CO) — binds haemoglobin with 250× the affinity of oxygen, forming carboxyhaemoglobin (COHb). Reduces oxygen delivery, impairs myocardial function, promotes atherosclerosis.
- Nicotine — not a carcinogen, but strongly addictive (dopamine reward pathway), causes sympathetic stimulation (↑HR, ↑BP, vasoconstriction), promotes platelet aggregation.
Key diseases caused by tobacco:
- Lung cancer — ~85% of cases attributable to smoking. Squamous cell carcinoma (central, arises in bronchial epithelium through squamous metaplasia → dysplasia → carcinoma in situ) and small-cell carcinoma have the strongest association. Adenocarcinoma risk is also elevated.
- Other cancers — oral cavity, larynx, oesophagus, bladder (carcinogens excreted in urine), cervix, pancreas.
- COPD / emphysema — smoke activates alveolar macrophages, recruiting neutrophils that release elastase (protease-antiprotease imbalance), destroying alveolar walls → centriacinar emphysema; mucus hypersecretion → chronic bronchitis.
- Atherosclerosis / IHD — CO-mediated endothelial injury + nicotine-driven vasoconstriction + pro-thrombotic state → accelerated plaques, ↑MI risk (2–4×).
- Adverse pregnancy outcomes — low birth weight (CO-mediated hypoxia, nicotine vasoconstriction), spontaneous abortion, placental abruption, sudden infant death syndrome.
Passive smoking delivers the same carcinogens and CO at lower dose; causally linked to lung cancer, IHD, and childhood asthma.
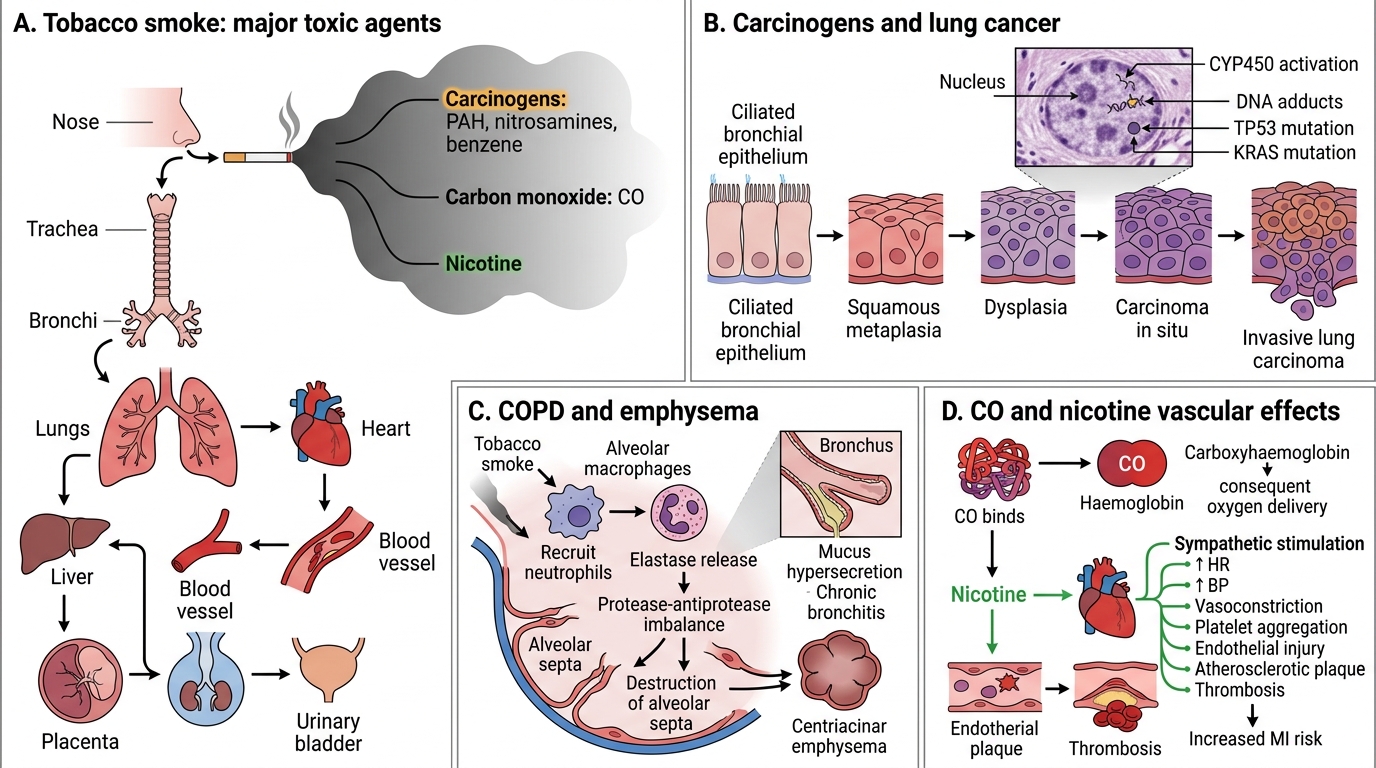
Tobacco Smoke: Mechanisms of Disease
CLINICAL PEARL
Tobacco is the single most preventable cause of death worldwide. When you take a smoking history, always record pack-years (packs/day × years). A patient with 30 pack-years has the same cumulative exposure regardless of whether they smoked 1 pack/day for 30 years or 2 packs/day for 15 years. Cessation at any age reduces risk — lung cancer risk halves within 10 years of stopping.
SELF-CHECK
A 52-year-old bidi smoker develops a central lung mass on CT. Biopsy shows keratin pearls and intercellular bridges. Which component of tobacco smoke is MOST responsible for the DNA mutation initiating this tumour?
A. Carbon monoxide forming carboxyhaemoglobin
B. Nicotine activating dopamine reward pathways
C. Polycyclic aromatic hydrocarbons forming DNA adducts via CYP450 activation
D. Sulphur dioxide causing bronchoconstriction
Reveal Answer
Answer: C. Polycyclic aromatic hydrocarbons forming DNA adducts via CYP450 activation
The biopsy features (keratin pearls, intercellular bridges) describe squamous cell carcinoma — the lung cancer type most strongly linked to smoking. The initiating mutations arise from DNA adducts formed when CYP450-activated PAH metabolites bind guanine residues, causing G→T transversions in TP53 and KRAS. CO causes hypoxia/endothelial injury, nicotine mediates addiction and vasoconstriction, and SO₂ is an outdoor pollutant — none of these are the primary carcinogenic mechanism.
Brief: Alcohol, Heavy Metals, and Occupational Toxins
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
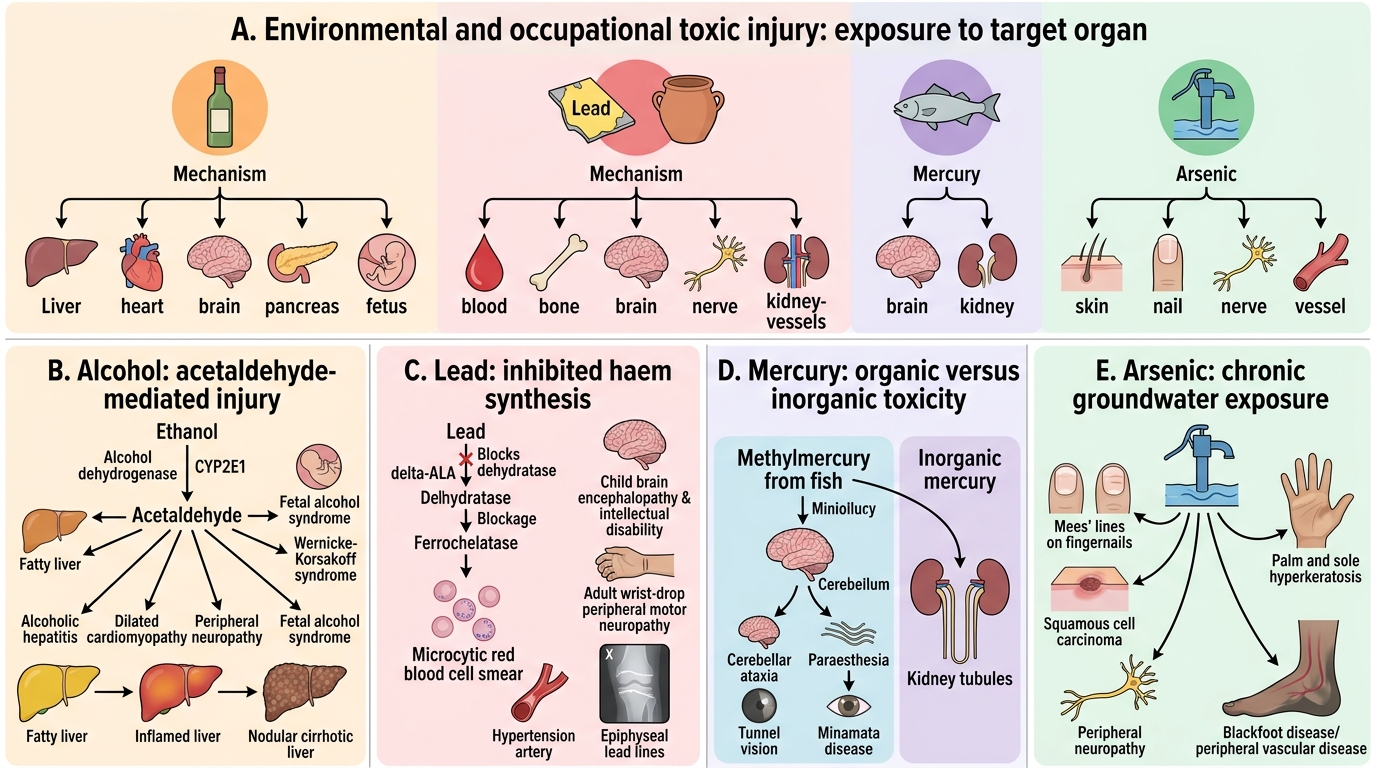
Alcohol, Heavy Metals, and Occupational Toxins
Alcohol (ethanol) — metabolised by alcohol dehydrogenase and CYP2E1 to acetaldehyde (toxic). Pathological consequences: alcoholic fatty liver → alcoholic hepatitis → cirrhosis; dilated cardiomyopathy; peripheral neuropathy; Wernicke-Korsakoff syndrome (B1 deficiency); pancreatitis; foetal alcohol syndrome.
Lead toxicity — sources: old paint, leaded petrol exhaust, certain ceramics. Lead inhibits haem synthesis (δ-ALA dehydratase and ferrochelatase) → microcytic anaemia with basophilic stippling. In children: encephalopathy, intellectual disability; in adults: peripheral motor neuropathy, hypertension. Radiological: lead lines at epiphyses.
Mercury toxicity — organic mercury (methylmercury from fish) causes cerebellar ataxia, paraesthesia, tunnel vision (Minamata disease). Inorganic mercury affects the kidneys.
Arsenic toxicity — chronic exposure (contaminated groundwater — a major problem in West Bengal and Bangladesh): Mees' lines on nails, hyperkeratosis, skin cancer (squamous cell carcinoma of skin), peripheral neuropathy, blackfoot disease (peripheral vascular disease).