Page 11 of 20
PA12.1-3 | Environmental & Nutritional Diseases — SDL Guide (Part 2)
Protein-Calorie Malnutrition — Kwashiorkor and Marasmus
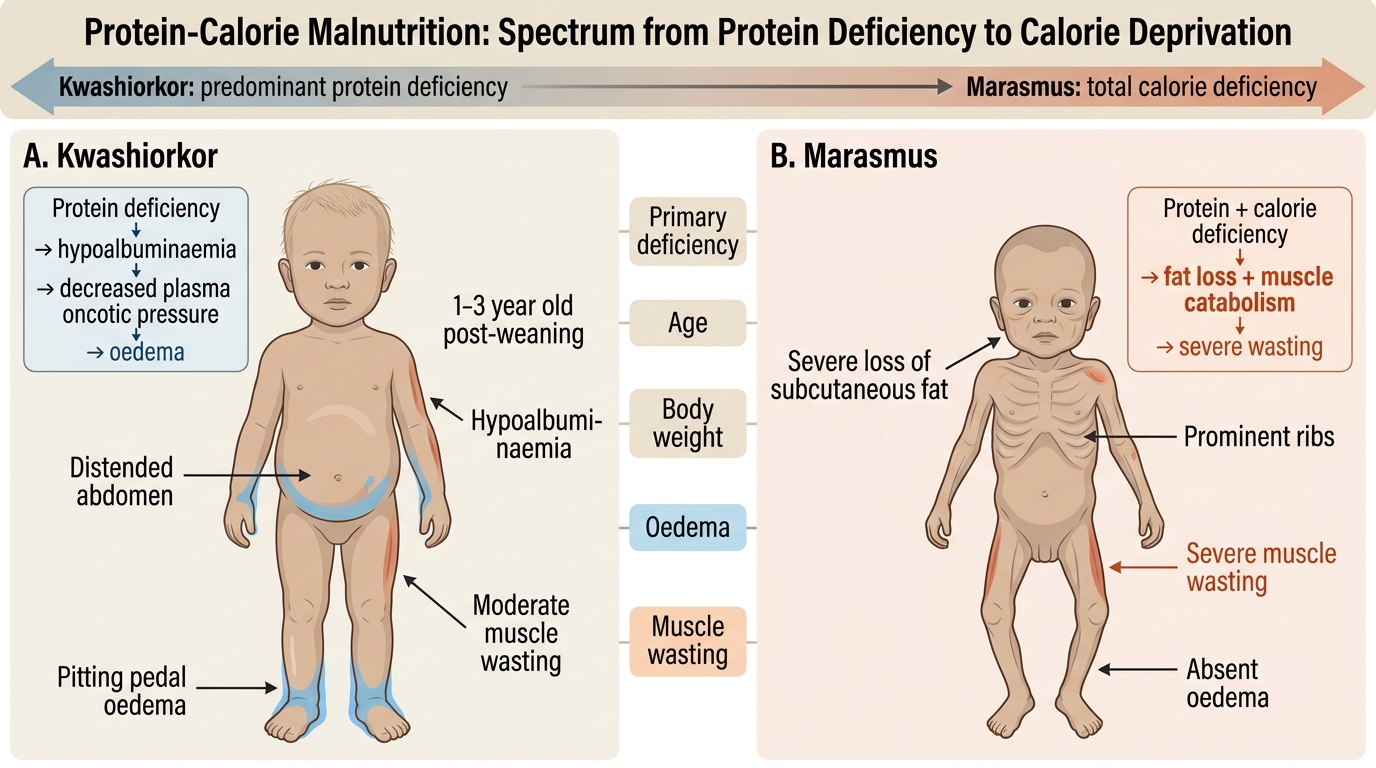
Protein-calorie malnutrition (PCM) occupies a spectrum from pure protein deficiency to total caloric deprivation. The two ends of this spectrum have distinct pathophysiology and morphology:
| Feature | Kwashiorkor | Marasmus |
|---|---|---|
| Primary deficiency | Protein (calories may be adequate — e.g., weaning diet of starchy gruel) | Total calorie deficit (protein + energy) |
| Age of onset | 1–3 years (post-weaning) | Infancy / early childhood |
| Body weight | Near-normal or slightly low | Severely low (<60% expected weight) |
| Oedema | Present (hypoalbuminaemia → ↓oncotic pressure) | Absent |
| Muscle wasting | Moderate | Severe ("skin and bones", "wizened monkey") |
| Subcutaneous fat | Preserved | Severely depleted |
| Fatty liver | Present (↓apolipoproteins → impaired VLDL export → fat accumulates in hepatocytes) | Absent |
| Skin/hair changes | Flaky-paint dermatitis, flag sign (alternating light/dark bands in hair due to alternating protein deficiency), depigmentation | Loose, wrinkled skin; no rash |
| Serum albumin | Markedly low | Low-normal (adaptation maintains albumin) |
| Mood/affect | Apathetic, miserable | Paradoxically alert |
Pathophysiology of kwashiorkor oedema: Adequate calorie intake allows insulin secretion to suppress fat mobilisation, but absent dietary protein means hepatic synthesis of albumin and other proteins collapses. Hypoalbuminaemia → reduced plasma oncotic pressure → fluid shifts to interstitium → oedema (generalised: peripheral + ascites + facial).
Kwashiorkor vs Marasmus in Protein-Calorie Malnutrition
SELF-CHECK
A 2-year-old boy is brought with bilateral pedal oedema, a protuberant abdomen, and reddish, easily pluckable hair. His diet consists mainly of maize porridge since weaning 8 months ago. Which biochemical mechanism BEST explains his oedema?
A. Raised portal pressure from hepatic fibrosis
B. Hypoalbuminaemia reducing plasma oncotic pressure, causing fluid shift to interstitium
C. Renal sodium retention from activation of the RAAS due to total calorie deficiency
D. Lymphatic obstruction from parasitic infection
Reveal Answer
Answer: B. Hypoalbuminaemia reducing plasma oncotic pressure, causing fluid shift to interstitium
This is classic kwashiorkor — protein-deficient diet (maize porridge) with adequate calories suppresses fat mobilisation but collapses hepatic albumin synthesis. Hypoalbuminaemia is the key driver: low oncotic pressure allows fluid to escape the intravascular compartment into the interstitium (Starling forces). Portal hypertension (option A) occurs in cirrhosis, not kwashiorkor. RAAS-mediated retention (option C) characterises marasmic adaptation. Lymphatic obstruction (option D) produces localised, not generalised oedema.
Vitamin Deficiency Diseases — High-Yield Summary
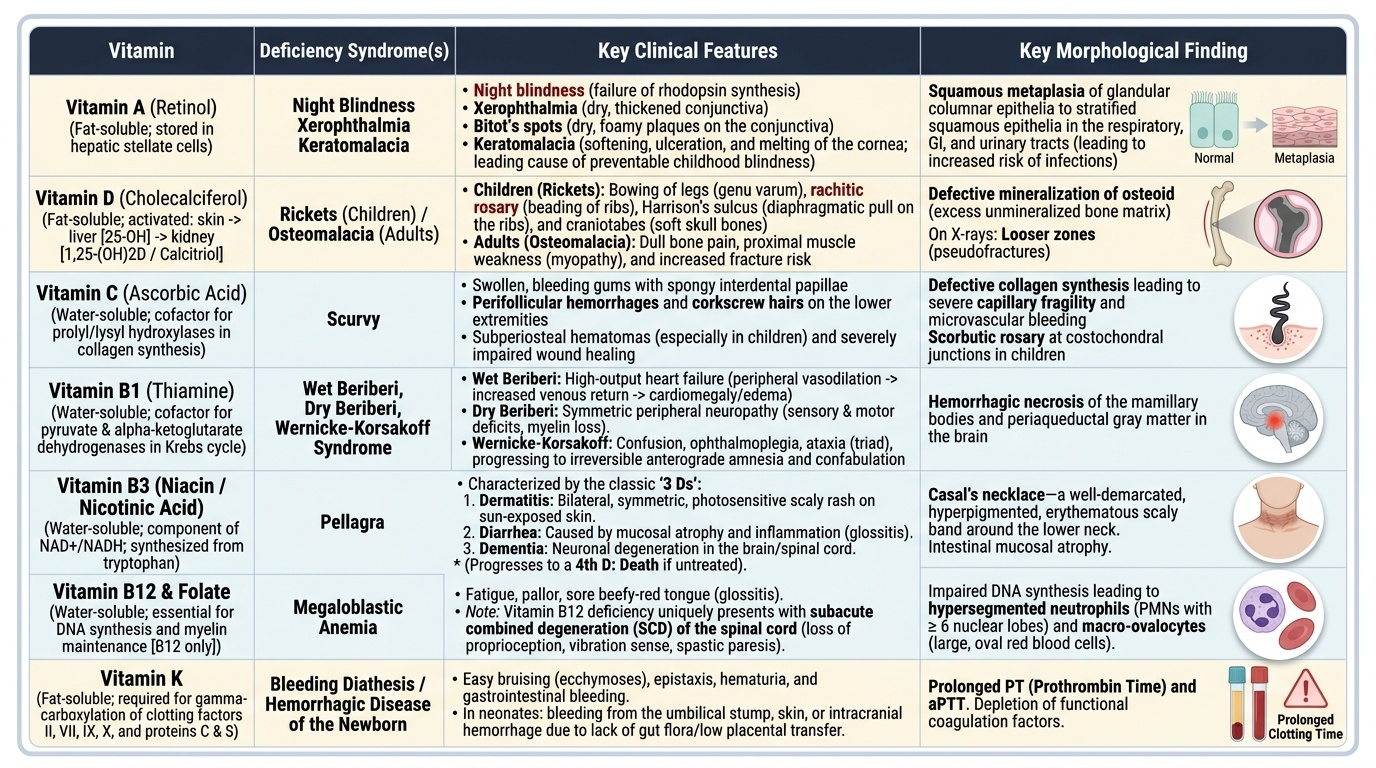
Vitamin A (retinol) — fat-soluble; stored in hepatic stellate cells.
• Deficiency: night blindness (rhodopsin synthesis fails) → xerophthalmia (dry, thickened conjunctiva) → Bitot's spots (foamy conjunctival plaques) → keratomalacia (corneal ulceration and melting — leading preventable cause of childhood blindness).
• Squamous metaplasia of respiratory, GI, and urinary epithelia → increased infection risk.
Provided image
Vitamin D (cholecalciferol) — synthesised in skin from 7-dehydrocholesterol under UV; activated in liver (25-OH) then kidney (1,25-dihydroxy = calcitriol).
• Deficiency: inadequate mineralisation of osteoid → rickets (children: bowing of legs, rachitic rosary, Harrison's sulcus, craniotabes) / osteomalacia (adults: bone pain, proximal myopathy, Looser zones on X-ray).
Vitamin C (ascorbic acid) — water-soluble; essential cofactor for prolyl and lysyl hydroxylases in collagen synthesis.
• Deficiency (scurvy): perifollicular haemorrhages, corkscrew hairs, bleeding gums with swollen/spongy interdental papillae, subperiosteal bleeding (children), poor wound healing. Morphology: defective collagen → capillary fragility; scorbutic rosary (costochondral junction haemorrhage in children).
Vitamin B1 (thiamine) — cofactor for pyruvate dehydrogenase and α-ketoglutarate dehydrogenase (Krebs cycle).
• Deficiency (beriberi): Wet beriberi — high-output cardiac failure (dilatation of arterioles → ↑venous return → cardiac dilatation); Dry beriberi — peripheral polyneuropathy (demyelination).
• Wernicke's encephalopathy (classically in alcoholics): triad of confusion, ophthalmoplegia, ataxia — haemorrhagic necrosis of mamillary bodies and periaqueductal grey. Untreated → Korsakoff syndrome (anterograde amnesia, confabulation — irreversible).
Vitamin B3 (niacin/nicotinic acid) — component of NAD⁺/NADH.
• Deficiency (pellagra): 3 Ds — Dermatitis (photosensitive, symmetric rash in sun-exposed areas — Casal's necklace), Diarrhoea (glossitis, intestinal atrophy), Dementia (neuronal degeneration). A 4th D is Death if untreated.
• Common in populations dependent on maize (low in niacin and tryptophan, which is the niacin precursor).
Vitamin B12 and Folate — covered in Cluster H4 (megaloblastic anaemia). Briefly: deficiency impairs DNA synthesis → megaloblastic changes in all rapidly dividing cells. B12 also required for myelin synthesis (subacute combined degeneration of the cord — dorsal + lateral columns).
Vitamin K — fat-soluble; essential for hepatic synthesis of clotting factors II, VII, IX, X and anticoagulants protein C and S (γ-carboxylation of glutamate residues).
• Deficiency: bleeding diathesis — prolonged PT and aPTT. Seen in newborns (haemorrhagic disease of newborn — prophylactic IM vitamin K given at birth), fat malabsorption (cholestasis, coeliac), prolonged antibiotic use (kills gut flora).
CLINICAL PEARL
A useful mnemonic for pellagra: "3 Ds from lack of Bs" — Dermatitis, Diarrhoea, Dementia from B3 (niacin) deficiency. In clinical practice, any chronic alcoholic or malnourished patient with a photosensitive rash and cognitive change needs niacin supplementation. Isoniazid (INH) used for TB treatment inhibits B6, which is a precursor in tryptophan→niacin conversion — supplement pyridoxine when prescribing INH.
SELF-CHECK
A 4-year-old girl in a drought-affected region presents with bilateral corneal ulceration and cloudy, soft-appearing corneas. Her mother reports she has trouble seeing at dusk. Which vitamin deficiency and pathological process best explain the corneal findings?
A. Vitamin C deficiency leading to collagen synthesis failure and corneal stromal breakdown
B. Vitamin A deficiency causing squamous metaplasia of the corneal epithelium progressing to keratomalacia
C. Vitamin D deficiency impairing calcium-dependent corneal clarity
D. Vitamin B2 deficiency causing corneal vascularisation and ulceration
Reveal Answer
Answer: B. Vitamin A deficiency causing squamous metaplasia of the corneal epithelium progressing to keratomalacia
Night blindness (trouble at dusk) + corneal ulceration with softening = keratomalacia — the end-stage of Vitamin A deficiency. Vitamin A is essential for maintenance of specialised surface epithelia; deficiency causes squamous metaplasia and loss of goblet cells (xerophthalmia) progressing to corneal ulceration and melting (keratomalacia). Vitamin C deficiency causes capillary fragility and scurvy but not corneal ulceration. Vitamin D deficiency causes bone disease. Vitamin B2 deficiency causes corneal vascularisation but not ulceration.
Obesity — Definition, Pathogenesis, and Adipokines
Obesity: Definition, Pathogenesis, and Adipokines
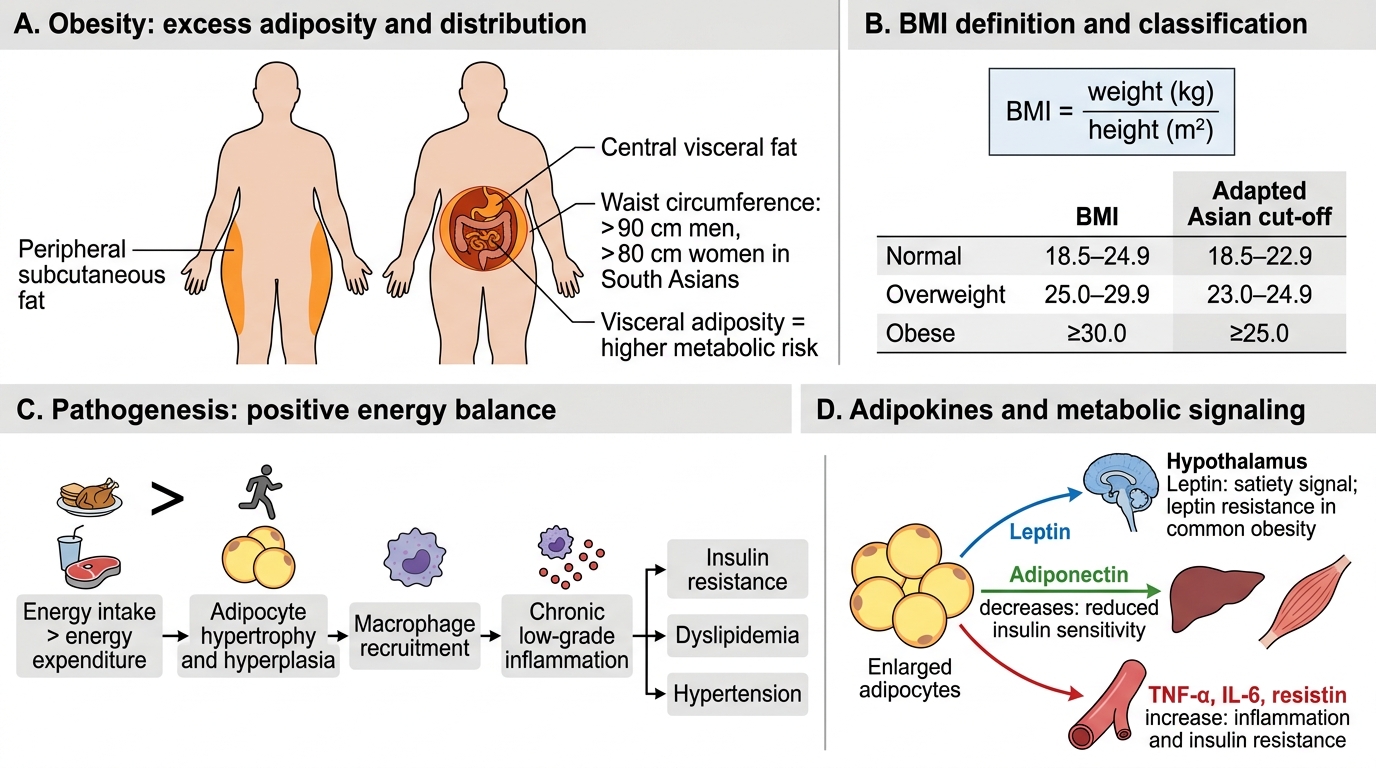
Obesity is defined by excess body fat sufficient to impair health. The commonly used clinical measure is the body mass index (BMI) = weight (kg) / height (m²).
| Classification | BMI (kg/m²) | Adapted Asian cut-off |
|---|---|---|
| Normal | 18.5–24.9 | 18.5–22.9 |
| Overweight | 25.0–29.9 | 23.0–24.9 |
| Obese | ≥30.0 | ≥25.0 |
Central (visceral) adiposity is more metabolically dangerous than peripheral (subcutaneous) fat. Waist circumference >90 cm (men) / >80 cm (women) in South Asians signals excess visceral fat.
Pathogenesis of obesity:
A positive energy balance (intake > expenditure) is the proximate cause, but the molecular regulation involves:
- Leptin — adipokine secreted proportional to fat mass; acts on hypothalamus to suppress appetite and ↑energy expenditure. In obesity, circulating leptin is high, but leptin resistance develops (analogous to insulin resistance), so appetite suppression fails.
- Adiponectin — anti-inflammatory, insulin-sensitising adipokine. Paradoxically low in obesity despite increased fat mass — loss of this protective signal contributes to insulin resistance and inflammation.
- Inflammatory adipokines (TNF-α, IL-6, resistin) — secreted by hypertrophied adipocytes and infiltrating macrophages in visceral fat → systemic low-grade inflammation → insulin receptor signalling disruption → insulin resistance.
- Insulin resistance → hyperinsulinaemia → further fat deposition (vicious cycle) → β-cell exhaustion → Type 2 Diabetes Mellitus (T2DM).