Page 12 of 20
PA12.1-3 | Environmental & Nutritional Diseases — SDL Guide (Part 3)
Metabolic Syndrome — Criteria and Consequences
Metabolic syndrome is a cluster of cardiometabolic risk factors that frequently co-occur due to their shared driver: visceral adiposity and insulin resistance.
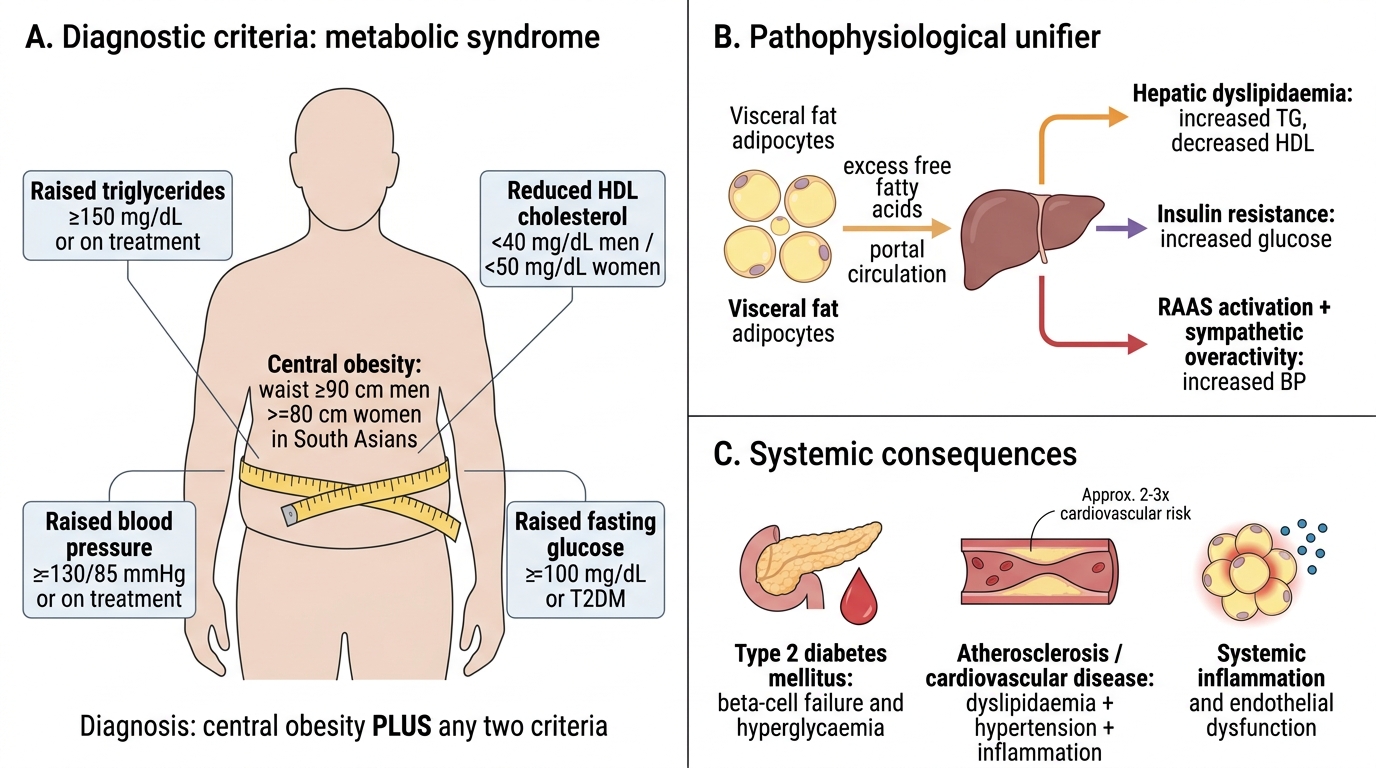
Diagnostic criteria (IDF 2006 / modified ATP III):
Central obesity (waist ≥90 cm men / ≥80 cm women in South Asians) PLUS any two of:
| Component | Cut-off |
|---|---|
| Raised triglycerides | ≥150 mg/dL (or on treatment) |
| Reduced HDL cholesterol | <40 mg/dL (men), <50 mg/dL (women) |
| Raised blood pressure | ≥130/85 mmHg (or on treatment) |
| Raised fasting glucose | ≥100 mg/dL (or diagnosed T2DM) |
Pathophysiological unifier: visceral fat → excess free fatty acids → hepatic dyslipidaemia (↑TG, ↓HDL) + insulin resistance (↑glucose) + RAAS activation and sympathetic overactivity (↑BP).
Systemic consequences of obesity and metabolic syndrome:
- Type 2 Diabetes Mellitus — insulin resistance → β-cell failure → hyperglycaemia
- Atherosclerosis / cardiovascular disease — dyslipidaemia, hypertension, and systemic inflammation accelerate plaque formation; metabolic syndrome confers 2–3× CV risk
- Non-alcoholic fatty liver disease (NAFLD) → steatohepatitis (NASH) → cirrhosis — driven by excess free fatty acids and insulin resistance
- Obstructive sleep apnoea (OSA) — fat deposition in pharyngeal tissues; OSA further worsens insulin resistance
- Cancer risk — colorectal, endometrial, breast (post-menopausal), renal, oesophageal adenocarcinoma; mechanisms: hyperinsulinaemia (↑IGF-1), adipokine signalling, chronic inflammation
- Polycystic ovary syndrome, hyperuricaemia/gout, osteoarthritis (mechanical load)
Metabolic Syndrome: Criteria, Mechanism and Consequences
SELF-CHECK
A 44-year-old man has a waist circumference of 96 cm, fasting glucose 108 mg/dL, triglycerides 190 mg/dL, HDL 36 mg/dL, and blood pressure 136/88 mmHg. Which ONE adipokine is PARADOXICALLY LOW despite his increased fat mass and most contributes to his insulin resistance?
A. Leptin
B. TNF-α
C. Resistin
D. Adiponectin
Reveal Answer
Answer: D. Adiponectin
This patient meets criteria for metabolic syndrome (central obesity + all 4 other criteria present). Adiponectin is the key anti-inflammatory, insulin-sensitising adipokine that is paradoxically LOW in obesity — its loss removes an important brake on insulin resistance and inflammation. Leptin is HIGH in obesity (though functionally ineffective due to resistance). TNF-α and resistin are pro-inflammatory adipokines that are elevated in obesity and worsen insulin resistance, but the 'paradoxically low despite high fat mass' clue specifically points to adiponectin.
Linking Environmental and Nutritional Disease: A Synthesis
Time Scale of Environmental and Nutritional Disease
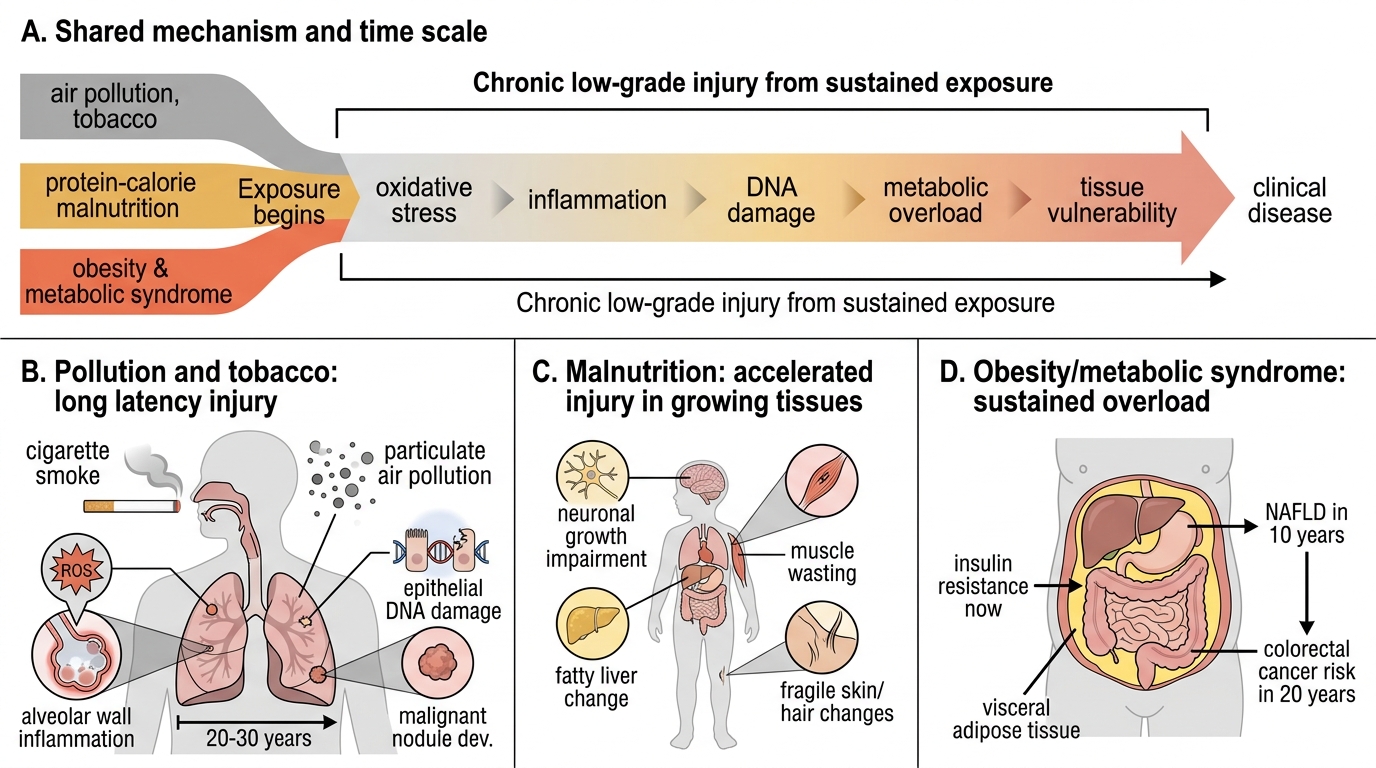
The three PA12 competency areas share a common pathological theme: chronic low-grade injury from sustained exposure.
- Air pollution and tobacco cause decades-long oxidative stress, inflammation, and DNA damage before clinical disease appears — the latency between first cigarette and lung cancer is typically 20–30 years.
- Protein-calorie malnutrition causes accelerated morphological changes in actively growing tissues — the child's developing brain, liver, and skin are the earliest casualties.
- Obesity and metabolic syndrome represent a sustained metabolic overload — the same visceral adiposity that causes insulin resistance today causes NAFLD in 10 years and colorectal cancer in 20.
Recognising the time scale of these exposures is as important as knowing the pathological endpoint — it is the foundation of both primary prevention counselling and early diagnosis.