Page 3 of 20
PA10.1-5 | Infections & Infestations — SDL Guide (Part 3)
Integrating the Concepts: A Diagnostic Framework
Diagnostic Framework for Infectious Diseases
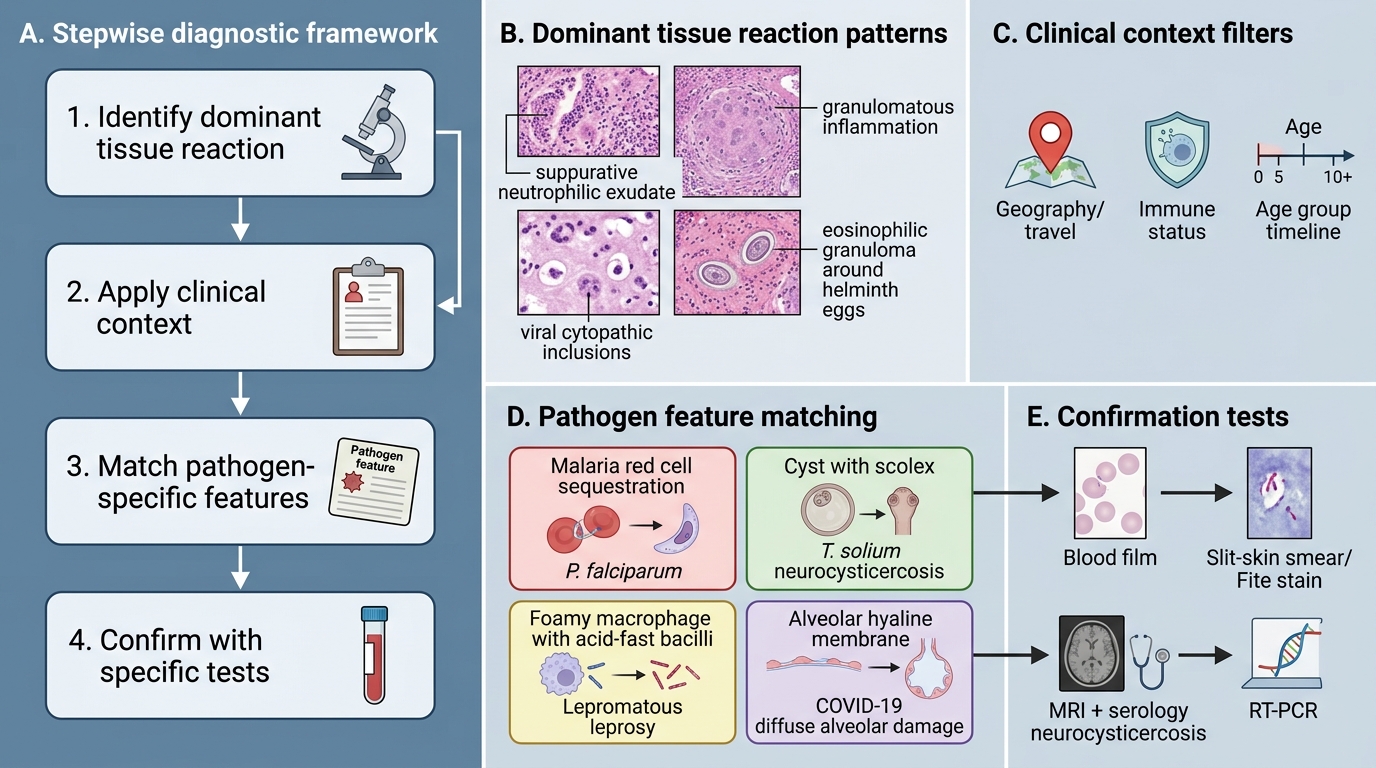
When you encounter an infectious disease case — in clinical practice, on autopsy, or in an exam — use this stepwise framework:
Step 1: Identify the dominant tissue reaction
• Suppurative → pyogenic bacteria
• Granulomatous → mycobacteria, fungi, some parasites
• Cytopathic inclusions → viruses
• Eosinophilic + granuloma around eggs → helminths
Step 2: Apply clinical context
• Geography and travel history (malaria belt, cysticercosis-endemic area)
• Immune status (HIV/immunosuppression → opportunistic fungi, CMV, Pneumocystis)
• Age (neonates → CMV, toxoplasma; elderly → reactivation TB; young adult → NCC)
Step 3: Match to specific pathogen features
• Sequestration + crescent gametocytes → P. falciparum
• Cyst with scolex + eosinophilia → T. solium (NCC)
• Foamy macrophages + AFB on Fite stain → lepromatous leprosy
• Hyaline membranes + lymphopenia + ↑D-dimer → COVID-19 DAD
Step 4: Confirm with specific tests
• Blood film (malaria), slit-skin smear/Fite stain (leprosy), MRI+serology (NCC), RT-PCR (COVID-19)
This framework converts a complex, memorisation-heavy topic into a logical, reproducible thought process — the hallmark of clinical thinking.
SELF-CHECK
A 40-year-old HIV-positive patient (CD4 count 80 cells/μL) presents with headache, fever, and a positive India ink preparation of CSF showing encapsulated round yeast cells. A chest X-ray shows bilateral interstitial infiltrates. Methenamine silver stain of BAL fluid shows small disc-shaped organisms (2–8 μm) without budding. Two SEPARATE pathogens are involved. Which combination is MOST likely?
A. Aspergillus fumigatus (CNS) + Candida albicans (lung)
B. Cryptococcus neoformans (CNS) + Pneumocystis jirovecii (lung)
C. Mucor (CNS) + Histoplasma capsulatum (lung)
D. Toxoplasma gondii (CNS) + Cytomegalovirus (lung)
Reveal Answer
Answer: B. Cryptococcus neoformans (CNS) + Pneumocystis jirovecii (lung)
India ink showing encapsulated round budding yeast with a large mucoid capsule = Cryptococcus neoformans (CNS meningitis). The methenamine silver (GMS) stain showing small (2–8 μm) 'disc-shaped' or 'cup-shaped' organisms without budding in BAL = Pneumocystis jirovecii pneumonia (PCP) — classic for CD4 <200 cells/μL. At CD4 <100, Cryptococcal meningitis is the prototypical CNS opportunist. These two AIDS-defining infections co-occurring is a classical examination scenario. Aspergillus causes hyphal invasion (not encapsulated yeast), Mucor causes angio-invasive disease, and Toxoplasma causes ring-enhancing brain lesions (not meningitis), CMV causes owl-eye inclusions.
CLINICAL PEARL
Remembering the leprosy spectrum in 20 seconds: Think of it as a tug-of-war between the immune system and the bacteria. At the TT end, the immune system wins (granuloma formed, bacilli killed) — but it over-destroys the nerve in the process. At the LL end, the bacteria win (lepra cells full of AFB, anergic T-cells) — the nerve is infiltrated slowly but the patient is full of contagious organisms. The lepromin test and AFB count move in opposite directions across the spectrum: strong lepromin (↑) / no AFB (TT) to negative lepromin (↓) / abundant AFB (LL).