Page 1 of 18
PA7.1 | Diagnostic Cytology — SDL Guide
Learning Objectives
- Define cytology and distinguish it from histopathology
- Describe the techniques of exfoliative and interventional cytology, including FNAC
- Explain the Papanicolaou, MGG/Romanowsky, and H&E staining methods and their respective strengths
- List the cytological criteria of malignancy
- Outline the diagnostic applications, advantages, and limitations of cytology in clinical practice
INSTRUCTIONS
Cytology is the first-line investigation for millions of cancer diagnoses each year. From a Pap smear taken in a gynaecology clinic to an FNAC of a neck lump performed at the bedside, cytological techniques offer rapid, minimally invasive answers with minimal patient risk. As a Year-2 student, understanding how cells are collected, stained, and interpreted — and when to escalate to histopathology — equips you to reason through both screening programmes and diagnostic pathways.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 1 (The Cell as a Unit of Health and Disease) (textbook)
- Harsh Mohan, Textbook of Pathology, 8th ed., Ch 3 (Cytopathology) (textbook)
- DeMay RM, The Art and Science of Cytopathology, 2nd ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old woman attends a routine cervical cancer screening camp in a rural district. A Pap smear takes 60 seconds to collect. Three days later, the cytologist's report reads: High-grade squamous intraepithelial lesion (HSIL) — recommend colposcopy and biopsy. No surgery, no anaesthesia, no waiting weeks for a result. Cytology just changed her life trajectory.
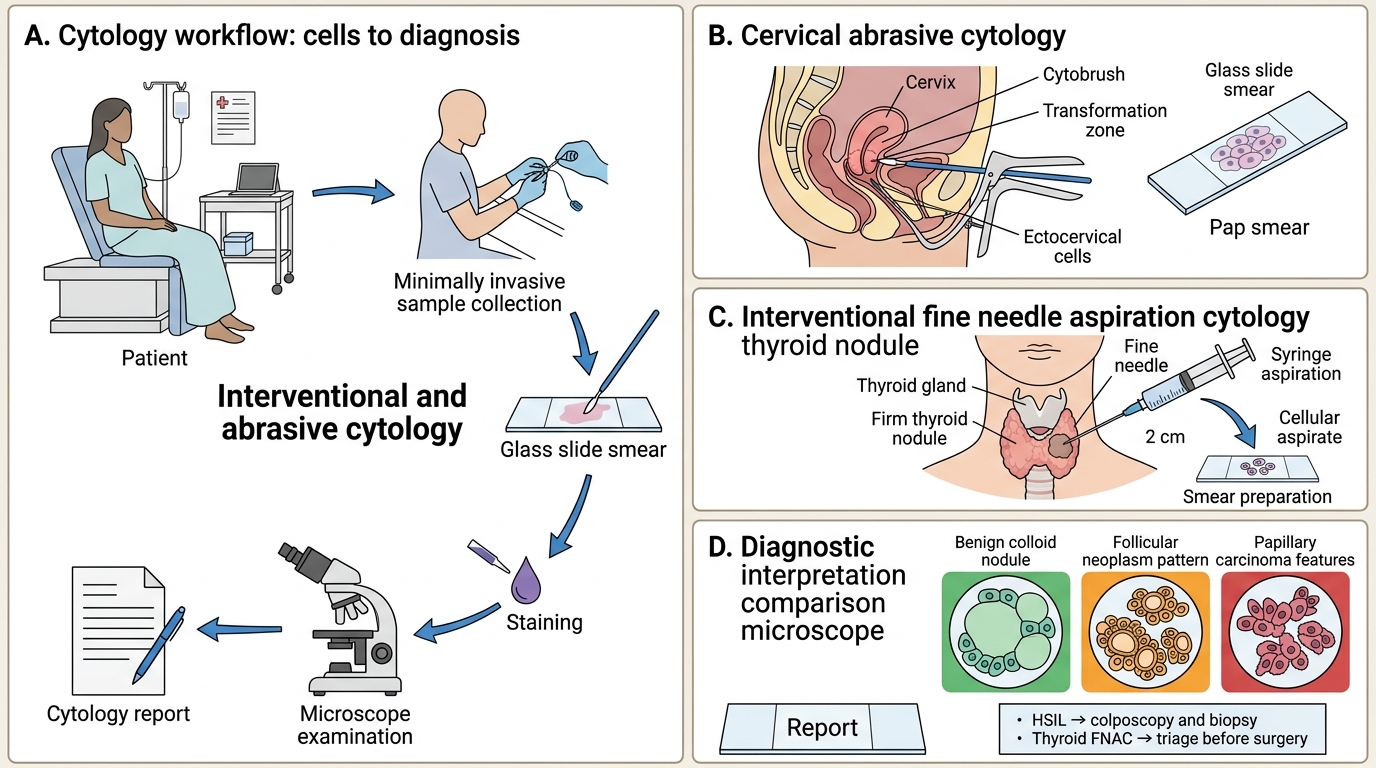
Now consider a surgeon who feels a 2 cm firm lump in a patient's thyroid. Rather than sending her to the operating theatre blind, a fine needle is passed into the lump and cells are aspirated. The smear is stained within minutes. Is it a colloid nodule, follicular neoplasm, or papillary carcinoma? Cytology answers that question before a single incision is made.
This module demystifies how cells are collected, processed, and interpreted — and what those interpretations can and cannot tell us.
WHY THIS MATTERS
PA7.1 explicitly requires you to understand techniques of cytology, staining, and the diagnostic role of cytology and its applications. This competency is assessed in the University practical examination (slide identification, staining principles), in clinico-pathological case discussions (when to request cytology vs biopsy), and in professional practice — every physician requisitions cytology reports and must read them intelligently.
The NMC 2024 curriculum positions diagnostic cytology as the bridge between basic pathology (cell injury, neoplasia) and clinical medicine. Mastering this module also underpins your later work in PA8 (neoplasia in individual systems), PA17 (gynaecological pathology), and clinical postings in Surgery, OBG, and Medicine.
RECALL
Before proceeding, activate what you already know:
- What is the difference between a cell and a tissue? Cytology examines individual cells or small cell clusters; histology examines the architecture of intact tissue sections.
- Name two epithelial cell types. Squamous (stratified, surface shedding) and columnar (glandular, secretory) — both are harvested in cervical cytology.
- What is the nucleus:cytoplasm (N:C) ratio? The proportion of nuclear area to total cell area — a key marker in neoplasia.
- Recall the cell cycle. Rapidly dividing cells (high mitotic index) are more likely to be malignant — cytology captures nuclear features that reflect this.
- What is staining in histology? Differential binding of dyes to tissue components. The same principle applies to cytological smears but with different fixation requirements.
What is Cytology? Definition, Scope, and Relationship to Histopathology
Cytology and Histopathology: Definition, Scope, and Relationship
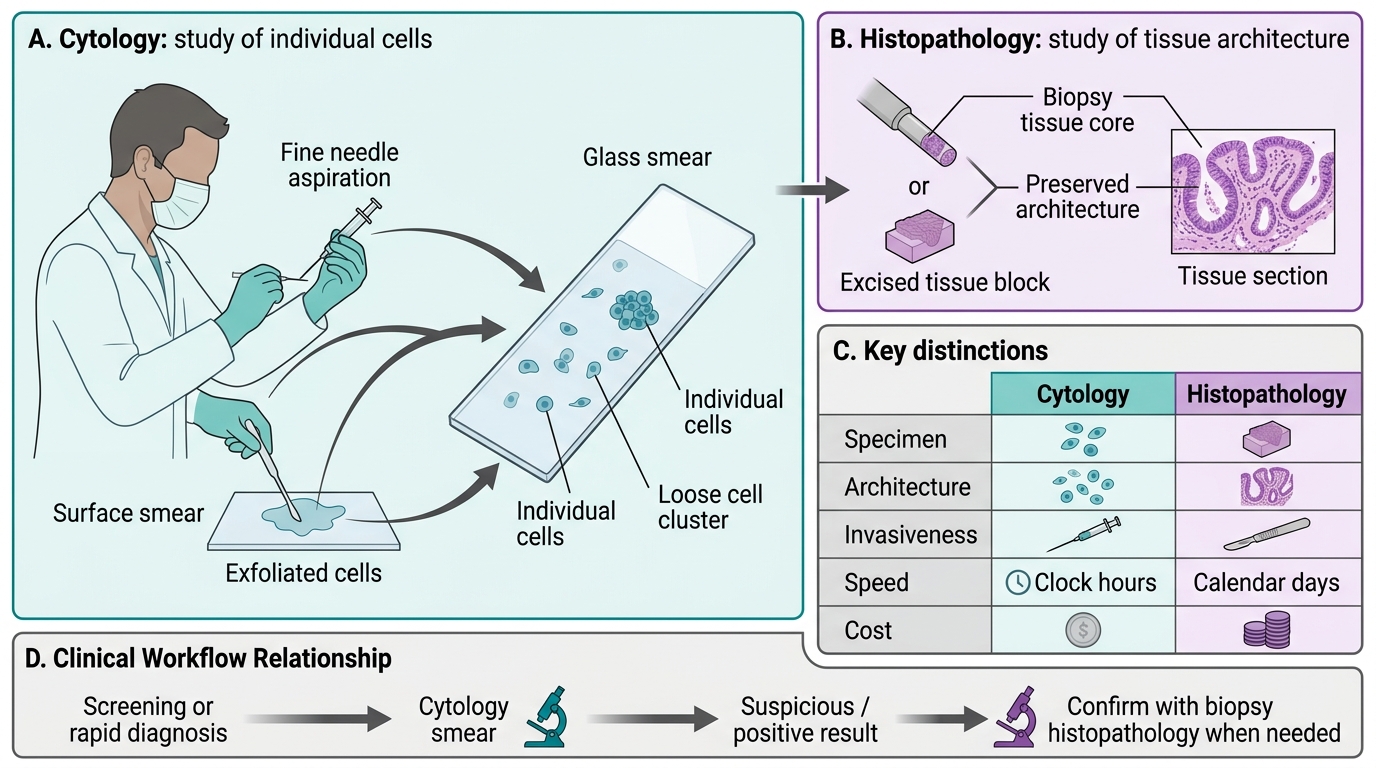
Cytology (from Greek kytos, cell) is the branch of pathology that studies cells shed from or aspirated out of body surfaces or organs. Unlike histopathology, which examines intact tissue sections preserving the spatial architecture of cells, cytology examines individual cells or small loosely cohesive clusters on a glass smear.
Key distinctions:
| Feature | Cytology | Histopathology |
|---|---|---|
| Specimen | Individual cells / cell clusters | Intact tissue core or excised block |
| Architecture preserved? | No | Yes |
| Invasiveness | Minimal (smear, FNA) | Moderate–high (biopsy, excision) |
| Speed of result | Hours | 1-3 days (routine) |
| Cost | Low | Higher |
| Stroma visible? | No | Yes |
Advantages of cytology:
• Rapid, cheap, and minimally invasive
• High patient acceptability — suitable for mass screening
• Can be repeated serially (monitoring)
• Does not require an operating theatre
Limitations:
• No tissue architecture — cannot determine invasion, depth, or stromal reaction
• Cannot classify some tumours that require architectural patterns (e.g., follicular adenoma vs carcinoma of thyroid)
• Sampling error — non-representative aspiration yields a false-negative
• Interpretation requires cytopathology expertise
The cytology–histology relationship: A positive (malignant) cytology report is highly specific for cancer but a negative report does not exclude it. Histological biopsy is still required for:
• Definitive tumour typing and grading
• Assessment of surgical margins
• Staging (lymphovascular invasion, depth)
• Cases where cytology is suspicious but not conclusive
Exfoliative Cytology — Naturally Shed Cells
Exfoliative cytology collects cells that are naturally shed (exfoliated) from epithelial surfaces into body fluids or onto accessible surfaces. No needles are required.
1. Cervical/Pap Smear
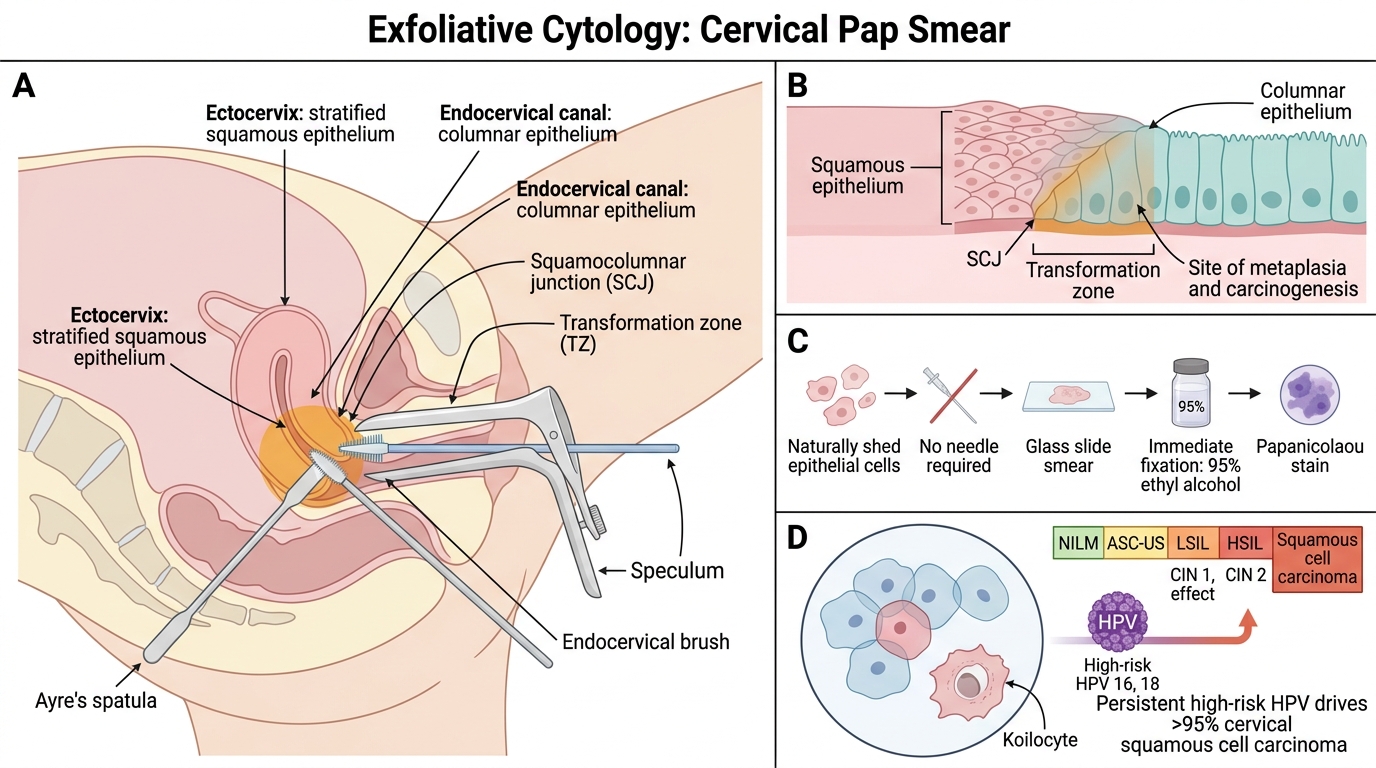
The Papanicolaou (Pap) smear screens for cervical cancer and its precursors. Technique:
1. Position the patient (lithotomy); insert a bivalve speculum.
2. Sample the transformation zone (TZ) — the junction between the squamocolumnar junction (SCJ) of ectocervix (stratified squamous epithelium) and endocervix (columnar epithelium). This TZ is where squamous metaplasia and carcinogenesis begin.
3. Use an Ayre's spatula (ectocervix) + endocervical brush to collect cells from both zones.
4. Smear onto a glass slide and fix immediately in 95% ethyl alcohol (or use liquid-based cytology — LBC — see later block).
5. Stain by Papanicolaou method.
Bethesda System (2014 revision) — reporting categories:
• Negative for intraepithelial lesion or malignancy (NILM)
• Atypical squamous cells of undetermined significance (ASCUS)
• Low-grade squamous intraepithelial lesion (LSIL) — CIN 1, HPV effect
• High-grade squamous intraepithelial lesion (HSIL) — CIN 2/3
• Squamous cell carcinoma
• (Plus glandular lesion categories for endocervical/endometrial cells)
HPV and cervical cancer: Persistent infection with high-risk HPV (types 16, 18) drives > 95% of cervical squamous cell carcinomas. The Pap smear detects morphological changes (koilocytes in LSIL); HPV co-testing by molecular methods improves sensitivity. Pap smear screening has reduced cervical cancer mortality by > 70% in countries with robust programmes.
Exfoliative Cytology: Cervical Pap Smear
2. Sputum Cytology
Used for suspected lung malignancy. Patient produces a deep-cough morning sample (3 consecutive days). Squamous cell carcinomas and some small-cell carcinomas exfoliate well; adenocarcinomas of the periphery do not. Sensitivity ~65% for central tumours.
3. Urine Cytology
Catches urothelial (transitional cell) carcinoma cells, especially high-grade lesions and carcinoma in situ. Voided urine or bladder washings (catheter specimen). Low-grade urothelial carcinomas have near-normal morphology and are often cytology-negative.
4. Effusion Cytology (Body Cavity Fluids)
Pleurial, peritoneal (ascitic), and cerebrospinal fluid (CSF) are centrifuged; the cell button (sediment) is smeared and stained.
- Reactive mesothelial cells — enlarged, activated, with nucleoli; arranged singly or in clusters; hallmark: intercellular windows (spaces between adjacent cells)
- Malignant cells — form large 3D cell balls (morulae), nuclear moulding, prominent nucleoli, loss of intercellular windows
- Reactive vs malignant distinction is one of the most challenging in cytopathology; clinical context (known primary tumour? pleural thickening on CT?) is essential.
SELF-CHECK
A 38-year-old woman's Pap smear report reads: 'HSIL — High-grade squamous intraepithelial lesion.' Which anatomical zone of the cervix is the primary target of cytological sampling, and why?
A. The vaginal fornix, because it accumulates the highest concentration of exfoliated cervical cells
B. The endometrial cavity, because endometrial cells are more likely to become malignant
C. The transformation zone (SCJ), because squamous metaplasia and carcinogenesis predominantly occur here
D. The ectocervix only, because the endocervical brush introduces sampling artefact
Reveal Answer
Answer: C. The transformation zone (SCJ), because squamous metaplasia and carcinogenesis predominantly occur here
The transformation zone (TZ) is the dynamic metaplastic area between the original squamocolumnar junction and the current SCJ. HPV infects metaplastic reserve cells here, driving the progression LSIL→HSIL→invasive carcinoma. Both the Ayre spatula (ectocervix) and endocervical brush must be used to adequately sample the TZ. Sampling the endometrial cavity is a different procedure (endometrial sampling); vaginal fornix cells are shed, but TZ sampling is the standard target.
Interventional & Abrasive Cytology — Brushings and Scrapings
Brushings, Scrapings, and FNAC in Diagnostic Cytology
When cells cannot be shed spontaneously, mechanical contact harvests them directly.
Brushings: A small brush is passed through an endoscope and rotated against a mucosal surface. Used for:
• Bronchial cytology (bronchoscopy) — superior to sputum for peripheral lesions accessible to the scope
• Oesophageal, gastric, and colonic cytology (upper and lower GI endoscopy)
• Biliary and pancreatic duct brushings (ERCP) — though sensitivity is limited (~40-50%)
The brush is then rolled onto a glass slide and immediately fixed.
Scrapings/Imprint cytology:
• Oral scraping — for leukoplakia, suspicious lesions of the buccal mucosa
• Conjunctival scraping — for trachoma (intracytoplasmic inclusions), allergic conjunctivitis (eosinophils)
• Skin scraping — for fungal elements (KOH mount + Tzanck smear for herpes, pemphigus)
• Tzanck smear — scraping from the base of a blister stained with Giemsa; demonstrates acantholytic cells (pemphigus) or multinucleated giant cells (herpes)
• Touch/imprint cytology — cut surface of a freshly excised tumour pressed onto a slide; gives an immediate intra-operative diagnosis