Page 2 of 18
PA7.1 | Diagnostic Cytology — SDL Guide (Part 2)
Fine Needle Aspiration Cytology (FNAC) — Technique and Applications
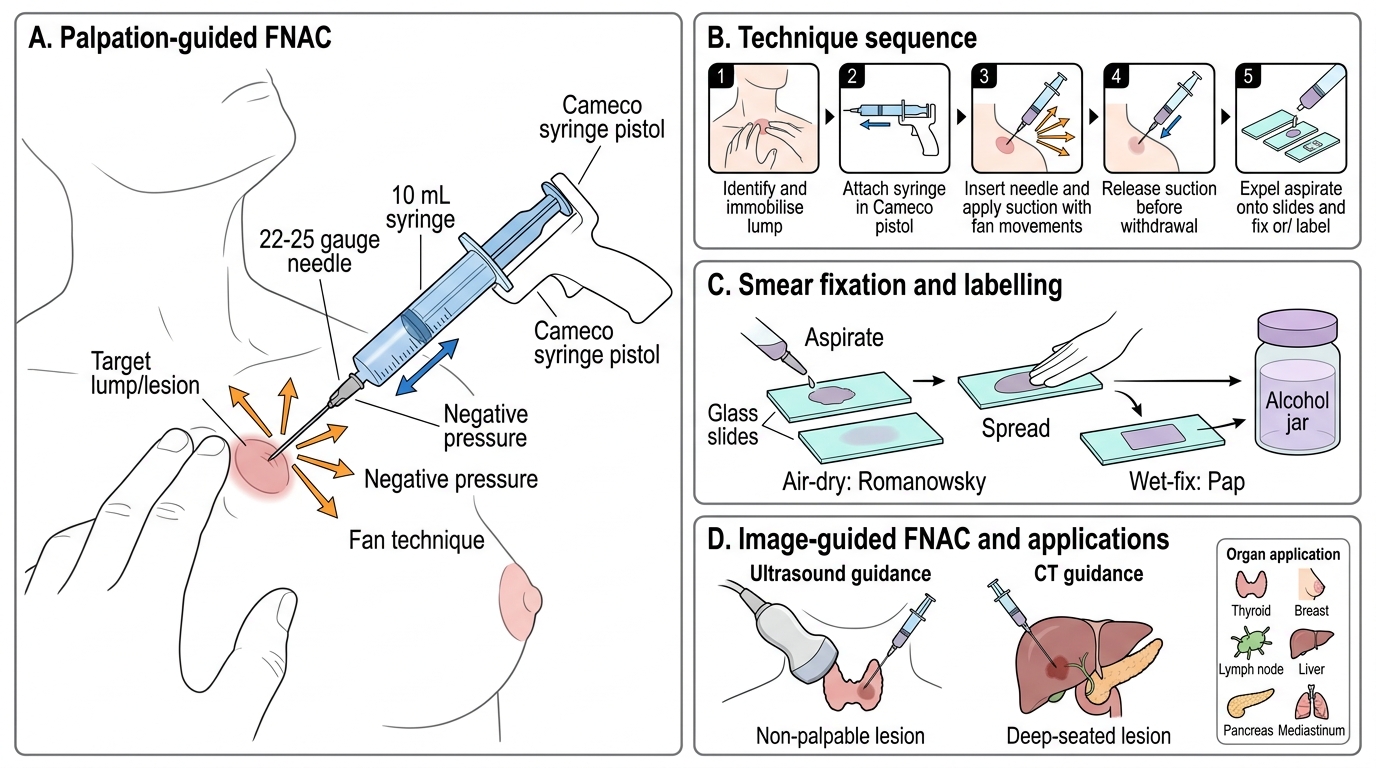
Fine Needle Aspiration Cytology (FNAC) is the most widely used interventional cytological technique. A fine needle (22–25 gauge) is introduced into a lesion and cells are aspirated by negative pressure.
Technique (standard palpation-guided FNAC):
1. Identify and immobilise the target lump between two fingers.
2. Attach a 10 mL or 20 mL syringe in a Cameco syringe pistol (one-handed aspiration).
3. Insert the needle, apply suction, and move the needle back and forth in multiple directions (fan technique) to sample different parts of the lesion.
4. Release suction before withdrawing the needle (prevents haemorrhagic dilution).
5. Expel aspirate onto 2–4 glass slides; smear, fix (air-dry for Romanowsky, wet-fix for Pap), and label immediately.
Image-guided FNAC:
• Ultrasound-guided — for non-palpable lesions (small thyroid nodules, retroperitoneal nodes, deep breast masses)
• CT-guided — for deep-seated lesions (pancreas, mediastinum, liver)
• Image guidance increases adequacy and reduces false-negative rates
FNAC applications by organ:
| Organ | Key cytological diagnoses | Note |
|---|---|---|
| Thyroid | Colloid nodule, follicular neoplasm, papillary carcinoma, Hashimoto's, anaplastic carcinoma | Cannot distinguish follicular adenoma from follicular carcinoma (needs capsule — histology required) |
| Breast | Fibroadenoma, fibrocystic change, carcinoma (ductal / lobular) | Triple test: clinical + imaging + FNAC |
| Lymph node | Reactive hyperplasia, granulomatous lymphadenitis (TB), metastatic carcinoma, lymphoma | Lymphoma subtyping needs histology + flow cytometry |
| Salivary gland | Pleomorphic adenoma, Warthin's tumour, mucoepidermoid carcinoma | Accurate for benign vs malignant distinction |
Advantages of FNAC:
• Outpatient procedure; no anaesthesia or sutures
• Result in hours (same day in ROSE centres)
• Low complication rate (haematoma, infection rare)
• Guides surgical planning — avoids unnecessary open biopsy
Rapid On-Site Evaluation (ROSE):
ROSE is immediate on-site assessment of smear adequacy by the cytopathologist during the FNAC procedure. The pathologist stains a quick Diff-Quik smear, confirms cell yield, and if adequate, the procedure ends. If inadequate, the needle pass is repeated. ROSE reduces non-diagnostic rates from ~20% to < 5% and is standard at academic centres and for CT/EUS-guided procedures.
Fine Needle Aspiration Cytology: Technique and Applications
CLINICAL PEARL
The thyroid FNAC paradox: FNAC is the gold standard for evaluating thyroid nodules and achieves > 90% sensitivity for papillary carcinoma (diagnostic nuclear features: ground-glass nuclei, nuclear grooves, pseudoinclusions). However, it cannot diagnose follicular carcinoma — the only criterion distinguishing follicular adenoma from follicular carcinoma is capsular or vascular invasion, which requires an intact histological section. So: a report of 'follicular neoplasm / Bethesda category IV' always mandates surgical excision and histology, regardless of cytological features.
Staining Methods in Cytology
Staining Methods in Cytology
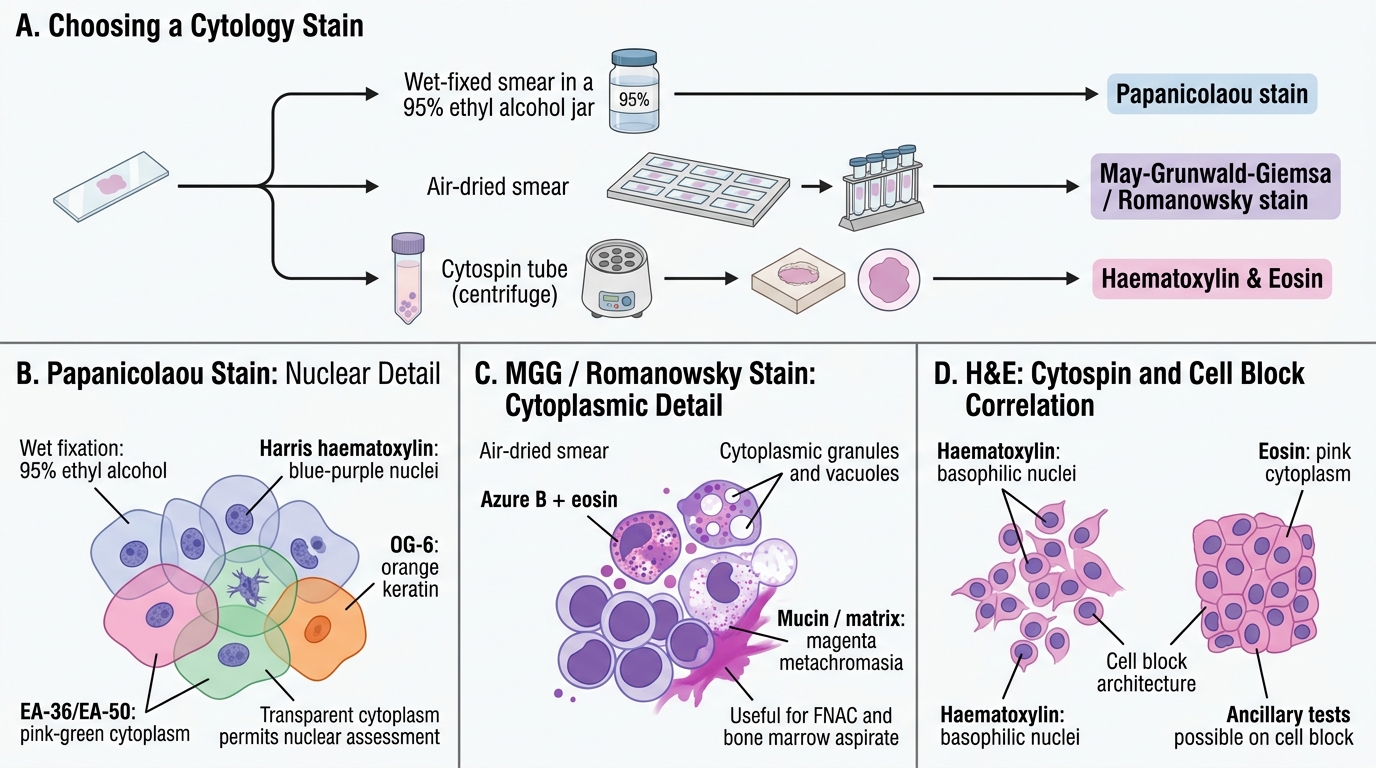
The choice of fixative and stain is determined by the specimen type and what diagnostic information is needed.
1. Papanicolaou Stain (Pap stain)
• Wet fixation (immediate immersion in 95% ethyl alcohol) — prevents air-drying artefact.
• Three-dye system: Harris haematoxylin (nuclear staining — blue/purple), OG-6 (eosinophilic keratin proteins — orange), EA-36/EA-50 (cytoplasmic counterstains — pink/green for metabolically active cells).
• Result: transparent cytoplasm with exquisite nuclear detail — chromatin texture, nucleoli, mitoses clearly visible.
• Ideal for: gynaecological smears, respiratory, urine, effusion cytology.
• Hallmark advantage: the transparency of cytoplasm allows nuclear assessment even in overlapping cells.
2. May-Grünwald-Giemsa (MGG) / Romanowsky stains
• Air-dried smears (not wet-fixed).
• Azure B + eosin dyes; stains metachromatic substances (mucin, cartilage matrix) magenta/pink.
• Gives excellent cytoplasmic detail — granules, vacuoles, mucin, haematopoietic cell morphology.
• Nuclear detail is less sharp than Pap, but cytoplasmic features and extracellular material are superior.
• Ideal for: FNAC smears (haematological lesions, lymph nodes, salivary gland mucin, cartilaginous matrix in pleomorphic adenoma), bone marrow aspirates.
3. Haematoxylin & Eosin (H&E)
• Standard histology stain; can also be applied to cytospin preparations and cell blocks.
• Cell block — cell-rich effusions/washings are centrifuged and the pellet is fixed in formalin, processed as a paraffin block, and sectioned. The H&E cell block allows immunohistochemistry (IHC) on cytological material.
4. Special Stains on Cytology Smears
• PAS (Periodic acid-Schiff) — glycogen (glycogen-rich carcinoma), mucin
• Ziehl-Neelsen (ZN) — acid-fast bacilli in FNA of tuberculous lymph nodes
• Grocott-Methenamine Silver (GMS) / PAS-D — fungal elements (Cryptococcus, Histoplasma)
• Alcian Blue — hyaluronic acid in mesothelioma
• Immunocytochemistry (ICC) — applied to cell blocks or fixed smears for cytokeratins, ER/PR/HER2 (breast), TTF-1 (lung/thyroid), PSA (prostate)
Comparative summary:
| Stain | Fixation | Best for | Nuclear detail |
|---|---|---|---|
| Papanicolaou | Wet (alcohol) | GYN, respiratory, urine | Excellent |
| MGG/Romanowsky | Air-dried | FNAC, haematology | Good |
| H&E (cell block) | Formalin | IHC, effusions | Good |
SELF-CHECK
A cytotechnician air-dries a cervical smear before Papanicolaou staining. What artefact will be seen and why?
A. Air-drying causes cellular enlargement and nuclear pale-out, mimicking HSIL
B. Air-drying causes nuclear condensation and hyperchromatism, falsely simulating carcinoma
C. No artefact — Pap stain works equally well on air-dried and wet-fixed smears
D. Cells will appear too transparent — the dye cannot penetrate dry, shrunken cytoplasm
Reveal Answer
Answer: A. Air-drying causes cellular enlargement and nuclear pale-out, mimicking HSIL
Air-drying artefact before Papanicolaou staining causes the cells to spread and flatten on the glass. The nucleus takes up more area and the chromatin appears pale ('washed out'), simulating the nuclear enlargement of a high-grade lesion. This is a common false-positive pitfall. Papanicolaou stain requires immediate wet fixation (95% ethyl alcohol within seconds of smear preparation) to preserve the transparent cytoplasm and crisp nuclear detail that make it diagnostically superior.
Cytological Criteria of Malignancy
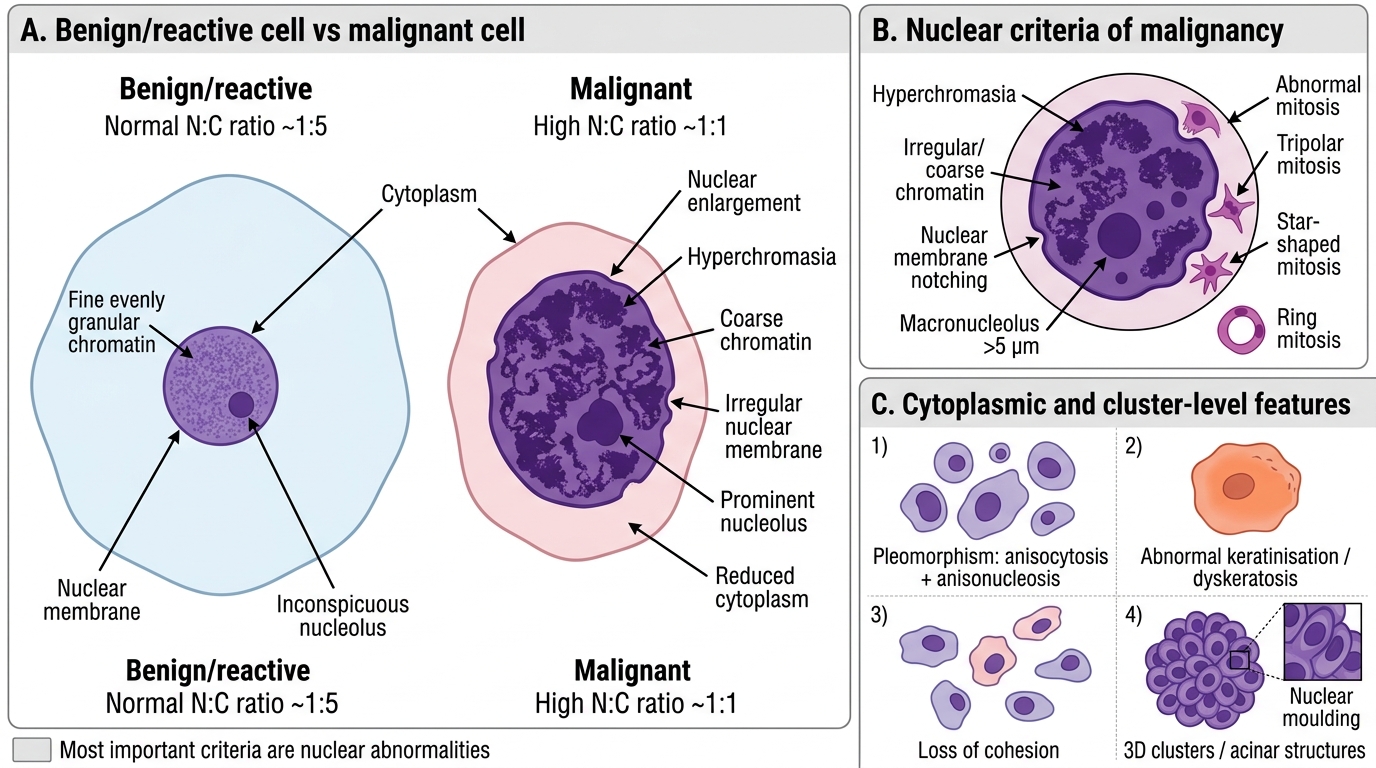
Distinguishing malignant cells from reactive or benign cells is the core interpretive skill in cytology. Malignant cells show several well-defined nuclear and cytoplasmic abnormalities.
Nuclear criteria (most important):
- Nuclear enlargement — malignant nuclei are disproportionately large for the cell size (increased absolute nuclear area)
- Increased N:C ratio (nucleus:cytoplasm ratio) — in normal squamous cells the N:C ratio is ~1:5; in malignant cells it may reach 1:1
- Hyperchromasia — dark staining due to increased DNA content (aneuploidy, polyploidy) and altered chromatin packaging
- Irregular/coarse chromatin — clumped, irregularly distributed (vs fine, evenly granular in reactive cells)
- Irregular nuclear membrane — notching, indentations, lobulations
- Prominent/irregular nucleoli — macronucleoli (> 5 µm), multiple nucleoli, irregular shapes
- Abnormal mitotic figures — tripolar, star-shaped, or ring mitoses
Cytoplasmic criteria:
8. Marked pleomorphism — variation in cell size (anisocytosis) and shape
9. Abnormal keratinisation — premature keratin production in individual malignant squamous cells (dyskeratosis)
10. Loss of cohesion — malignant epithelial cells lose cell-cell adhesion and occur singly (vs cohesive sheets in benign epithelium)
Cluster-level features:
11. 3D clusters / acinar structures — adenocarcinoma cells form 3D balls, papillary clusters
12. Nuclear moulding — nuclei shaped by adjacent nuclei (especially small-cell carcinoma)
Cytological Criteria of Malignancy
Important: No single criterion is pathognomonic. Interpretation integrates all criteria with clinical context, specimen adequacy, and background population of cells.