Page 3 of 18
PA7.1 | Diagnostic Cytology — SDL Guide (Part 3)
Liquid-Based Cytology (LBC) and Automation
Liquid-Based Cytology and Automated Screening
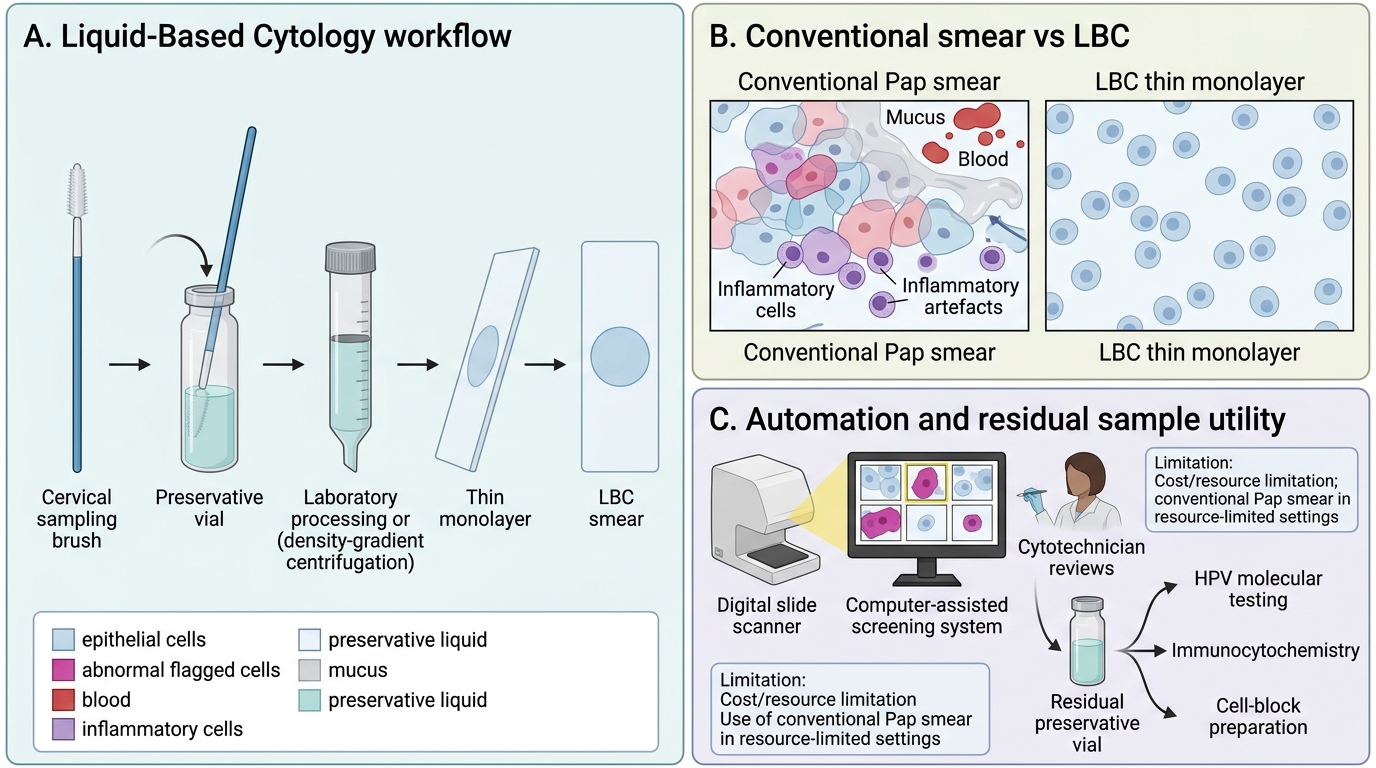
Liquid-based cytology (LBC) is a refinement of the conventional smear developed to reduce artefacts and improve cell preservation.
Technique:
1. Instead of smearing directly onto a slide, the brush is rinsed into a vial of preservative liquid (ThinPrep™ uses methanol-based PreservCyt; SurePath™ uses an ethanol-based fixative).
2. In the laboratory, cells are dispersed, contaminants (blood, mucus) are reduced by filtration or density gradient centrifugation, and a thin monolayer is deposited onto a glass slide.
Advantages over conventional smear:
• Fewer obscuring elements (blood, mucus, inflammatory cells)
• Cells preserved in near-native round morphology (not distorted by smearing)
• Residual liquid can be used for HPV molecular testing, immunocytochemistry, or cell-block preparation
• Standardised thin monolayer — easier for automated screening
• Longer shelf life
Automated screening (AI-assisted):
• ThinPrep Imaging System / BD FocalPoint — computer-assisted prescreening that ranks fields of view by probability of abnormality
• Cytotechnician reviews the flagged fields; reduces false-negatives from fatigue
• Artificial intelligence-based screening tools are now being validated for primary autonomous screening in high-volume national programmes
Limitation: LBC is more expensive than conventional smear; in resource-limited settings, conventional Pap smear remains the standard.
Diagnostic Role of Cytology — Applications, Screening, and When Biopsy is Still Needed
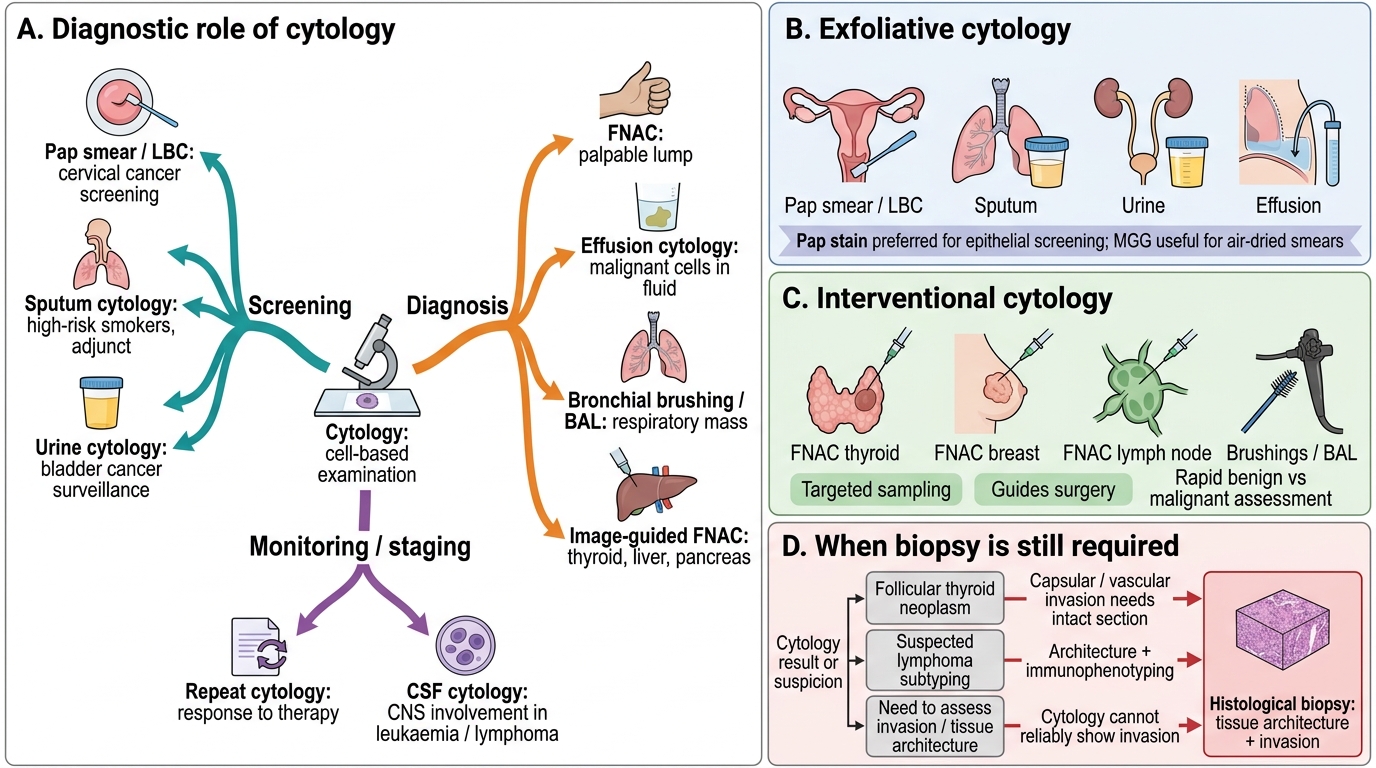
Cytology serves three overlapping clinical roles:
1. Screening (population-level)
• Cervical cancer: Pap smear / LBC — the paradigm of successful cancer screening; reduces mortality > 70% with organised programmes
• Lung cancer in high-risk smokers: sputum cytology (adjunct, lower sensitivity)
• Urothelial cancer surveillance: urine cytology for known bladder cancer follow-up
2. Diagnosis (individual patient)
• Palpable lump: FNAC → defines benign vs malignant, guides surgery
• Effusion: effusion cytology → detects metastatic deposits, lymphoma, mesothelioma
• Respiratory mass: bronchial brushing / BAL cytology
• Organ lesion (thyroid, liver, pancreas): image-guided FNAC
3. Monitoring and staging
• Repeat cytology to assess response to therapy (leukaemia, carcinoma in situ)
• CSF cytology for CNS involvement in leukaemia/lymphoma
Diagnostic Roles and Limits of Cytology
When histological biopsy is still required (cytology is NOT enough):
| Situation | Reason histology is needed |
|---|---|
| Follicular thyroid neoplasm | Capsular invasion only detectable on intact section |
| Lymphoma subtyping | Architecture + flow cytometry + IHC on intact node |
| Soft-tissue tumour grading | Extensive necrosis assessment, mitotic count per HPF |
| Assess surgical margins | Requires en bloc excision section |
| Inconclusive FNAC (Bethesda III or IV) | Risk-stratify before definitive surgery |
Remember: A positive cytology = cancer until proven otherwise. A negative cytology = low probability, but does NOT rule out malignancy (10-20% false-negative rate depending on site and technique). The triple test (clinical + imaging + cytology) reduces false-negatives in breast disease; all three must be concordant before proceeding conservatively.
CLINICAL PEARL
Reactive mesothelial cells vs metastatic adenocarcinoma in pleural fluid is among the most vexed differentials in cytopathology. Both form clusters, both have prominent nucleoli. The classic cytological clue: reactive mesothelial cells show intercellular windows (clear spaces between cells due to long microvilli), are arranged in flat sheets, and have a two-population pattern (larger and smaller cells in the same cluster). Adenocarcinoma cells form tight 3D acinar or papillary groups, show nuclear moulding, and the windows are absent. Whenever in doubt, a cell block with immunocytochemistry (Calretinin/WT-1 for mesothelial cells vs CEA/Ber-EP4 for adenocarcinoma) is definitive.
SELF-CHECK
On FNAC of a lymph node, the cytopathologist reports: 'Predominantly lymphoid cells with scattered epithelioid granulomas and Langhans-type giant cells; no acid-fast bacilli seen on ZN stain.' What is the most appropriate next step?
A. Reassure the patient — no ZN-positive bacilli means no tuberculosis
B. Immediately arrange surgical excision of the lymph node for histopathological confirmation of lymphoma
C. Report as reactive hyperplasia and discharge with antibiotics
D. Proceed to culture and molecular testing (GeneXpert) for Mycobacterium tuberculosis on the FNA material
Reveal Answer
Answer: D. Proceed to culture and molecular testing (GeneXpert) for Mycobacterium tuberculosis on the FNA material
Granulomatous lymphadenitis with Langhans giant cells is a classic FNAC pattern of TB lymphadenitis. ZN stain has only ~40-60% sensitivity on cytology smears; a negative ZN does NOT exclude TB. The correct next step is culture and molecular testing (GeneXpert MTB/RIF assay) on the FNA material, which can identify M. tuberculosis and rifampicin resistance within 2 hours with > 85% sensitivity. Histological excision is reserved for cases where cytology is non-diagnostic or lymphoma cannot be excluded.