Page 11 of 18
PA22.3-5 | Laboratory Panel Interpretation — SDL Guide (Part 3)
AKI vs CKD and the Prerenal/Renal/Postrenal Framework
AKI vs CKD and the Prerenal-Renal-Postrenal Framework
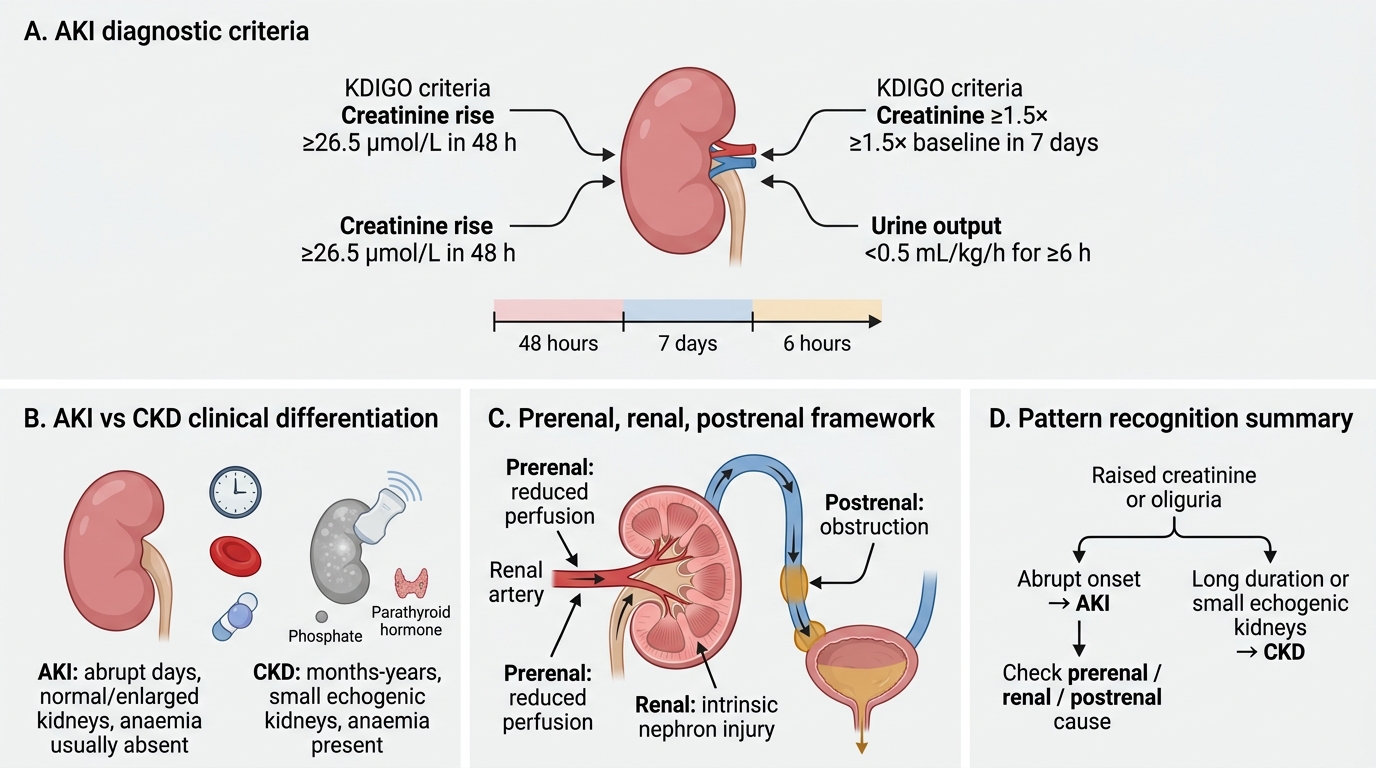
Acute kidney injury (AKI) is defined by KDIGO criteria as:
- Rise in creatinine ≥ 26.5 μmol/L within 48 hours, OR
- Rise to ≥ 1.5× baseline within 7 days, OR
- Urine output < 0.5 mL/kg/hr for ≥ 6 hours.
AKI vs CKD differentiation:
| Feature | AKI | CKD |
|---|---|---|
| Time course | Abrupt (days) | Chronic (months–years) |
| Anaemia | Absent (acute) | Yes (↓ erythropoietin) |
| Kidney size (USS) | Normal or enlarged | Small, echogenic, bilateral |
| Phosphate | Normal early | ↑ (hyperphosphataemia) |
| PTH | Normal | ↑ (secondary hyperparathyroidism) |
| Previous creatinine | Was normal | Elevated trend over time |
| Nails / skin / neurology | Absent | Uraemic features (late CKD) |
Prerenal / Renal / Postrenal framework for AKI:
Prerenal AKI (reduced perfusion → intact tubules try to conserve):
- Causes: haemorrhage, vomiting/diarrhoea, heart failure, burns, sepsis (distributive)
- Urea:creatinine ratio > 100 (high reabsorption)
- Urine Na⁺ < 20 mmol/L (tubular avid Na⁺ retention)
- Urine specific gravity > 1.020 (concentrated urine)
- Fractional excretion of Na⁺ (FENa) < 1%
- Responds to fluid resuscitation
Intrinsic renal AKI (tubular / glomerular / vascular injury):
- Causes: acute tubular necrosis (ATN — most common: ischaemia or nephrotoxins), glomerulonephritis, interstitial nephritis
- Urea:creatinine ratio 40–100 (tubules damaged → cannot concentrate urea)
- Urine Na⁺ > 40 mmol/L (tubules cannot reabsorb Na⁺)
- FENa > 2%
- Urine: granular casts (ATN), red cell casts (glomerulonephritis), eosinophils (interstitial nephritis)
Postrenal AKI (obstruction → back-pressure → bilateral renal impairment):
- Must be bilateral (or unilateral with single functioning kidney)
- Causes: BPH, bilateral ureteric stones, pelvic malignancy, retroperitoneal fibrosis
- Urea:creatinine ratio: variable
- Diagnosis confirmed by USS — bilateral hydronephrosis
- Post-obstruction diuresis after relief is an important complication
Worked example:
> 74-year-old male. Urea 32 mmol/L, creatinine 280 μmol/L → urea:creatinine ratio = 32/0.280 = 114 (> 100 in SI). eGFR 18 mL/min. Na⁺ 132 mmol/L, K⁺ 5.8 mmol/L. No previous records available.
> Pattern: markedly elevated urea:creatinine ratio suggests prerenal or postrenal obstruction (both cause tubular urea reabsorption). Hyperkalaemia + hyponatraemia consistent with AKI. In a 74-year-old male, obstruction from BPH must be excluded urgently — order USS abdomen/pelvis. Also assess volume status clinically.
SELF-CHECK
A 68-year-old woman with known hypertension has: creatinine 198 μmol/L today vs 90 μmol/L six months ago. Urea 18 mmol/L. Urea:creatinine ratio = 18/0.198 ≈ 91. Haemoglobin 9.1 g/dL (normocytic). USS: both kidneys 8.5 cm (small). K⁺ 5.4 mmol/L, phosphate 2.1 mmol/L (↑). Which best describes this patient?
A. Acute kidney injury, prerenal cause
B. Acute tubular necrosis
C. Chronic kidney disease with acute-on-chronic deterioration
D. Postrenal obstruction
Reveal Answer
Answer: C. Chronic kidney disease with acute-on-chronic deterioration
Multiple CKD markers are present: anaemia (↓ erythropoietin), elevated phosphate (impaired phosphate excretion), small bilateral kidneys on USS, and a documented rising creatinine trend over months. The ratio of 91 is within the normal/intrinsic range — not the > 100 expected in pure prerenal. The acute rise from 90 to 198 on a CKD background represents acute-on-chronic kidney disease, a common clinical scenario in hypertensive nephropathy. Postrenal needs hydronephrosis and is less likely in a woman without pelvic pathology described.
SELF-CHECK
Which urine electrolyte finding best distinguishes prerenal AKI from acute tubular necrosis (ATN)?
A. Urine Na⁺ > 40 mmol/L favours prerenal AKI
B. Urine Na⁺ < 20 mmol/L favours prerenal AKI
C. Urine Na⁺ is unreliable and should not be used
D. Urine Na⁺ > 40 mmol/L favours postrenal obstruction
Reveal Answer
Answer: B. Urine Na⁺ < 20 mmol/L favours prerenal AKI
In prerenal AKI, the tubules are intact and avidly reabsorb Na⁺ to restore circulating volume — urine Na⁺ < 20 mmol/L. In ATN, the tubular cells are damaged and cannot reabsorb Na⁺ — urine Na⁺ > 40 mmol/L. This is the physiological basis of the fractional excretion of Na⁺ (FENa): < 1% in prerenal, > 2% in ATN. Caveat: diuretics falsely raise urine Na⁺ in prerenal — use fractional excretion of urea instead if the patient is on diuretics.