Page 10 of 18
PA22.3-5 | Laboratory Panel Interpretation — SDL Guide (Part 2)
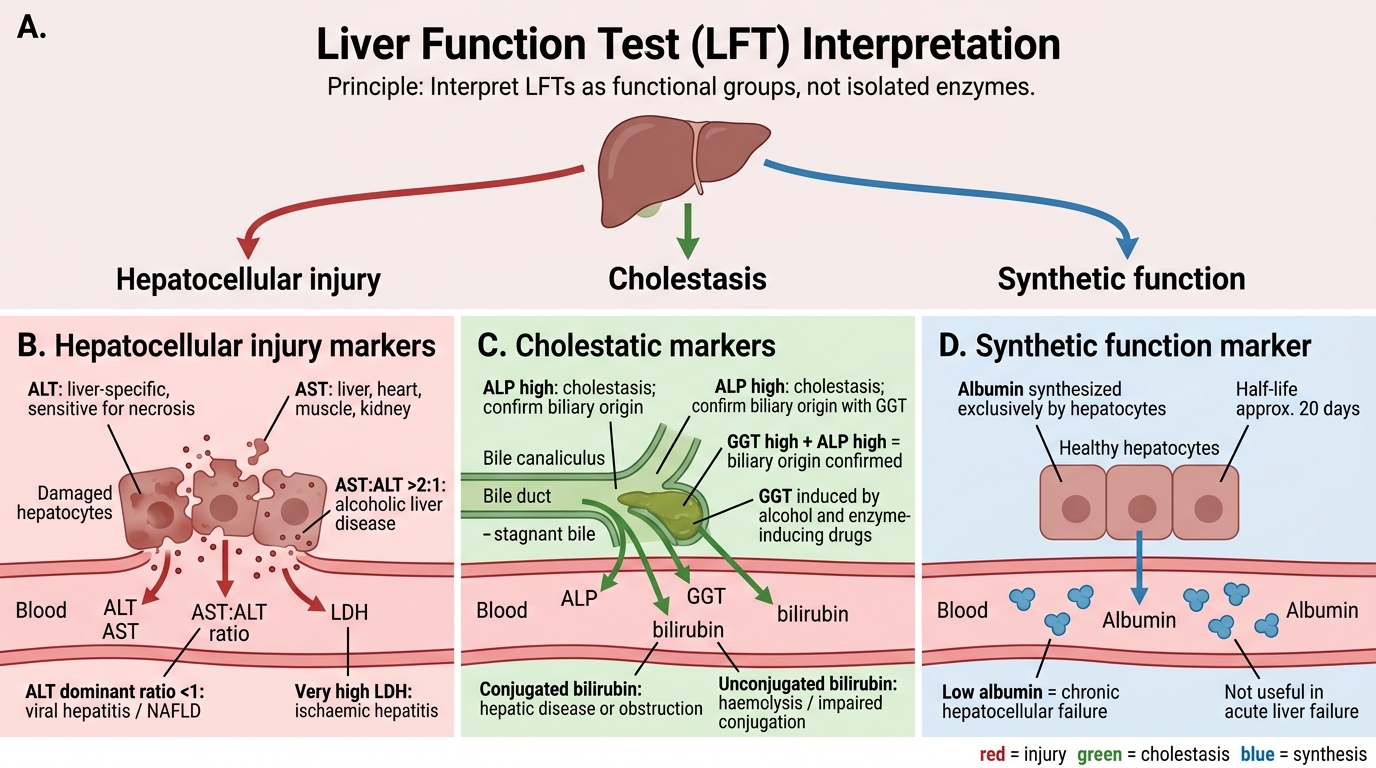
Liver Function Tests — Three Functional Groups
LFTs are best understood in three groups, not as a list of individual enzymes:
Group 1 — Hepatocellular injury markers:
• Alanine aminotransferase (ALT) — cytosolic, liver-specific; most sensitive marker of hepatocyte necrosis.
• Aspartate aminotransferase (AST) — found in liver, heart, muscle, kidney; less liver-specific.
• AST:ALT ratio — critical discriminator:
- Ratio > 2:1 strongly suggests alcoholic liver disease (alcohol induces mitochondrial AST release preferentially).
- Ratio < 1 (ALT dominant): viral hepatitis, non-alcoholic fatty liver disease (NAFLD).
• Lactate dehydrogenase (LDH) — non-specific; very high in ischaemic hepatitis ("shock liver").
Group 2 — Cholestatic markers:
• Alkaline phosphatase (ALP) — raised in cholestasis (and also in bone disease — confirm with GGT).
• Gamma-glutamyl transferase (GGT) — highly sensitive for cholestasis; also induced by alcohol and enzyme-inducing drugs. GGT ↑ + ALP ↑ = biliary origin confirmed.
• Bilirubin — distinguish conjugated (direct) from unconjugated (indirect):
- Unconjugated dominant: prehepatic (haemolysis) or impaired conjugation (Gilbert's, neonatal).
- Conjugated dominant: hepatic parenchymal disease or biliary obstruction.
- Mixed: most parenchymal diseases raise both.
Group 3 — Synthetic function markers:
• Albumin — synthesised exclusively in hepatocytes; half-life ~20 days. Low albumin reflects chronic hepatocellular failure. Not useful in acute liver failure (normal initially).
• Prothrombin time / INR — clotting factors II, VII, IX, X are made in the liver. PT/INR is the earliest and most sensitive indicator of acute synthetic failure (factor VII has a half-life of only 6 hours).
IMPORTANT NOTE: ALP is also elevated in bone disease (Paget's, osteomalacia, bone metastases) and in pregnancy (placental isoform). Always confirm liver origin with GGT.
Liver Function Tests: Three Functional Groups
LFT Patterns and Jaundice Classification
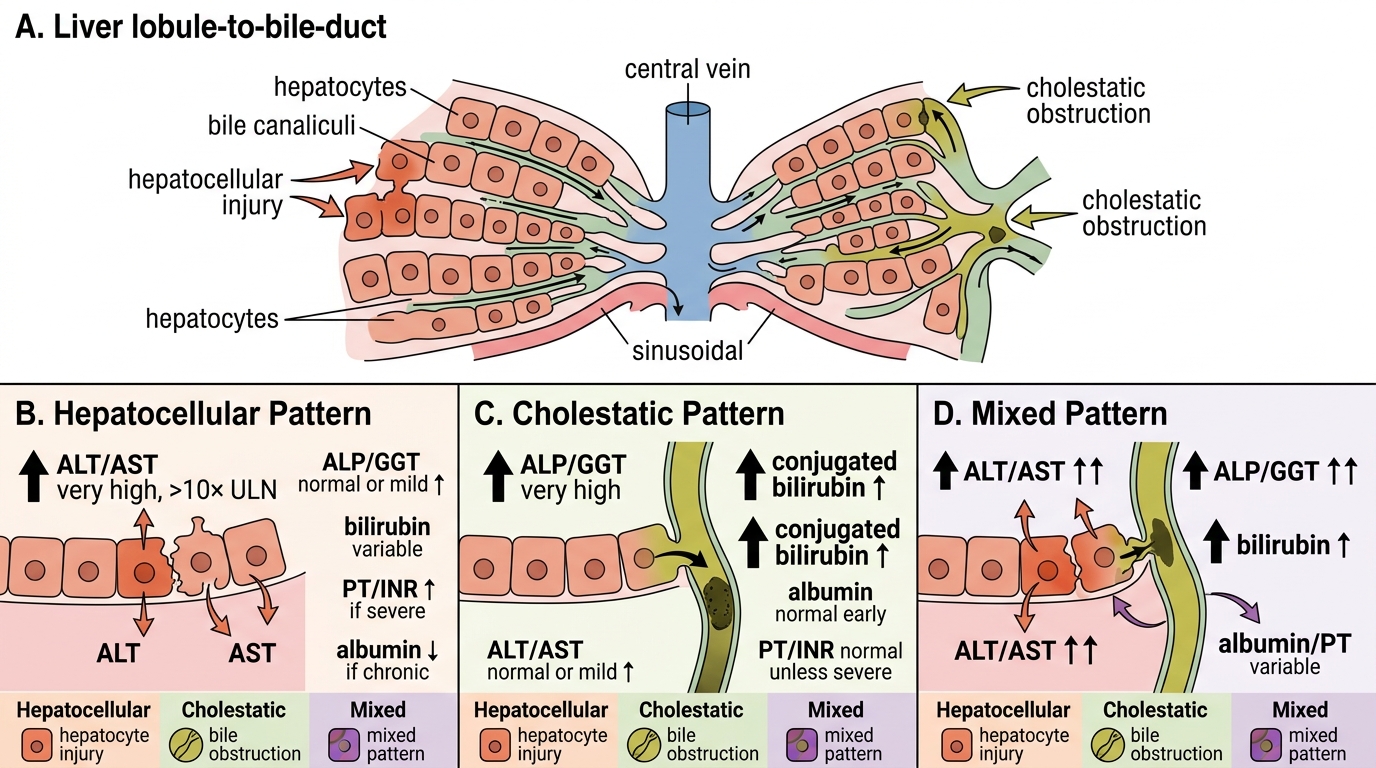
Pattern recognition — hepatocellular vs cholestatic vs mixed:
| Pattern | ALT/AST | ALP/GGT | Bilirubin | Albumin | PT/INR |
|---|---|---|---|---|---|
| Hepatocellular | ↑↑↑ (>10× ULN) | Normal or mildly ↑ | Variable | ↓ if chronic | ↑ if severe |
| Cholestatic | Normal or mildly ↑ | ↑↑↑ | ↑ (conjugated) | Normal early | Normal unless severe |
| Mixed | ↑↑ | ↑↑ | ↑ | Variable | Variable |
Jaundice classification by mechanism:
Prehepatic jaundice (haemolysis or ineffective erythropoiesis)
- Unconjugated bilirubin ↑↑ (not water-soluble → not in urine → acholuric jaundice)
- Urinary urobilinogen ↑↑ (excess bilirubin enters intestine → more urobilinogen reabsorbed)
- Urine bilirubin: absent
- LFTs (ALT, ALP, albumin, PT) — normal
- FBC: anaemia, reticulocytosis, peripheral blood film abnormalities
Hepatic jaundice (hepatocyte dysfunction — viral hepatitis, cirrhosis, drugs)
- Both conjugated and unconjugated bilirubin rise
- Urine bilirubin: present (conjugated is water-soluble)
- ALT/AST markedly elevated
- Albumin and PT abnormal in severe disease
Posthepatic (obstructive) jaundice (biliary obstruction — stones, carcinoma head of pancreas, cholangiocarcinoma)
- Conjugated bilirubin ↑↑ (water-soluble → in urine → dark urine)
- ALP and GGT ↑↑↑
- Pale/clay stools (no bile reaching gut), pruritus (bile salts in skin)
- Urinary urobilinogen: absent or very low
Worked example:
> 58-year-old male: AST 48, ALT 32 (AST:ALT ratio 1.5), ALP 420, GGT 680, total bilirubin 92 (conjugated 78), albumin 38 g/L (normal), PT 12 sec (normal). Dark urine. Pale stools.
> Pattern: ALP + GGT ↑↑↑, conjugated bilirubin dominant, dark urine, pale stools, normal synthetic function. → Posthepatic (obstructive) cholestasis. Next step: abdominal ultrasound for biliary dilation. The high GGT + ALP in an older male raises concern for carcinoma head of pancreas.
LFT Patterns and Jaundice Classification
SELF-CHECK
A 24-year-old medical student has episodic mild jaundice during exam stress. Labs: total bilirubin 38 μmol/L, unconjugated 34, ALT 18 U/L, ALP 72 U/L, albumin 42 g/L, PT 11 sec, Hb 14.2 g/dL (normal). Urine bilirubin: negative. Which diagnosis fits best?
A. Acute viral hepatitis
B. Obstructive jaundice from common bile duct stone
C. Gilbert's syndrome (benign unconjugated hyperbilirubinaemia)
D. Haemolytic anaemia
Reveal Answer
Answer: C. Gilbert's syndrome (benign unconjugated hyperbilirubinaemia)
The pattern: isolated unconjugated hyperbilirubinaemia, no urine bilirubin (unconjugated is lipid-soluble, not filtered), completely normal LFTs and PT, normal haemoglobin (excludes haemolysis). Triggered by fasting/stress. This is Gilbert's syndrome — a benign autosomal recessive UGT1A1 promoter variant that mildly impairs hepatic bilirubin conjugation. No treatment needed; the important task is distinguishing it from hepatitis and haemolysis.
CLINICAL PEARL
The AST:ALT ratio is one of the most powerful discriminators in hepatology, yet one of the most under-used in student practice.
- Ratio > 2:1 → alcoholic liver disease until proven otherwise. In alcoholic hepatitis, ALT rarely exceeds 300 U/L even in severe disease, while AST may be 600–800 U/L. This is because alcohol directly injures mitochondria (where AST resides) and also depletes pyridoxal phosphate, a cofactor for ALT synthesis.
- Ratio < 1 → viral or metabolic hepatitis. In acute hepatitis A or B, ALT typically exceeds AST because the viral cytopathic effect preferentially releases cytosolic enzymes.
- Ratio > 2:1 can also occur in Wilson's disease (copper-induced mitochondrial damage) and ischaemic hepatitis — context matters.
Always ask for the alcohol history before interpreting AST:ALT. The ratio is not a substitute for history, but it makes the pattern undeniable.
SELF-CHECK
A 50-year-old man is admitted with jaundice. Labs: AST 580 U/L, ALT 240 U/L, ALP 180 U/L (< 3× ULN), GGT 920 U/L, total bilirubin 85 μmol/L, albumin 28 g/L, PT 22 sec. The AST:ALT ratio is approximately:
A. 0.4 — suggesting viral hepatitis
B. 1.0 — indeterminate
C. 2.4 — suggesting alcoholic liver disease
D. Cannot be calculated from the data given
Reveal Answer
Answer: C. 2.4 — suggesting alcoholic liver disease
AST 580 ÷ ALT 240 = 2.4. A ratio > 2:1 strongly suggests alcoholic liver disease. The pattern is hepatocellular (dominant AST/ALT rise, ALP only mildly elevated). Low albumin and elevated PT indicate significant synthetic dysfunction — this is severe alcoholic hepatitis with compromised liver reserve. The markedly elevated GGT is also typical of alcohol-related liver disease. Clinical history of alcohol use should be sought urgently.
Renal Function Tests — Urea, Creatinine and eGFR
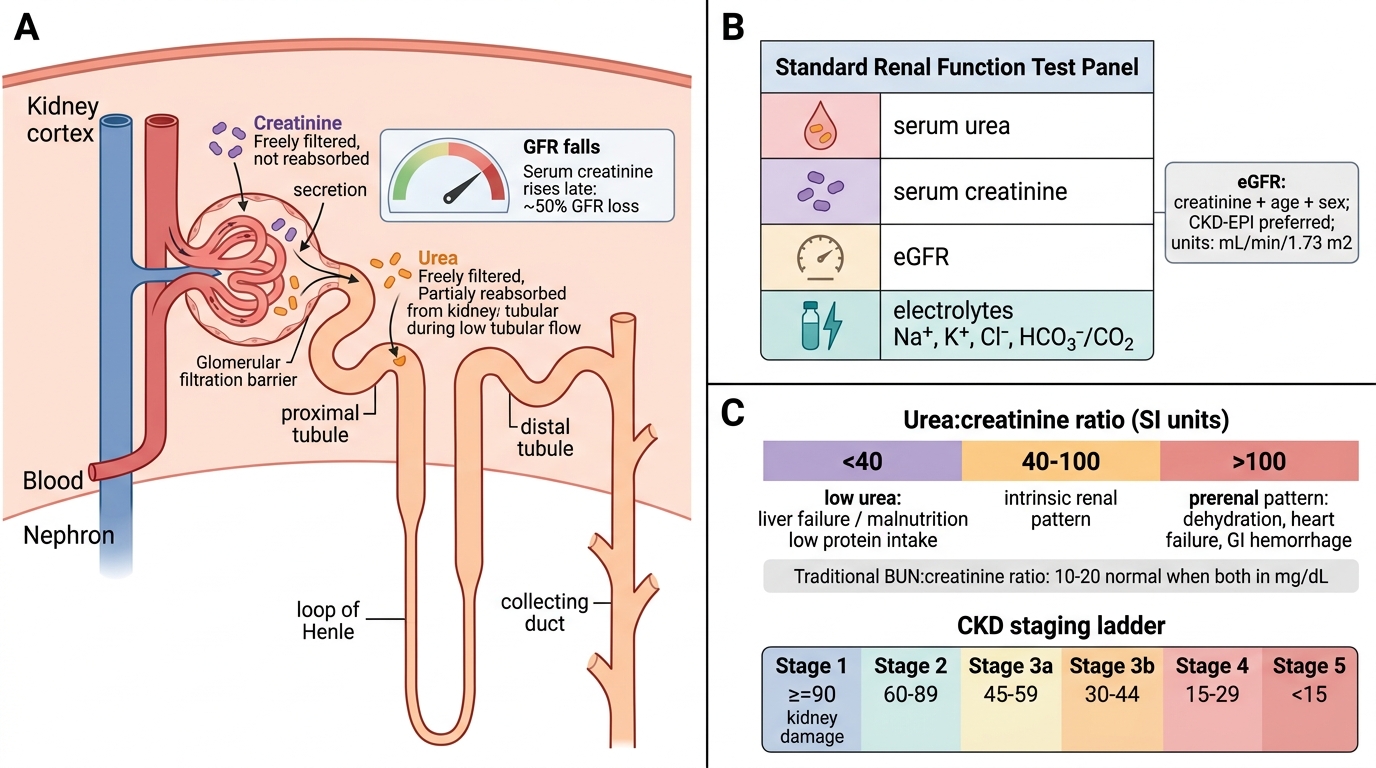
The standard RFT panel includes: serum urea, serum creatinine, estimated GFR (eGFR), and electrolytes (Na⁺, K⁺, Cl⁻, HCO₃⁻/CO₂).
Creatinine is a product of muscle creatine phosphate metabolism. It is freely filtered at the glomerulus and not reabsorbed (a small amount is secreted). Serum creatinine rises when GFR falls by ~50% — it is an insensitive early marker.
Urea is the main end-product of protein catabolism, synthesised in the liver. Urea is freely filtered but ~40–50% is passively reabsorbed in the tubules (more so when tubular flow is slow — prerenal state). This difference drives the urea:creatinine ratio.
Urea:creatinine ratio (both in mmol/L):
- Normal: approximately 40–100 (SI units) or 10–20 (if urea in mg/dL and creatinine in mg/dL — the traditional BUN:creatinine ratio used in many textbooks)
- > 100 (SI) → suggests prerenal cause (e.g. dehydration, heart failure, GI haemorrhage — high protein catabolism + tubular reabsorption of urea)
- 40–100 (SI) → intrinsic renal (tubular function impaired → less urea reabsorption; creatinine rises proportionately)
- < 40 (SI) → urea unusually low: liver failure (impaired urea synthesis), malnutrition, or low protein intake
eGFR is calculated from creatinine, age, and sex (CKD-EPI equation preferred). It is reported in mL/min/1.73 m². CKD staging uses eGFR:
- Stage 1: ≥90 (with other markers of kidney damage)
- Stage 2: 60–89
- Stage 3a: 45–59 / Stage 3b: 30–44
- Stage 4: 15–29
- Stage 5 (kidney failure): < 15
IMPORTANT NOTE: eGFR is unreliable in acute settings (steady-state creatinine required), in extreme muscle mass (bodybuilders: overestimate function; amputees: underestimate), and in pregnancy. In acute kidney injury, report actual creatinine and trend, not eGFR.
Renal Function Tests: Urea, Creatinine and eGFR