Page 5 of 18
PA22.1-2 | Urine & Body Fluid Analysis — SDL Guide
Learning Objectives
- Describe the physical, chemical, and microscopic findings in a complete urinalysis and correlate them with renal and systemic diseases.
- Distinguish dysmorphic from isomorphic red blood cells in urine sediment and state their clinical significance.
- Identify the major cast types in urine microscopy and name the disease state associated with each.
- Recognise common urine crystals and explain their clinical relevance.
- Distinguish a transudate from an exudate using Light's criteria and list causes for each.
- Compare CSF findings in bacterial, viral, tubercular, and fungal meningitis using the classic four-parameter table.
- Interpret synovial fluid analysis to differentiate gout from pseudogout.
- Apply the serum-ascites albumin gradient (SAAG) to differentiate causes of ascites.
INSTRUCTIONS
Laboratory analysis of body fluids is a cornerstone of clinical pathology. In daily ward practice, a carefully interpreted urine report can pinpoint the site of renal injury before imaging is done; a CSF report can be the difference between bacterial meningitis and a viral illness within 30 minutes. This module builds the systematic reading skills you need: from dipstick to microscopy, from pleural effusion biochemistry to CSF cell counts. Work through every micro-quiz actively — each is drawn directly from the kind of one-liner you will see in examinations and in clinics.
References
- Harsh Mohan, Textbook of Pathology, 8th ed., Ch 27 (Kidney) & Ch 28 (Lab Methods) (textbook)
- Robbins & Kumar, Basic Pathology, 11th ed., Ch 14 (Kidney) (textbook)
- Henry's Clinical Diagnosis and Management by Laboratory Methods, 24th ed., Ch 3 & Ch 29 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old presents with frothy urine, periorbital puffiness, and 3+ proteinuria on dipstick. The microscopy report returns: no casts seen, no RBCs. Another patient, same age, has smoky-brown urine, cola-coloured; microscopy shows dysmorphic RBCs and RBC casts. Both have 'abnormal urine' — but they could not be more different. One has nephrotic syndrome, the other nephritic syndrome. Knowing how to read the full urine report separates the two in under five minutes.
WHY THIS MATTERS
PA22.1 maps directly to urinalysis interpretation in renal and systemic disease — a skill tested in final MBBS theory, practicals, and clinics. PA22.2 covers body fluid analysis: pleural/peritoneal/CSF/synovial — fluids you will encounter on every general medicine, surgery, and neurology rotation. These are not abstract biochemistry; they are the reports you will be expected to act on as a houseman.
RECALL
Before proceeding, mentally rehearse:
• The nephron segments — glomerulus, proximal tubule, loop of Henle, distal tubule, collecting duct.
• The two main renal syndromes from Year-1 Physiology: nephritic (haematuria, oliguria, hypertension) vs nephrotic (massive proteinuria, hypoalbuminaemia, oedema, hyperlipidaemia).
• The normal glomerular filtration barrier: podocytes, GBM, endothelium — proteins >70 kDa are retained.
• From Biochemistry: glucose threshold (~180 mg/dL), ketone bodies (acetoacetate, β-hydroxybutyrate, acetone).
Physical Examination of Urine
Physical Examination of Urine
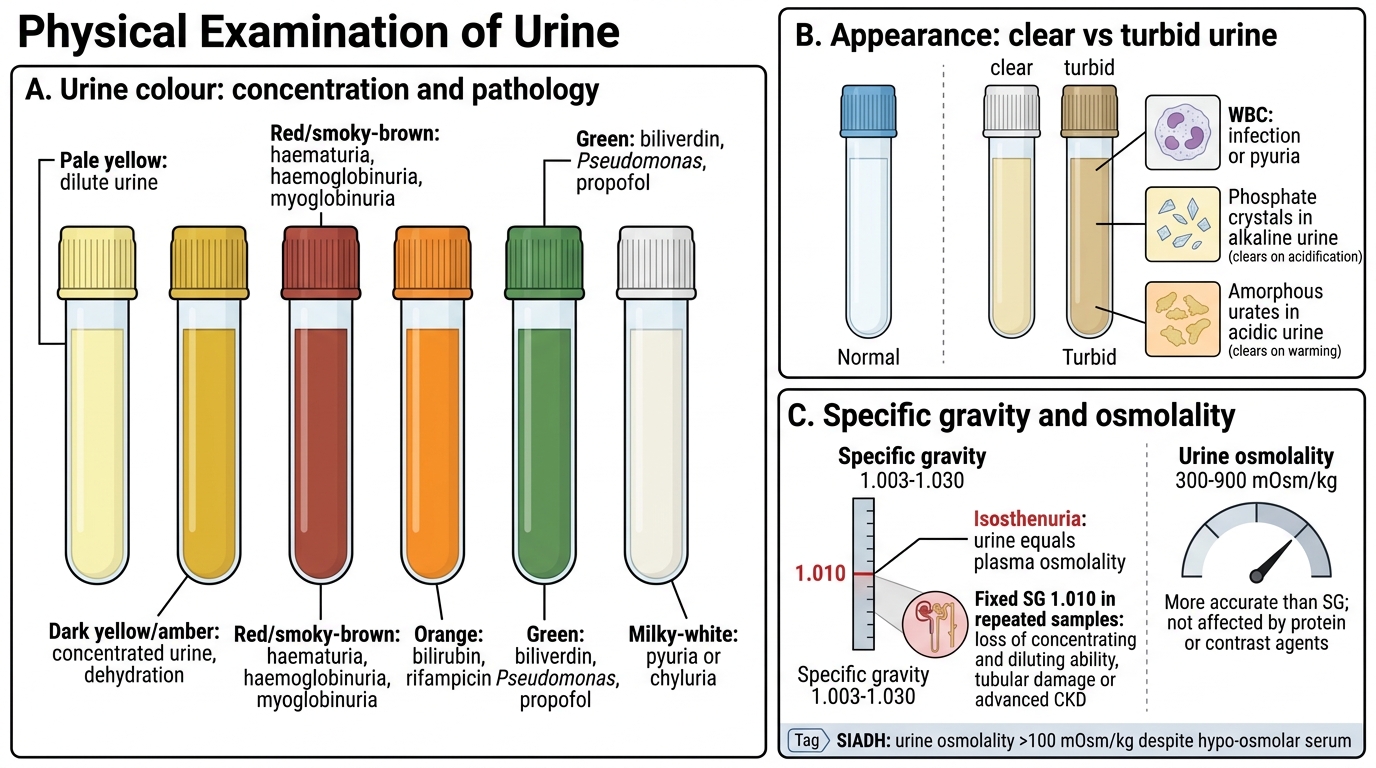
The physical examination of urine encompasses colour, appearance (clarity), specific gravity, and osmolality — quick observations made before any chemistry.
Colour reflects concentration and pathology:
• Pale yellow → dilute (diabetes insipidus, excess fluid intake)
• Dark yellow/amber → concentrated, dehydration
• Red/smoky-brown → blood (haematuria) or haemoglobinuria/myoglobinuria
• Orange → bilirubin (obstructive jaundice), rifampicin
• Green → biliverdin, Pseudomonas infection, propofol
• Milky-white → pyuria (WBCs) or chyluria (lymphatics)
Appearance (turbidity): Normal urine is clear. Turbidity indicates WBCs (infection), phosphate crystals (alkaline urine — clears on acidification), or amorphous urates (acid urine — clears on warming).
Specific gravity (SG): Normal 1.003–1.030. Measures solute concentration relative to water. SG 1.010 = isosthenuria (urine = plasma osmolality, seen in tubular damage). Fixed SG 1.010 in all samples indicates loss of concentrating and diluting ability — a sign of advanced chronic kidney disease (CKD).
Osmolality is more accurate than SG (not affected by large molecules like protein or contrast agents). Normal: 300–900 mOsm/kg. In SIADH, osmolality > 100 mOsm/kg despite hypo-osmolar serum.
SELF-CHECK
A patient with acute tubular necrosis has urine specific gravity fixed at 1.010 across multiple samples collected over 24 hours. What does this finding indicate?
A. The kidneys are concentrating urine appropriately
B. The tubules have lost both concentrating and diluting ability — urine osmolality equals plasma
C. The glomerular filtration rate is severely reduced
D. This is a normal finding in a well-hydrated patient
Reveal Answer
Answer: B. The tubules have lost both concentrating and diluting ability — urine osmolality equals plasma
Fixed SG 1.010 (isosthenuria) means the tubules can neither concentrate nor dilute the glomerular filtrate. The urine osmolality equals plasma osmolality (~290 mOsm/kg). This is the hallmark of tubular injury (ATN, advanced CKD) — the tubules are essentially 'blind' to ADH and other regulatory signals.
Chemical (Dipstick) Analysis
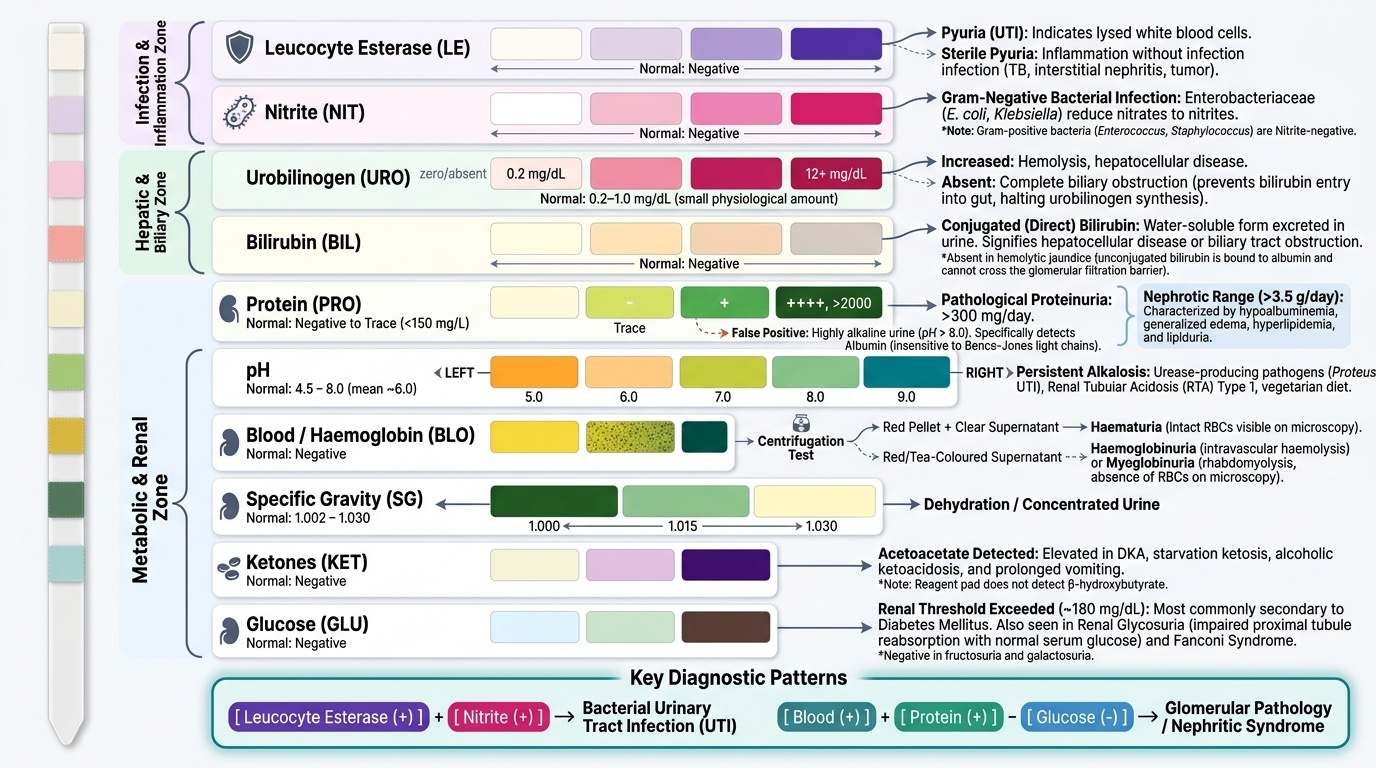
The dipstick simultaneously screens eight or more analytes using colorimetric pad reactions. Understanding the chemistry behind each pad helps you spot false positives and false negatives.
Provided image
pH: Normal 4.5–8.0 (mean ~6.0). Persistently alkaline → urease-producing organisms (Proteus UTI), RTA type 1, diet. Persistently acid → DKA, starvation, gout.
Protein: Dipstick detects albumin (threshold ~150–300 mg/L) via protein error of indicators. Insensitive to Bence-Jones protein (light chains) — needs SSA or urine protein electrophoresis. False positive: highly alkaline urine. Clinically significant: >300 mg/day is pathological. Nephrotic-range proteinuria = >3.5 g/day → hypoalbuminaemia, oedema, hyperlipidaemia, lipiduria.
Glucose: Dipstick positive only when plasma glucose exceeds the tubular threshold (~180 mg/dL). Causes: diabetes mellitus (commonest), renal glycosuria (low threshold, normal plasma glucose), Fanconi syndrome. Negative in fructosuria, galactosuria.
Ketones: Detects acetoacetate (not β-hydroxybutyrate). Positive in: diabetic ketoacidosis (DKA), starvation ketosis, alcoholic ketoacidosis, prolonged vomiting.
Blood/Haemoglobin: Reacts with haem peroxidase. Positive for: intact RBCs (haematuria), free haemoglobin (haemolysis, haemoglobinuria), myoglobin (rhabdomyolysis — the urine appears tea-coloured with no RBCs on microscopy). Distinguish: centrifuge urine — if supernatant stays red → haemoglobinuria; clear supernatant → haematuria (RBCs in pellet).
Bilirubin: Conjugated (direct) bilirubin is water-soluble → appears in urine. Unconjugated is albumin-bound → absent. Positive in: hepatocellular jaundice, obstructive jaundice. Absent in haemolytic jaundice.
Urobilinogen: Increased in haemolysis and hepatocellular disease. Absent in complete biliary obstruction (no bile → no urobilinogen in gut → none reabsorbed into blood).
Nitrites: Gram-negative bacteria (E. coli, Klebsiella) reduce nitrates → nitrites. Positive = probable GNB infection. Gram-positives (Enterococcus, Staphylococcus) are nitrite-negative.
Leucocyte esterase (LE): Released by lysed WBCs. Positive = pyuria. Sensitivity ~80% for UTI; can be positive in inflammation without infection (sterile pyuria → TB, interstitial nephritis, tumour).
IMPORTANT: Dipstick combination patterns guide diagnosis — LE+nitrite → bacterial UTI; blood+protein (no glucose) → glomerulonephritis; glucose+ketones → DKA; protein alone → nephrotic syndrome.
SELF-CHECK
A urine dipstick shows 3+ blood but microscopy reveals NO red blood cells. Plasma CK is markedly elevated. Which of the following best explains this dissociation?
A. The dipstick is falsely positive due to highly concentrated urine
B. Myoglobinuria from rhabdomyolysis — myoglobin reacts with the haem pad but is not a cell
C. Haemoglobinuria from intravascular haemolysis
D. Contamination of the sample with menstrual blood
Reveal Answer
Answer: B. Myoglobinuria from rhabdomyolysis — myoglobin reacts with the haem pad but is not a cell
The dipstick haem pad reacts with haem-containing proteins — haemoglobin AND myoglobin. In rhabdomyolysis, muscle breakdown releases myoglobin; it passes through the glomerulus (small molecule) and causes a positive haem reaction with no intact RBCs. The elevated CK confirms muscle injury. Centrifugation: clear supernatant (no haemolysis — no free Hb). This is myoglobinuria.
Urine Microscopy — Cells
Urine Microscopy: Cellular Findings
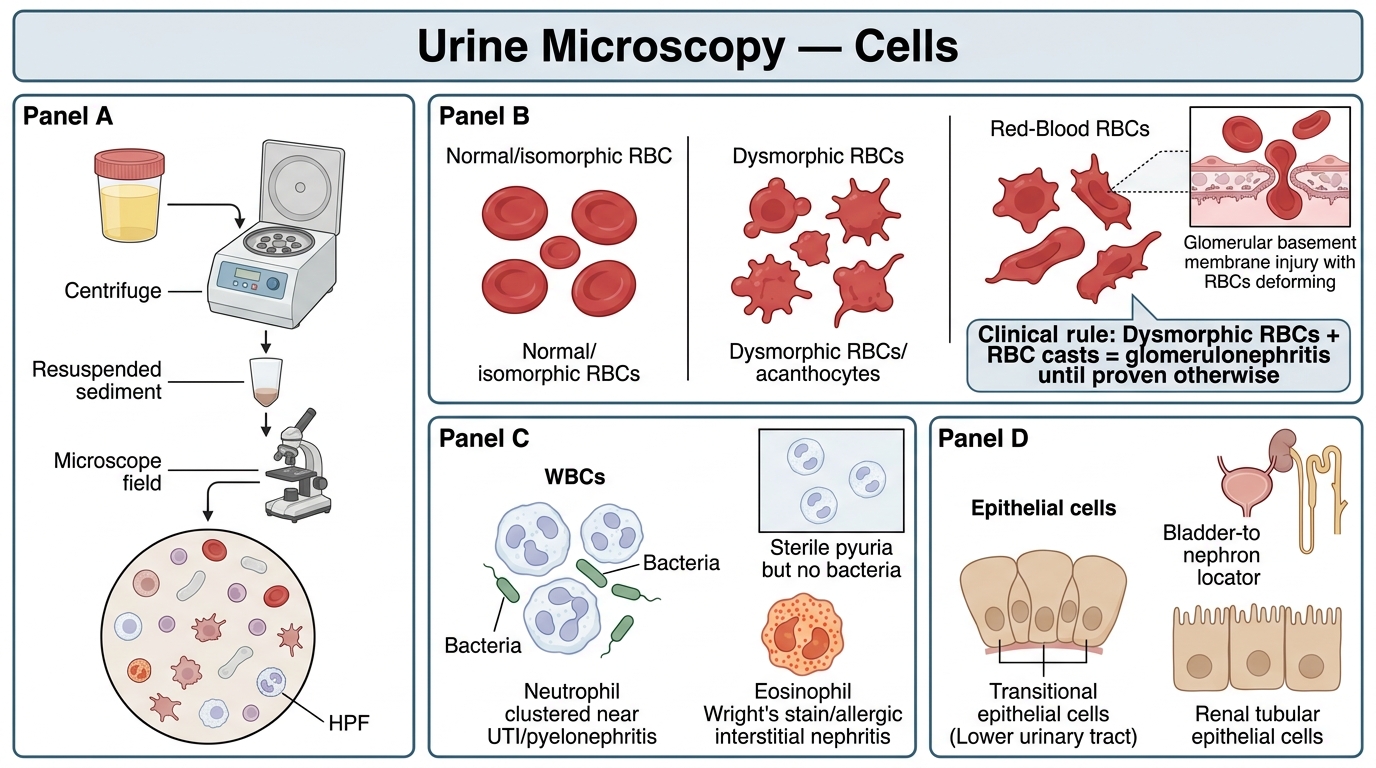
Urine is centrifuged (400×g, 5 min), the sediment resuspended, and examined under phase-contrast or bright-field microscopy. Reporting is per high-power field (HPF) for cells and casts.
Red blood cells (RBCs): Normal <2 RBCs/HPF. Greater than 3 is haematuria.
• Dysmorphic (acanthocytes/G1 cells): Irregular, blebs, protruding cytoplasmic protrusions. Caused by passage through damaged glomerular basement membrane → indicates glomerular origin (glomerulonephritis, vasculitis, IgA nephropathy). >5% acanthocytes or >80% dysmorphic RBCs is significant.
• Isomorphic: Uniform biconcave discs, indistinguishable from peripheral blood RBCs. Indicates lower urinary tract origin (UTI, stones, tumour, trauma, bleeding from bladder/urethra). Isomorphic haematuria with clots virtually never comes from glomeruli.
Clinical rule: dysmorphic RBCs + RBC casts = glomerulonephritis until proven otherwise.
White blood cells (WBCs/pyuria): Normal <5 WBCs/HPF (midstream catch). >10 WBCs/HPF = pyuria.
• Neutrophils → bacterial infection (UTI, pyelonephritis)
• Sterile pyuria (positive LE, no bacterial growth on culture): renal TB, analgesic nephropathy, interstitial nephritis, chlamydial urethritis, partially treated UTI.
• Eosinophiluria (Wright's stain) → allergic interstitial nephritis (drug-induced: NSAIDs, penicillins, cephalosporins).
Epithelial cells:
• Transitional epithelial cells → lower tract; large numbers suggest bladder pathology.
• Renal tubular epithelial cells (RTE cells) → tubular injury (ATN, nephrotoxins); clumped in oval fat bodies in nephrotic syndrome.
• Squamous epithelials → contamination from vaginal/perianal skin; invalidate the specimen if numerous.