Page 6 of 18
PA22.1-2 | Urine & Body Fluid Analysis — SDL Guide (Part 2)
Urine Microscopy — Casts
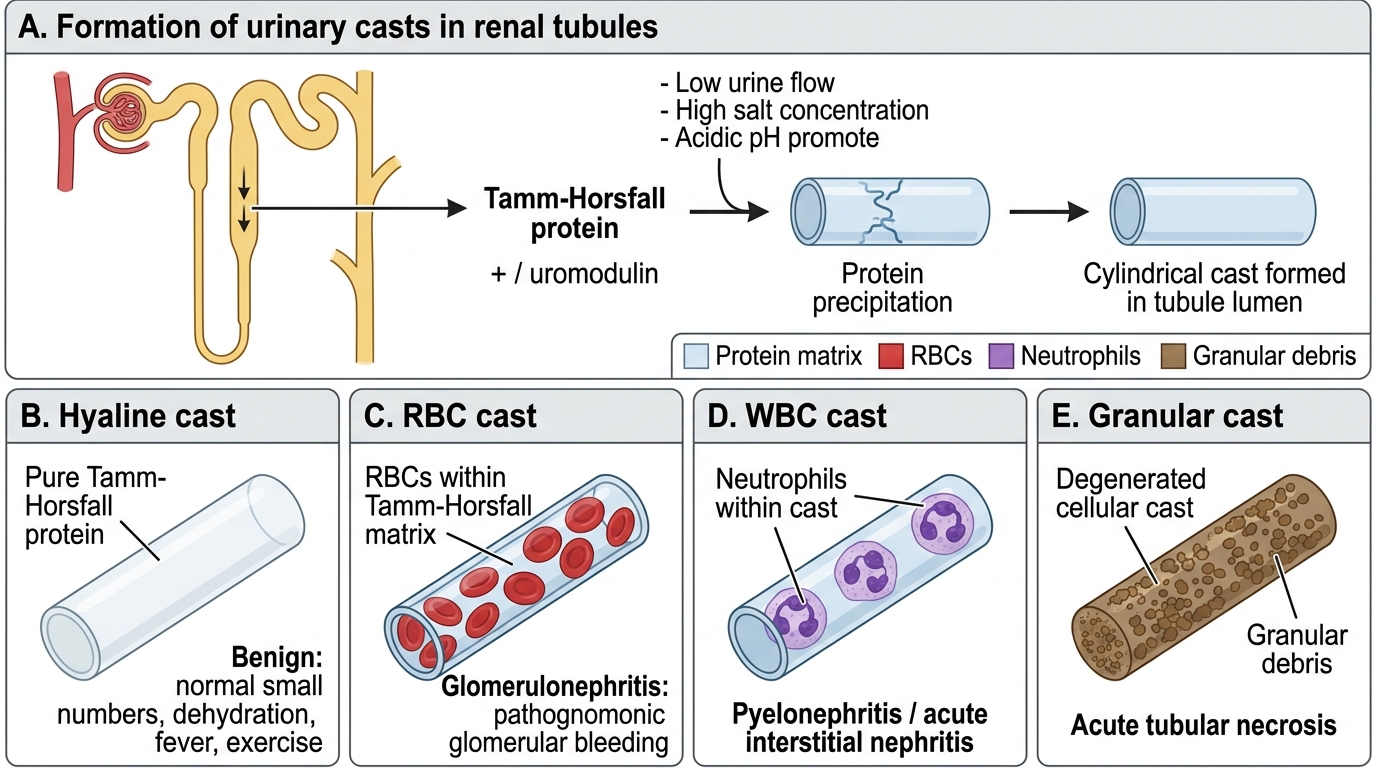
Casts are cylindrical moulds of the renal tubule lumen, formed by precipitation of Tamm-Horsfall protein (uromodulin) secreted by the thick ascending loop and early DCT. Low urine flow, high salt, and acidic pH promote cast formation. Their composition and shape carry diagnostic weight.
| Cast type | Composition | Disease association |
|---|---|---|
| Hyaline | Pure Tamm-Horsfall protein, transparent | Normal in small numbers; dehydration, fever, vigorous exercise — benign |
| RBC casts | Tamm-Horsfall + red blood cells | Glomerulonephritis (post-streptococcal GN, IgA, lupus nephritis, Goodpasture's) — pathognomonic of glomerular bleeding |
| WBC casts | Tamm-Horsfall + neutrophils | Pyelonephritis (upper UTI), acute interstitial nephritis |
| Granular casts | Degenerated cellular casts ('muddy brown') | Acute tubular necrosis — the 'muddy brown granular cast' is ATN until proven otherwise |
| Waxy/broad casts | Highly refractive, wide diameter | Chronic kidney disease (advanced, slow urine flow in dilated tubules) |
| Fatty casts / oval fat bodies | Lipid-laden tubular cells; Maltese cross under polarised light | Nephrotic syndrome (massive lipiduria) |
| Epithelial cell casts | Desquamated tubular cells | ATN, heavy metal toxicity, viral nephritis |
Memory peg: Hypertension = Hyaline (benign), Red = gloRmis (glomerulonephritis), White = pyelo (Whiteblood/pyelonephritis), Granular = ATN (Granular/muddy), Waxy = CKD (Waxy = wasted kidneys).
Urinary Casts: Formation, Types, and Clinical Significance
SELF-CHECK
Phase-contrast microscopy of urine from a 28-year-old with acute oliguria after an episode of haemolysis shows numerous 'muddy-brown' granular casts. WBC casts and RBC casts are absent. Which diagnosis does this best support?
A. Post-streptococcal glomerulonephritis
B. Acute pyelonephritis
C. Acute tubular necrosis
D. Lupus nephritis class IV
Reveal Answer
Answer: C. Acute tubular necrosis
Muddy-brown granular casts are the classic finding of acute tubular necrosis (ATN). They represent degenerated epithelial cells and cellular debris entrapped in Tamm-Horsfall protein, appearing as opaque brown cylinders. RBC casts are pathognomonic of glomerulonephritis; WBC casts indicate pyelonephritis. In ATN, the glomeruli are structurally intact — the injury is tubular — hence no RBC or WBC casts.
Urine Crystals
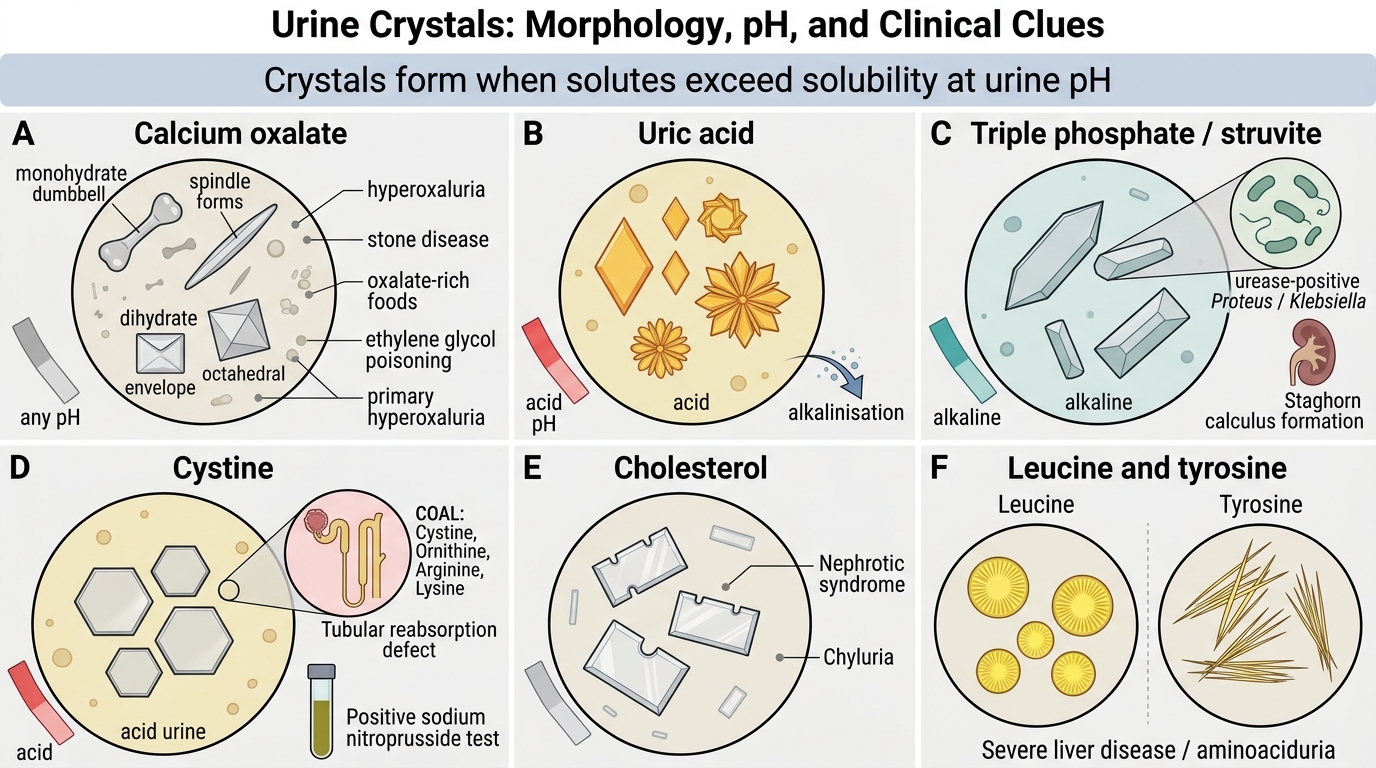
Crystals form when solutes exceed their solubility at the urine pH. Most crystals are incidental; a few are diagnostically critical.
Calcium oxalate (monohydrate — envelope/dumbbell; dihydrate — envelope/square):
• Most common crystal, seen at any pH.
• Monohydrate form: dumbbell or spindle-shaped — more associated with hyperoxaluria and stone disease.
• Dihydrate: classic envelope (octahedron). Seen after eating oxalate-rich foods (spinach, rhubarb), ethylene glycol poisoning (massive monohydrate crystals in ATN), or primary hyperoxaluria.
Uric acid (yellow-orange rhomboid/rosette, acid pH):
• Seen in gout, hyperuricaemia, myeloproliferative disorders, Lesch-Nyhan syndrome, high purine diet.
• Dissolve if urine is alkalinised — useful therapeutic manoeuvre.
Triple phosphate / struvite (coffin-lid, alkaline pH):
• Magnesium ammonium phosphate. Form only in alkaline urine produced by urease-splitting organisms (Proteus, Klebsiella).
• Grow to fill the renal pelvis → staghorn calculi (also called infection stones).
Cystine (hexagonal plates, acid pH):
• Pathognomonic of cystinuria — autosomal recessive defect in tubular reabsorption of dibasic amino acids (COAL: Cystine, Ornithine, Arginine, Lysine).
• Positive sodium nitroprusside (Brand's) test on urine. Treat by alkalinisation + high fluid intake.
Cholesterol (notched rectangular plates): Nephrotic syndrome, chyluria.
Leucine (yellow spheroids with radial striations) and Tyrosine (fine needles in sheaves): Severe hepatic failure (overflow aminoaciduria).
Urine Crystals: Morphology and Clinical Significance
CLINICAL PEARL
Gout vs pseudogout: In synovial fluid analysis, polarised-light microscopy is the key discriminator. Monosodium urate (MSU) crystals (gout) are needle-shaped and negatively birefringent — they appear yellow when parallel to the slow axis of the compensator (mnemonic: gout = yellow when parallel = 'y-ellow p-arallel'). Calcium pyrophosphate dihydrate (CPPD) crystals (pseudogout/chondrocalcinosis) are rhomboid-shaped and positively birefringent — blue when parallel. The shape difference alone (needle vs rhomboid) distinguishes them under ordinary light if polarisation is unavailable.
SELF-CHECK
Urine microscopy from a 45-year-old with recurrent renal calculi shows flat hexagonal crystals that are birefringent under polarised light. Urine pH is 5.5. Which metabolic disorder does this finding indicate?
A. Primary hyperoxaluria
B. Xanthinuria
C. Cystinuria — autosomal recessive defect in dibasic amino acid transport
D. Hyperuricosuria from gout
Reveal Answer
Answer: C. Cystinuria — autosomal recessive defect in dibasic amino acid transport
Hexagonal (benzene-ring shaped) crystals in acid urine are pathognomonic of cystinuria. The defect is in the SLC3A1/SLC7A9 transporter responsible for tubular reabsorption of cystine, ornithine, arginine, and lysine (COAL). Calcium oxalate crystals are envelope-shaped; uric acid crystals are rhomboid/rosette in acid urine; xanthine crystals are amorphous yellow-brown.
Urine Patterns in Disease — Nephritic vs Nephrotic
Nephritic vs Nephrotic Urine Patterns
Two syndromic patterns are the cornerstone of nephrology interpretation:
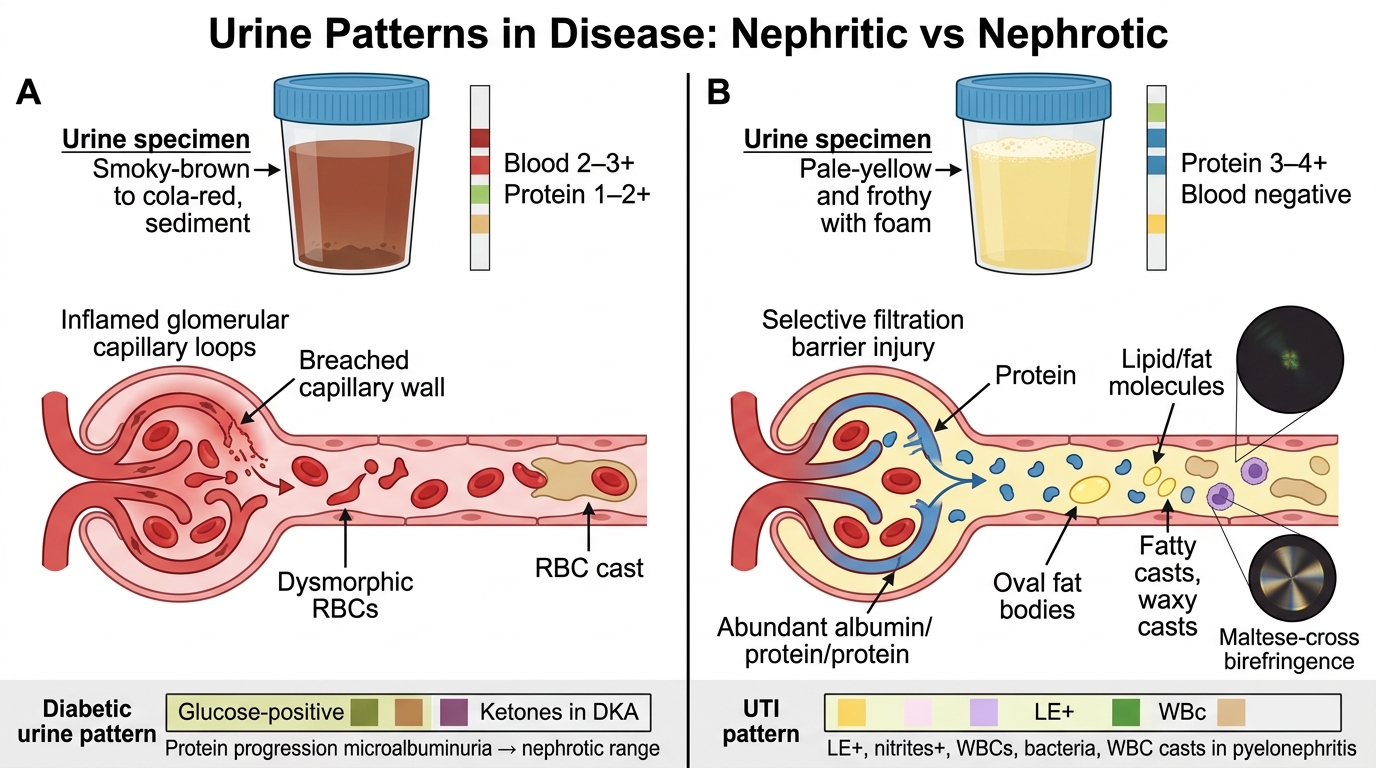
Nephritic syndrome urine:
• Colour: smoky-brown, cola, or frank red haematuria
• Dipstick: blood 2–3+, protein 1–2+ (non-selective, moderate)
• Microscopy: dysmorphic RBCs, RBC casts (hallmark), WBC casts (if proliferative inflammation)
• Causes: post-streptococcal GN, IgA nephropathy, lupus nephritis, anti-GBM disease, MPGN
• Mechanism: glomerular inflammation → capillary wall breach → RBCs pass into tubule → casts form
Nephrotic syndrome urine:
• Colour: frothy (foam test for protein), pale-yellow
• Dipstick: protein 3–4+ (selective in minimal change disease — mostly albumin; non-selective in others), glucose absent unless DM
• Microscopy: oval fat bodies (lipid-laden tubular cells), fatty casts, waxy casts, Maltese-cross birefringence under polarised light
• RBCs and RBC casts are typically absent (glomerular wall is damaged selectively for charge/size — not torn)
• Causes: minimal change disease (children), FSGS, membranous GN, diabetic nephropathy, amyloidosis
DM urine pattern: Glucose positive (above threshold), ketones positive in DKA, protein positive when diabetic nephropathy develops (microalbuminuria → macroalbuminuria → nephrotic range).
UTI urine pattern: Dipstick LE+, nitrites+; microscopy WBCs, bacteria, WBC casts if upper tract (pyelonephritis); epithelial cells from trigone.