Page 7 of 18
PA22.1-2 | Urine & Body Fluid Analysis — SDL Guide (Part 3)
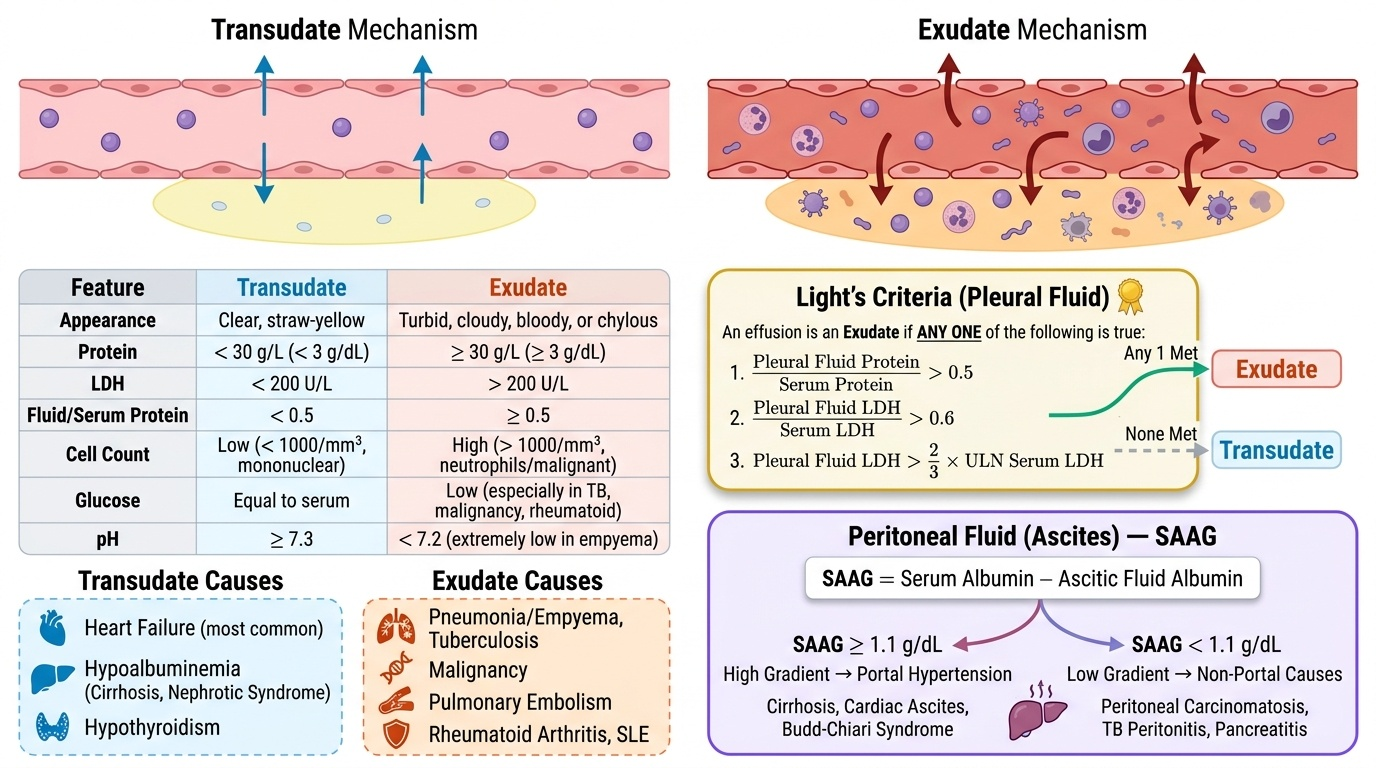
Pleural and Peritoneal Effusions — Transudate vs Exudate
Effusions accumulate when the balance of hydrostatic/oncotic forces is disrupted (transudate) or when inflammation/infection/malignancy damages the membrane (exudate). The clinical and analytical distinction is essential because management differs entirely.
Provided image
Light's criteria (1972, still the gold standard for pleural fluid):
An effusion is an exudate if ANY ONE of these is true:
1. Pleural fluid protein / serum protein > 0.5
2. Pleural fluid LDH / serum LDH > 0.6
3. Pleural fluid LDH > 2/3 upper limit of normal serum LDH
If NONE is met → transudate.
| Feature | Transudate | Exudate |
|---|---|---|
| Protein | <30 g/L (<3 g/dL) | >30 g/L (>3 g/dL) |
| LDH | <200 U/L | >200 U/L |
| Fluid/serum protein ratio | <0.5 | >0.5 |
| Appearance | Clear, straw-yellow | Turbid, cloudy, haemorrhagic, chylous |
| Cell count | <1000/mm³ (mostly mononuclear) | >1000/mm³ |
| Glucose | = serum | Low (TB, malignancy, rheumatoid) |
| pH | >7.3 | <7.2 (empyema, TB, malignancy) |
Transudate causes: Heart failure (most common), hypoalbuminaemia (cirrhosis, nephrotic syndrome), hypothyroidism, Meigs' syndrome.
Exudate causes: Infection (parapneumonic/empyema), malignancy, TB, pulmonary embolism, autoimmune (SLE, RA), chylothorax.
Peritoneal fluid (ascites) — SAAG (Serum-Ascites Albumin Gradient): SAAG = serum albumin − ascitic fluid albumin.
• SAAG ≥1.1 g/dL → portal hypertension (cirrhosis, cardiac ascites, Budd-Chiari syndrome)
• SAAG <1.1 g/dL → non-portal causes (malignancy, TB peritonitis, nephrotic syndrome, pancreatitis)
Note: Light's criteria are for pleural fluid. SAAG (not Light's) is the preferred tool for ascites, as it reflects the underlying haemodynamic mechanism rather than membrane permeability.
Empyema: Frank pus. pH <7.0, glucose <2.2 mmol/L, LDH extremely elevated. WBCs predominantly neutrophils (>10,000/mm³). Requires drainage + antibiotics.
Haemorrhagic effusion: Haematocrit fluid/blood >50% → haemothorax. RBC count >100,000/mm³ suggests trauma, malignancy, pulmonary infarction.
SELF-CHECK
Pleural fluid analysis: protein 42 g/L, serum protein 65 g/L, pleural LDH 280 U/L, serum LDH 310 U/L (upper limit of normal = 220 U/L). Applying Light's criteria, which of the following is correct?
A. Transudate — because total fluid protein is less than 50 g/L
B. Exudate — pleural/serum protein ratio is 0.65 (>0.5) AND LDH is >2/3 ULN
C. Cannot be determined without glucose and pH
D. Transudate — only LDH ratio matters in Light's criteria
Reveal Answer
Answer: B. Exudate — pleural/serum protein ratio is 0.65 (>0.5) AND LDH is >2/3 ULN
Light's criteria require only ONE criterion to be met for exudate. Criterion 1: 42/65 = 0.65 > 0.5 → exudate. Criterion 3: pleural LDH 280 > 2/3 × 220 = 147 → exudate. Two of three Light's criteria are positive. The full diagnostic picture (glucose, pH, cytology) refines the cause but is not needed to classify the effusion type.
CSF Analysis — Normal vs Meningitis Patterns
Cerebrospinal fluid (CSF) is produced by the choroid plexus (~500 mL/day, circulating volume ~150 mL). Normal opening pressure: 7–18 cm H₂O (lateral decubitus). Analysis includes appearance, cell count and differential, protein, and glucose (always with simultaneous serum glucose).
Provided image
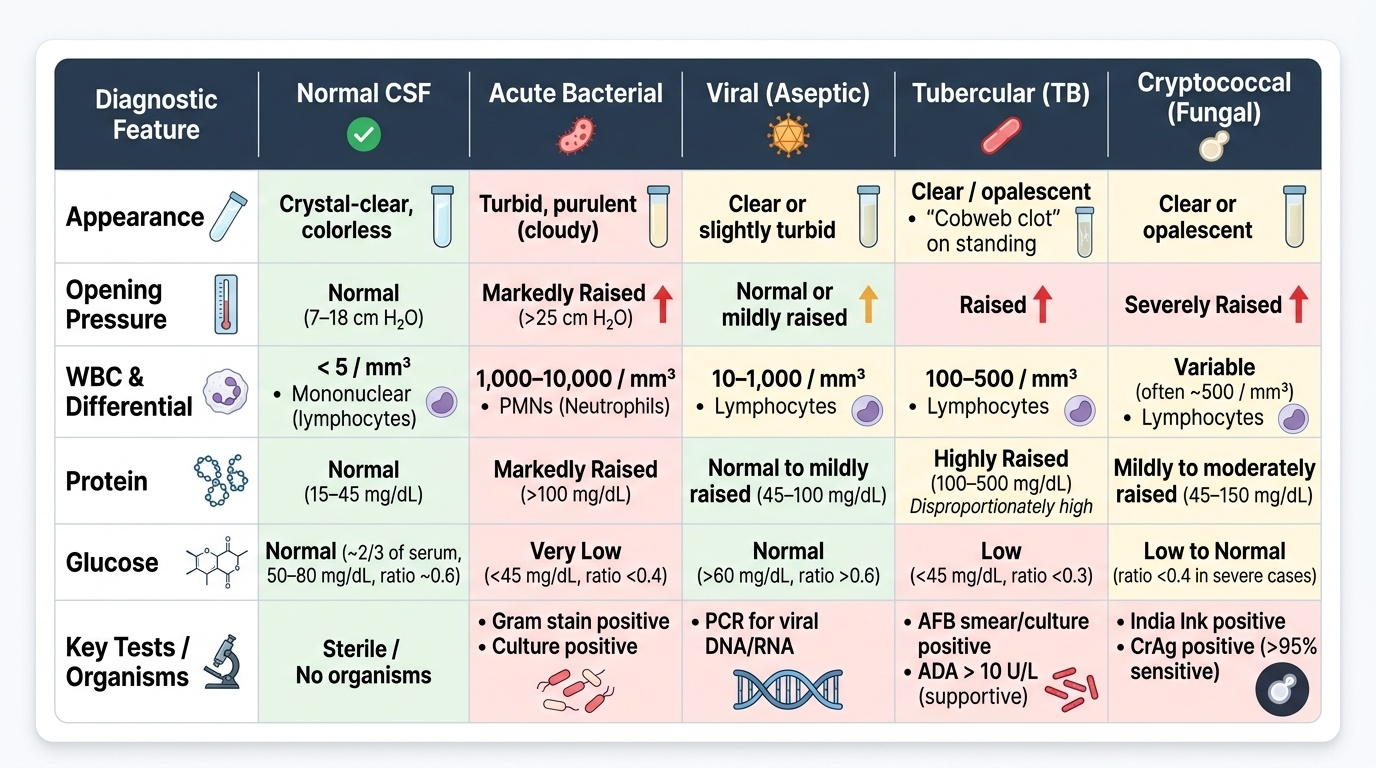
Normal CSF: Crystal-clear, colourless, WBC <5 (all mononuclear lymphocytes), protein 15–45 mg/dL, glucose 2/3 of serum (50–80 mg/dL, ratio >0.6), no organisms, no xanthochromia.
Xanthochromia (yellow discolouration): due to oxyhaemoglobin (pink, 2–4 hours post-SAH) → bilirubin (yellow, 12 hours–2 weeks). Differentiates subarachnoid haemorrhage from traumatic tap (traumatic tap: no xanthochromia, clears as tubes collected sequentially).
| Feature | Bacterial | Viral (aseptic) | Tubercular (TB) | Fungal (Cryptococcus) |
|---|---|---|---|---|
| Appearance | Turbid, purulent | Clear/slightly turbid | Clear or opalescent, cobweb clot | Clear or opalescent |
| Pressure | Raised | Normal/mildly raised | Raised | Raised |
| WBC count | 1,000–10,000/mm³ | 10–1,000/mm³ | 100–500/mm³ | Variable, often <500 |
| Cell type | PMN (neutrophils) | Mononuclear (lymphocytes) | Mononuclear (lymphocytes) | Mononuclear (lymphocytes) |
| Protein | Markedly raised (>100 mg/dL) | Normal to mildly raised (45–100 mg/dL) | Raised (100–500 mg/dL) | Mildly–moderately raised |
| Glucose | Very low (<45 mg/dL, ratio <0.4) | Normal (>60 mg/dL) | Low (<45 mg/dL) | Low to normal |
| Organisms/tests | Gram stain + culture positive | PCR for virus | AFB smear/culture/ADA elevated | India ink +; latex agglutination (CrAg) + |
Key differentiating points:
• PMNs in CSF → bacterial until proven otherwise. A viral meningitis can begin with PMNs but shifts to lymphocytes within 24–48 hours.
• TB meningitis: protein is disproportionately high, glucose disproportionately low; a cobweb clot on standing is characteristic; ADA >10 U/L is supportive.
• Cryptococcal meningitis (immunocompromised — HIV CD4 <100): India ink shows the encapsulated yeast ('halo' appearance); latex agglutination for cryptococcal antigen (CrAg) is 95%+ sensitive.
• Glucose interpretation: always use CSF:serum ratio; in hyperglycaemia, CSF glucose may appear 'normal' but the ratio is still low.
SELF-CHECK
A 22-year-old HIV-positive patient (CD4 count 60 cells/μL) presents with 2 weeks of headache and low-grade fever. CSF: clear, WBC 80/mm³ (lymphocytes), protein 95 mg/dL, glucose 35 mg/dL (serum glucose 90 mg/dL). India ink preparation shows encapsulated yeast. Which organism is responsible?
A. Mycobacterium tuberculosis
B. Neisseria meningitidis
C. Cryptococcus neoformans
D. Listeria monocytogenes
Reveal Answer
Answer: C. Cryptococcus neoformans
This is textbook Cryptococcal meningitis: HIV-positive with very low CD4 (<100), subacute onset (2 weeks), lymphocytic pleocytosis, elevated protein, low CSF glucose — and India ink showing encapsulated yeast with a clear halo (the large polysaccharide capsule). M. tuberculosis would not show yeast on India ink. N. meningitidis causes acute purulent meningitis with PMNs. Listeria occurs in elderly/immunocompromised with PMNs.
Synovial Fluid Analysis
Synovial Fluid Analysis
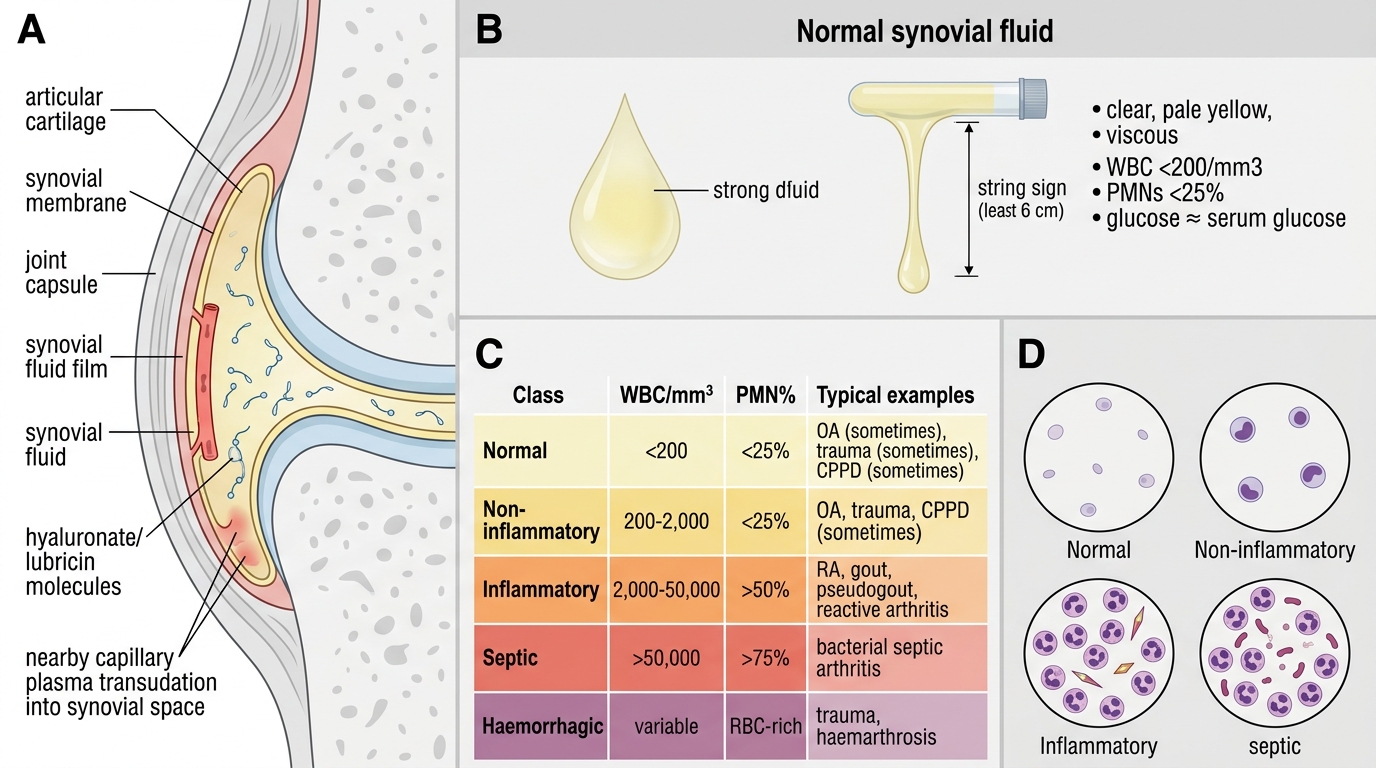
Synovial fluid (SF) is a transudate of plasma plus lubricin/hyaluronate secreted by synoviocytes. Normal SF: clear, pale yellow, viscous (string sign ≥6 cm), WBC <200/mm³ (<25% PMNs), glucose ≈ serum glucose.
SF is classified by its gross and microscopic appearance:
| Class | WBC/mm³ | PMN% | Example |
|---|---|---|---|
| Normal | <200 | <25% | — |
| Non-inflammatory | 200–2,000 | <25% | OA, trauma, CPPD (sometimes) |
| Inflammatory | 2,000–50,000 | >50% | RA, gout, pseudogout, reactive arthritis |
| Septic (infectious) | >50,000 | >75% | Septic arthritis (bacterial) |
| Haemorrhagic | RBCs present | — | Trauma, haemophilia, pigmented villonodular synovitis |
Crystal analysis (compensated polarised light microscopy):
- Monosodium urate (MSU) — gout:
- Shape: long needles (may be intracellular in WBCs)
- Birefringence: negatively birefringent → yellow when parallel to the slow axis, blue when perpendicular
- Appearance: 'matchstick' or needle, sharp ends
- Calcium pyrophosphate dihydrate (CPPD) — pseudogout:
- Shape: rhomboid/short rod, often intra- or extracellular
- Birefringence: positively birefringent → blue when parallel, yellow when perpendicular
- X-ray: chondrocalcinosis (calcification of articular cartilage)
Septic arthritis: The most important emergency — joint fluid WBC >50,000 with >75% PMNs and positive Gram stain/culture warrants immediate joint drainage and IV antibiotics. Never miss it; glucocorticoid injection into an infected joint is catastrophic.
Mucin clot test: Acetic acid added to SF — good clot (rope-like) = normal/non-inflammatory; poor/friable clot = inflammatory/septic.
SELF-CHECK
Polarised light microscopy of synovial fluid aspirated from a painful, swollen first MTP joint shows needle-shaped crystals that appear YELLOW when oriented parallel to the slow axis of the red compensator. What is the correct interpretation?
A. Calcium pyrophosphate dihydrate crystals — pseudogout
B. Monosodium urate crystals — gout; negatively birefringent
C. Calcium oxalate crystals — oxalate arthropathy
D. Cholesterol crystals from lipid effusion
Reveal Answer
Answer: B. Monosodium urate crystals — gout; negatively birefringent
Yellow when PARALLEL = negatively birefringent = monosodium urate (MSU) = gout. The mnemonic: 'gout is Yellow when Parallel' (YP). CPPD is positively birefringent — blue when parallel. The first MTP joint (podagra) is the classic gout joint. Confirm with serum uric acid and clinical history. CPPD typically affects larger joints — knee (chondrocalcinosis on X-ray), wrist.