Page 14 of 28
PA23.8 | Colorectal Carcinoma — SDL Guide
Learning Objectives
- List the major risk factors for colorectal carcinoma including dietary, inflammatory and hereditary factors
- Describe the precursor lesions — adenomatous polyps (tubular, tubulovillous, villous) — and explain the adenoma-carcinoma sequence
- Outline the polyposis syndromes FAP/APC and HNPCC/Lynch syndrome with their molecular basis
- Distinguish the APC/β-catenin (chromosomal instability) pathway from the MMR/microsatellite instability pathway
- Contrast the gross and clinical features of right-sided vs left-sided colorectal carcinoma
- Identify the histological subtypes — conventional adenocarcinoma, mucinous and signet-ring — and interpret tumour grading
- Apply Dukes and TNM staging systems and correlate stage with prognosis
- Describe routes of spread and the role of CEA as a tumour marker in monitoring
INSTRUCTIONS
Colorectal carcinoma is the third most common cancer worldwide and a model example of stepwise molecular carcinogenesis — from normal epithelium through precursor polyps to invasive malignancy. Understanding this disease is essential for clinico-pathological correlation because presentation, prognosis and surgical management differ strikingly depending on which side of the colon is involved. This module also introduces the two major molecular pathways driving colorectal cancer, which underpin hereditary syndromes you will encounter in clinical practice.
References
- Robbins & Kumar — Basic Pathology, 11th ed., Ch 17 (Gastrointestinal Tract) (textbook)
- Harsh Mohan — Textbook of Pathology, 8th ed., Ch 20 (textbook)
- WHO Classification of Tumours — Digestive System, 5th ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 68-year-old retired schoolteacher comes to you with a six-month history of fatigue and is found to have a haemoglobin of 7.2 g/dL with a microcytic picture — yet she has had no visible blood in the stool. Her faecal occult blood test is positive. Meanwhile, her 52-year-old son presents to the surgical OPD with a two-month history of colicky left iliac fossa pain, pencil-thin stools and a sense of incomplete evacuation. Same disease; completely different presentations. By the end of this module you will understand exactly why — and why the difference matters for survival.
WHY THIS MATTERS
Colorectal carcinoma kills more patients worldwide than almost any other GI malignancy, yet it is one of the most preventable cancers through screening. As a clinician you will use your understanding of the adenoma-carcinoma sequence to counsel patients on colonoscopic surveillance, recognise the phenotypes of hereditary polyposis syndromes in family histories, interpret staging at multidisciplinary tumour boards, and monitor disease with CEA after resection. The molecular pathways you learn here reappear in targeted therapy decisions and in explaining why some colorectal cancers respond to immunotherapy.
RECALL
Before starting, spend two minutes recalling:
- What is a polyp? How does a sessile polyp differ from a pedunculated one?
- What genes drive the G1/S cell-cycle checkpoint, and what happens when they are lost?
- What is microsatellite instability, and which repair system prevents it?
- Trace the portal venous drainage of the colon — where does haematogenous spread from the colon first lodge?
If any of these feel shaky, quickly review cell-cycle regulation (Biochemistry/Pathology Year-1) and portal venous anatomy (Anatomy Year-1) before proceeding.
Epidemiology and Risk Factors
Epidemiology and Risk Factors of Colorectal Carcinoma
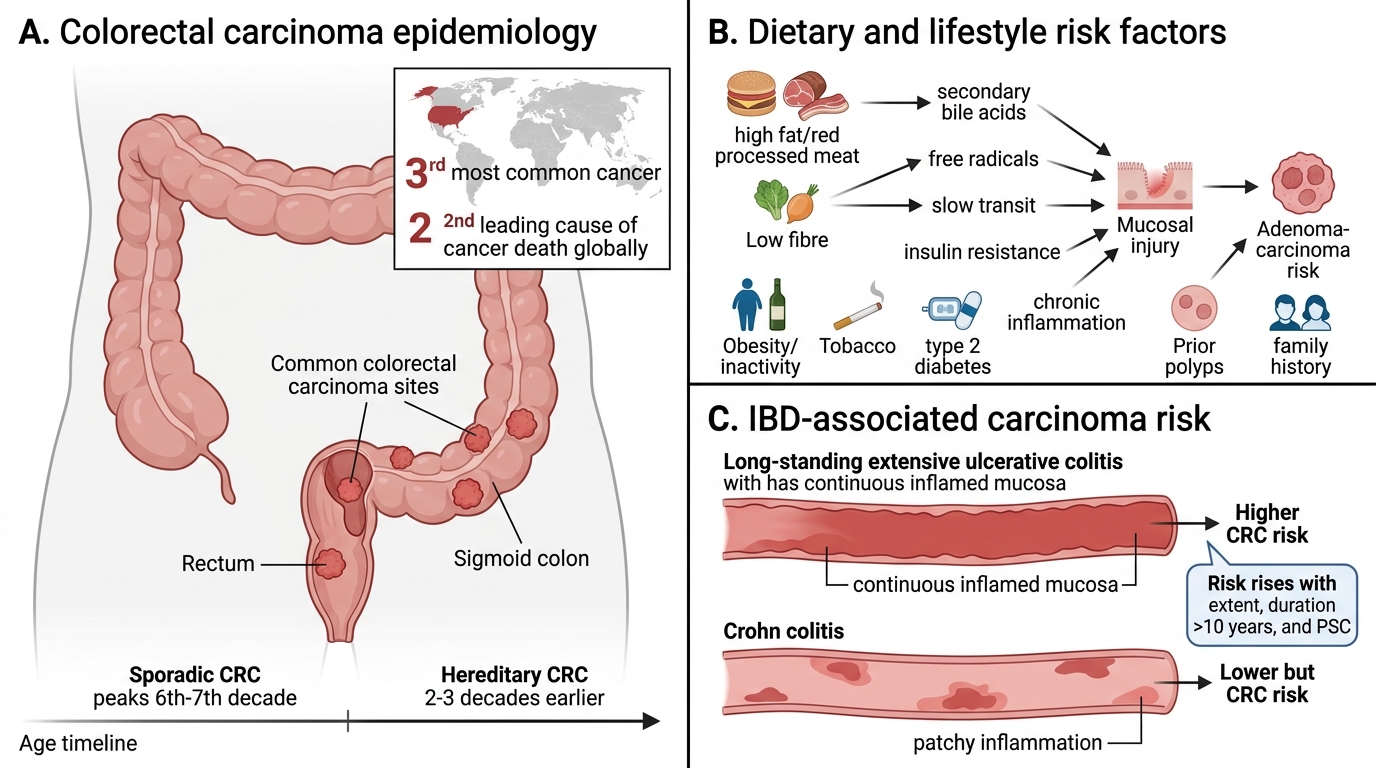
Colorectal carcinoma (CRC) is the third most common cancer and the second leading cause of cancer death globally. Incidence peaks in the sixth to seventh decade, though hereditary forms present two to three decades earlier.
Dietary and lifestyle risk factors:
- High fat, high red/processed meat intake — promotes secondary bile acid production and free-radical mucosal injury.
- Low dietary fibre — reduces stool transit time, increasing mucosal exposure to carcinogens.
- Obesity and physical inactivity — linked via insulin resistance and chronic low-grade inflammation.
- Alcohol and tobacco independently increase risk.
Inflammatory bowel disease: Ulcerative colitis (UC) confers the highest CRC risk among inflammatory conditions (colitis-associated carcinoma), rising dramatically with extent of disease, duration (>10 years) and co-existing primary sclerosing cholangitis. Crohn's colitis carries a lower but still elevated risk.
Other risk factors: previous colorectal polyps or CRC, family history, type-2 diabetes.
Note that approximately 75% of CRCs are sporadic (no hereditary syndrome); 25% show familial clustering.
SELF-CHECK
A 55-year-old man with a 20-year history of extensive ulcerative colitis presents with a new mass in the sigmoid colon. Which ONE of the following factors in his history MOST directly increases his colorectal carcinoma risk above that of the general population?
A. Long-standing extensive UC with chronic mucosal inflammation
B. Low dietary fibre intake
C. High red meat consumption
D. Obesity (BMI 31 kg/m²)
Reveal Answer
Answer: A. Long-standing extensive UC with chronic mucosal inflammation
Long-standing extensive ulcerative colitis (≥10 years, pancolitis) is the single greatest individual risk factor in this scenario, conferring a cumulative CRC risk of ~2% at 10 years, 8% at 20 years, and up to 18% at 30 years — far exceeding the contribution of diet or obesity alone. Chronic mucosal inflammation drives colitis-associated carcinoma through oxidative DNA damage, epigenetic silencing, and field-effect dysplasia, often progressing without a distinct adenoma precursor.
Precursor Lesions — Adenomatous Polyps
Adenomatous Polyps: Classification and Malignant Risk
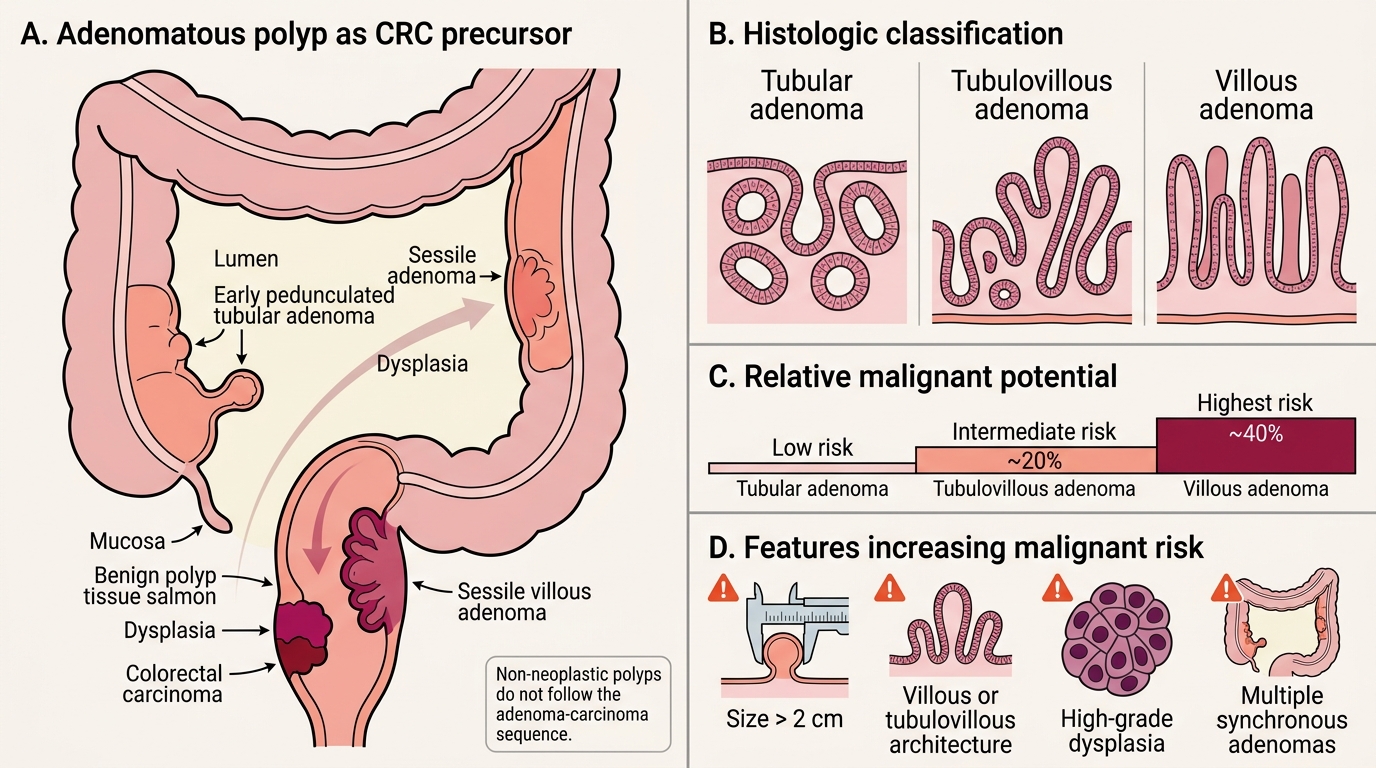
The vast majority of sporadic CRCs arise from adenomatous polyps (adenomas) — benign glandular neoplasms that carry genuine malignant potential. Understanding their classification is fundamental.
Classification by histology:
| Type | Architecture | Malignant Potential |
|---|---|---|
| Tubular adenoma | ≥80% tubular glands | Low (~5%) |
| Tubulovillous adenoma | Mixed tubular + villous (25–75% villous) | Intermediate (~20%) |
| Villous adenoma | ≥80% villous fronds | Highest (~40%) |
Villous adenomas are typically sessile, large, and most commonly found in the rectum. Their finger-like villous projections maximise surface area and dysplasia depth.
Features increasing malignant risk in any adenoma:
- Size >2 cm
- Villous or tubulovillous architecture
- High-grade dysplasia
- Multiple adenomas (synchronous polyps)
Non-neoplastic polyps (hyperplastic, juvenile, hamartomatous) do not follow the adenoma-carcinoma sequence — a distinction critical for correct management.
The Adenoma-Carcinoma Sequence
Adenoma-Carcinoma Sequence in Colorectal Cancer
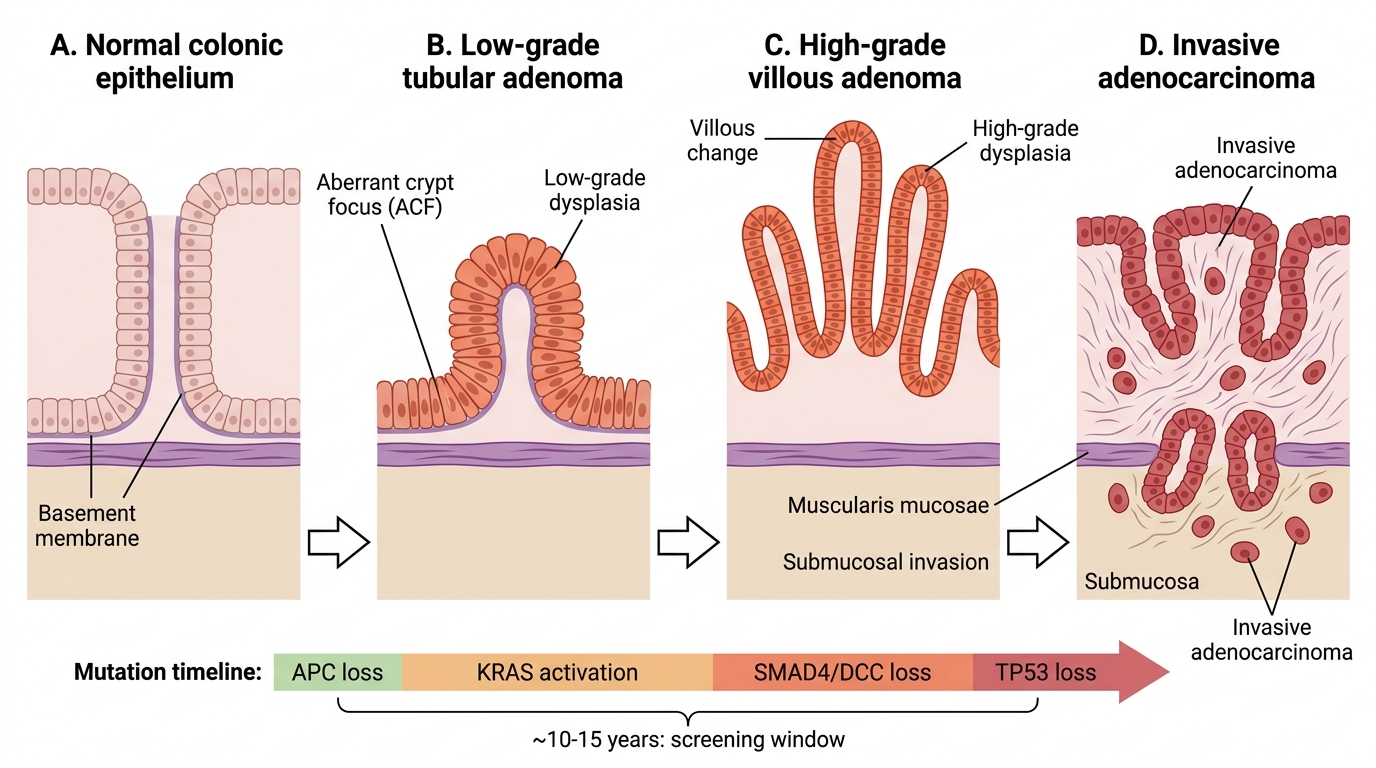
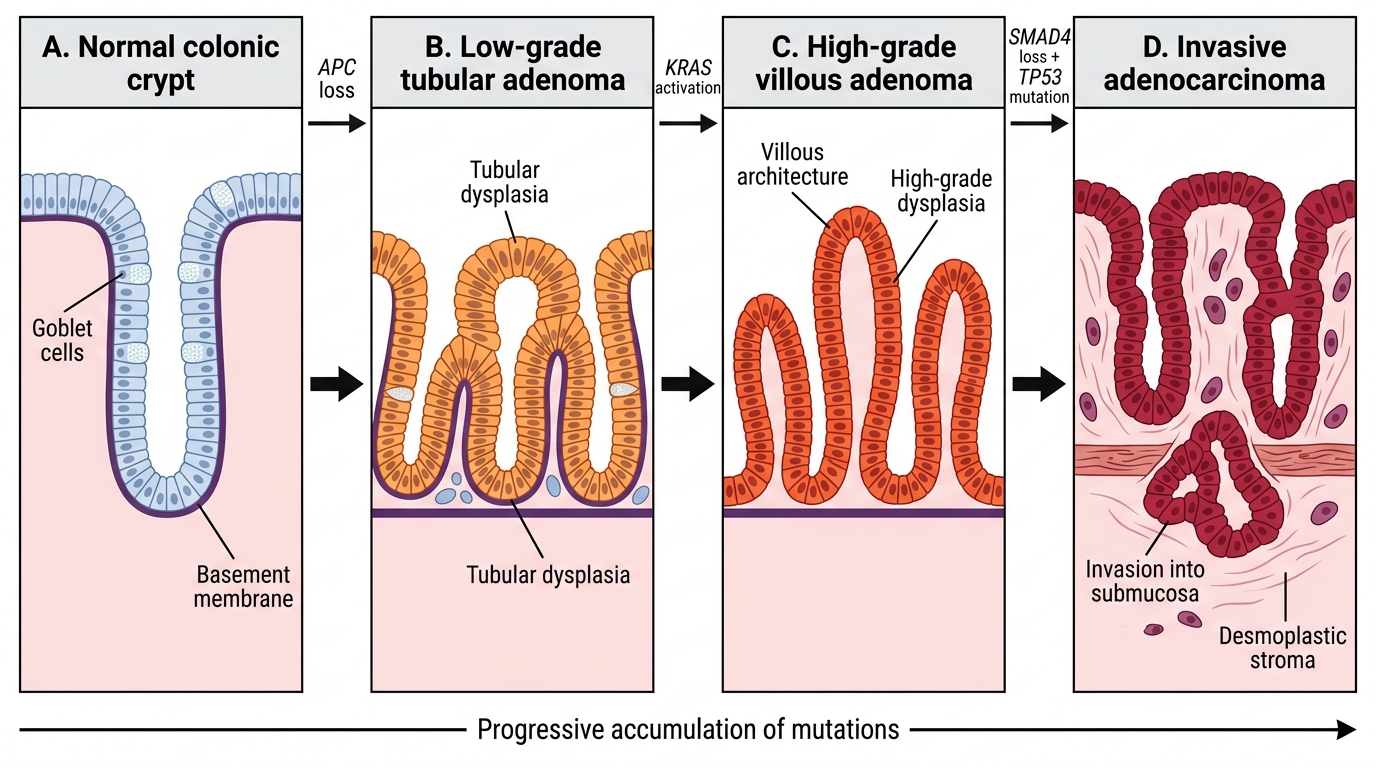
The adenoma-carcinoma sequence is the stepwise molecular and morphological progression from normal colonic epithelium → low-grade adenoma → high-grade adenoma → invasive adenocarcinoma. This is the Vogelstein model, supported by decades of epidemiological and molecular evidence.
Morphological steps:
1. Normal mucosa → focal epithelial proliferation (ACF — aberrant crypt foci)
2. Small tubular adenoma (low-grade dysplasia)
3. Enlarging adenoma with increasing villous change and high-grade dysplasia
4. Carcinoma in situ → invasive adenocarcinoma (once the muscularis mucosae is breached)
Time frame: ~10–15 years from first adenoma to invasive carcinoma — the biological window that makes screening effective.
IMPORTANT: The adenoma must acquire sequential mutations (not all at once). Loss of APC is the initiating step in the chromosomal instability pathway; subsequent mutations in KRAS, SMAD4/DCC, and finally TP53 drive progression.
Adenoma-Carcinoma Sequence in Colorectal Cancer