Page 15 of 28
PA23.8 | Colorectal Carcinoma — SDL Guide (Part 2)
Polyposis Syndromes — FAP and HNPCC/Lynch
Hereditary Colorectal Cancer Syndromes: FAP vs Lynch
Two major hereditary syndromes account for most familial CRC:
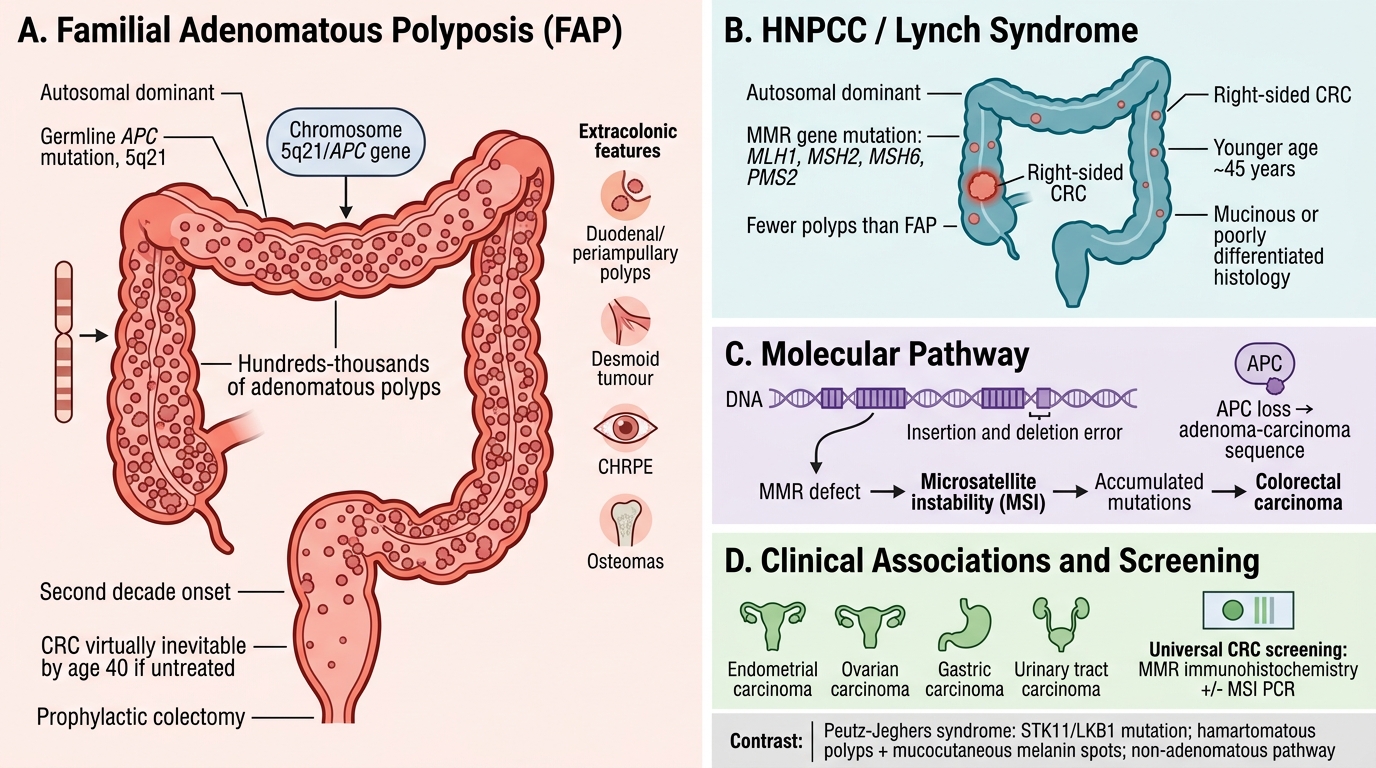
1. Familial Adenomatous Polyposis (FAP)
- Inheritance: Autosomal dominant; germline APC mutation (chromosome 5q21).
- Phenotype: Hundreds to thousands of colorectal adenomatous polyps, typically appearing in the second decade; if untreated, CRC is virtually inevitable by age 40.
- Extracolonic: Duodenal/periampullary polyps, desmoid tumours (Gardner syndrome variant), congenital hypertrophy of retinal pigment epithelium (CHRPE), osteomas.
- Management: Prophylactic colectomy.
2. Hereditary Non-Polyposis Colorectal Cancer (HNPCC) / Lynch Syndrome
- Inheritance: Autosomal dominant; germline mutations in mismatch repair (MMR) genes — most commonly MLH1, MSH2, MSH6, PMS2.
- Molecular consequence: Microsatellite instability (MSI) — repetitive DNA sequences (microsatellites) accumulate insertion/deletion errors.
- Phenotype: Fewer polyps than FAP; CRC often right-sided, arising at younger age (~45 years); mucinous or poorly differentiated histology.
- Extracolonic: Endometrial, ovarian, gastric, urinary tract carcinomas (Amsterdam II criteria).
- Screening: MMR immunohistochemistry ± MSI PCR on all CRC tissue (universal screening).
Peutz-Jeghers syndrome (STK11/LKB1 mutation) causes hamartomatous polyps + mucocutaneous melanin spots; CRC risk elevated but pathway is non-adenomatous.
SELF-CHECK
A 44-year-old woman is found to have a right-sided colon carcinoma. Immunohistochemistry shows absent MLH1 and PMS2 protein expression. Which molecular pathway is most likely driving this tumour?
A. APC/β-catenin chromosomal instability pathway
B. Mismatch repair deficiency with microsatellite instability
C. RAS/RAF serrated pathway
D. TP53 loss with aneuploidy
Reveal Answer
Answer: B. Mismatch repair deficiency with microsatellite instability
Loss of MLH1 and PMS2 by IHC indicates mismatch repair (MMR) deficiency. Absent MMR protein leads to microsatellite instability (MSI-H). This is the hallmark of the Lynch syndrome/HNPCC pathway, and MSI-H CRCs characteristically arise on the right side of the colon, at a younger age, and show mucinous or poorly differentiated histology. MSI-H CRCs also respond to PD-1/PD-L1 immune checkpoint inhibitors.
Molecular Pathways — CIN vs MSI
Molecular Pathways in Colorectal Carcinogenesis: CIN vs MSI
Two principal molecular mechanisms drive colorectal carcinogenesis:
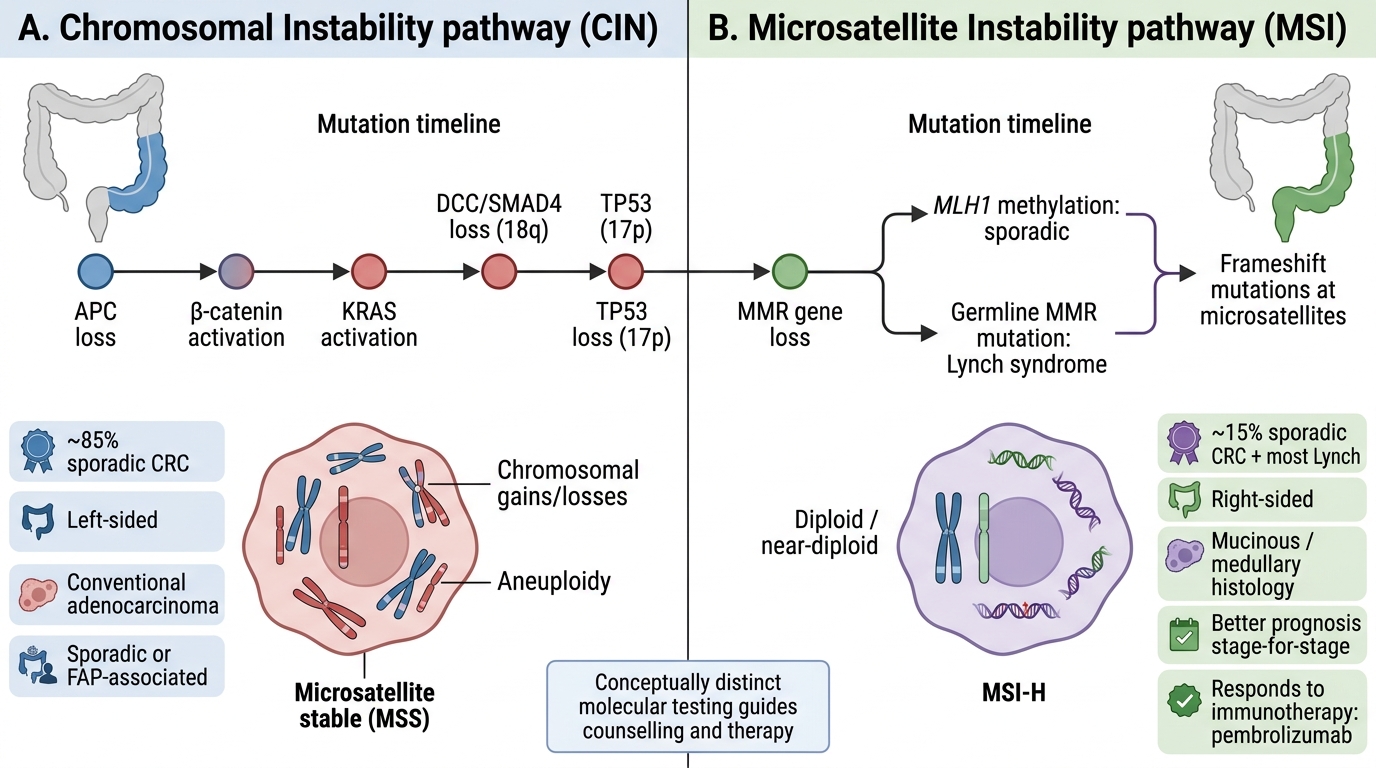
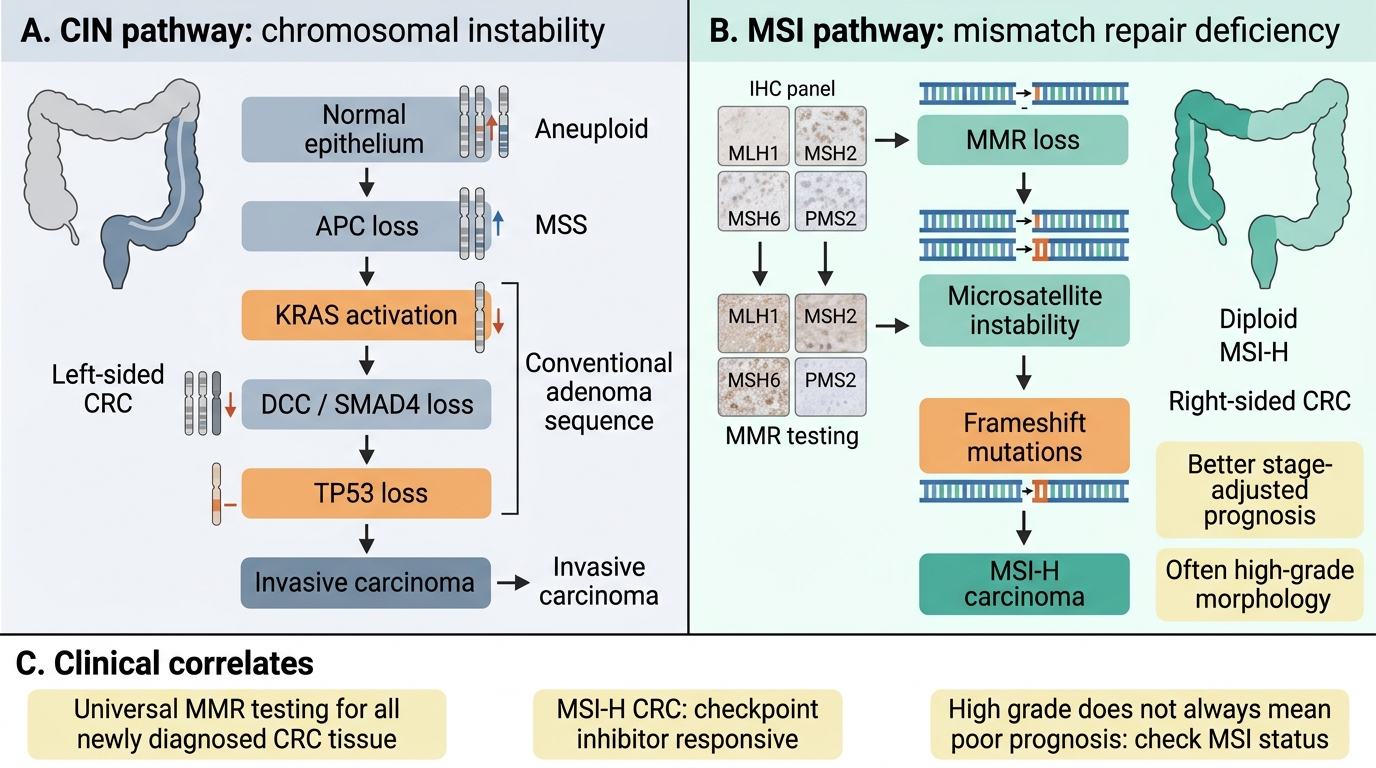
Pathway 1 — Chromosomal Instability (CIN): APC/β-catenin
- Accounts for ~85% of sporadic CRC.
- Initiating event: loss of APC tumour suppressor → unrestrained β-catenin transcription → increased cell proliferation.
- Sequential mutations: APC → activating KRAS → loss of SMAD4/DCC (18q) → loss of TP53 (17p).
- Result: widespread chromosomal gains and losses (aneuploidy), microsatellite stable (MSS).
- Clinically: left-sided predominance, conventional adenocarcinoma, sporadic or FAP-associated.
Pathway 2 — Microsatellite Instability (MSI): MMR deficiency
- Accounts for ~15% of sporadic CRC + most Lynch syndrome.
- Initiating event: loss of MMR genes (MLH1 silenced by methylation in sporadic cases; germline mutation in Lynch).
- Result: frameshift mutations accumulate at microsatellites throughout genome; diploid or near-diploid tumours.
- Clinically: right-sided predominance, mucinous/medullary histology, better prognosis stage-for-stage, respond to immunotherapy (MSI-H = predictive biomarker for pembrolizumab).
IMPORTANT: These pathways are not mutually exclusive but are conceptually distinct; knowing which pathway is active guides molecular testing, hereditary counselling and therapy selection.
CIN versus MSI Pathways in Colorectal Carcinoma
CLINICAL PEARL
Universal MMR testing is now recommended for all newly diagnosed CRC tissue. This single IHC panel (MLH1, MSH2, MSH6, PMS2) identifies Lynch syndrome candidates, guides immunotherapy eligibility (MSI-H CRCs respond dramatically to checkpoint inhibitors), and provides prognostic information. A tumour that is MSI-H has better stage-adjusted survival — but paradoxically tends to be higher grade on morphology. Never assume high grade = poor prognosis without knowing MSI status.
Gross Pathology — Right-Sided vs Left-Sided CRC
Gross Pathology of Right-Sided vs Left-Sided Colorectal Carcinoma
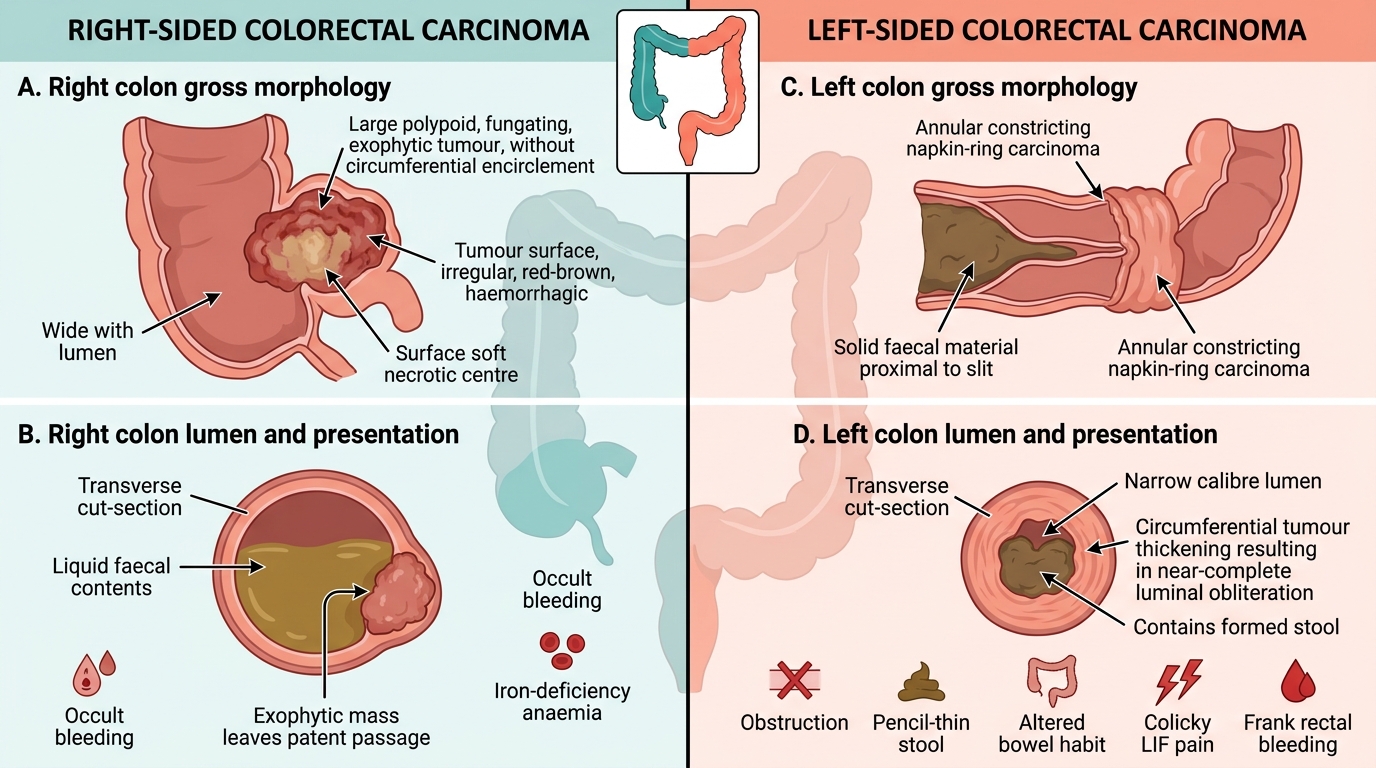
The anatomical side of the colon profoundly influences gross morphology and clinical presentation, because luminal calibre and faecal consistency differ markedly between caecum/ascending colon and descending/sigmoid colon.
Right-sided CRC (caecum, ascending colon)
- Gross form: Polypoid / fungating / exophytic mass — grows into the wide lumen without encircling it.
- Lumen: Wide; liquid faeces → obstruction is late and uncommon.
- Clinical presentation: Occult gastrointestinal bleeding → iron-deficiency anaemia, fatigue, palpable RIF mass. No visible rectal bleeding, no obstruction.
- Cut surface: Soft, haemorrhagic tumour tissue; necrotic centre common.
Left-sided CRC (descending colon, sigmoid, rectum)
- Gross form: Annular / constricting / "napkin-ring" lesion — encircles the narrow lumen circumferentially.
- Lumen: Narrow; solid/formed faeces → obstruction is early and common.
- Clinical presentation: Colicky LIF pain, altered bowel habit (constipation alternating with diarrhoea), pencil-thin stools, rectal bleeding (frank).
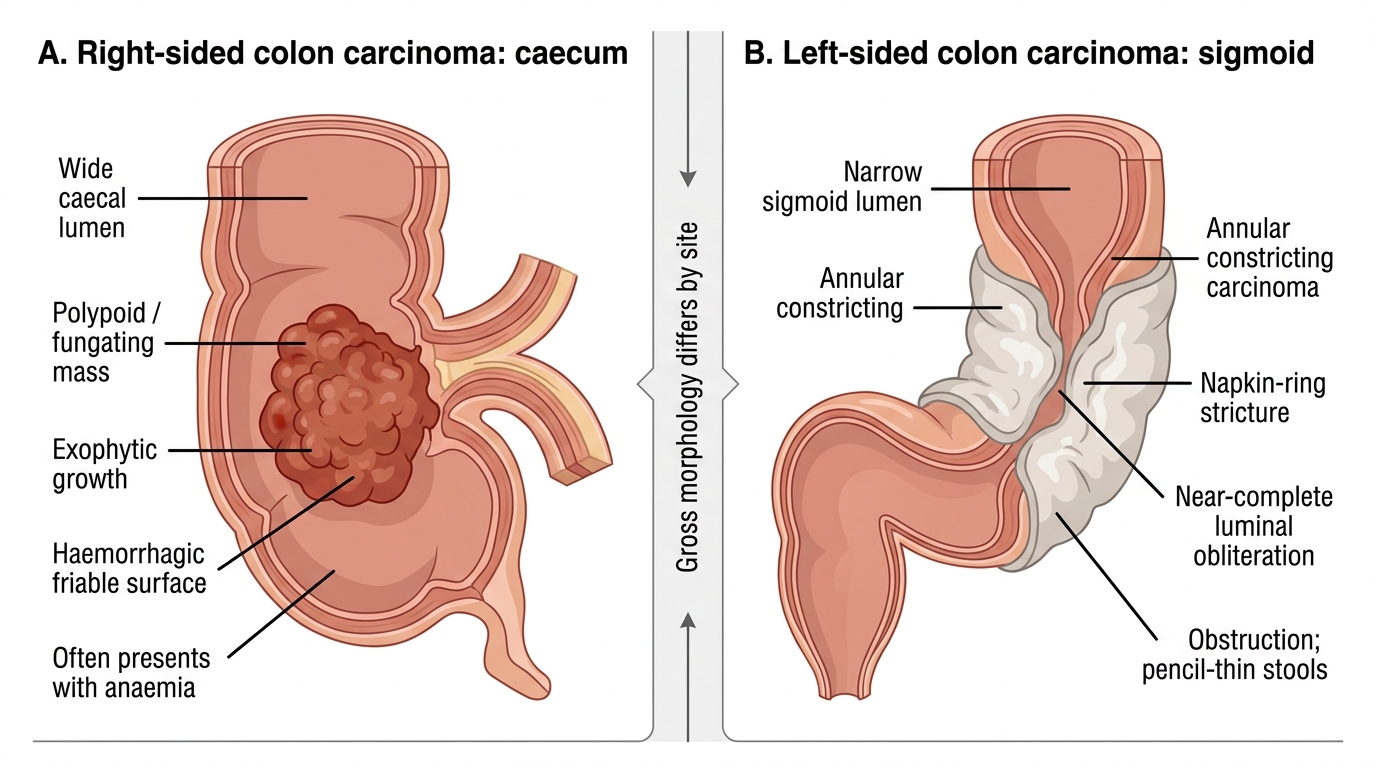
Gross Morphology of Right- versus Left-Sided Colorectal Carcinoma
SELF-CHECK
A 70-year-old man presents with progressive obstruction and pencil-thin stools. Colonoscopy reveals a circumferential annular lesion at the sigmoid colon. Which gross morphological pattern does this represent?
A. Polypoid / fungating / exophytic
B. Annular / constricting / napkin-ring
C. Ulcerating with raised edges
D. Diffuse infiltrating (linitis plastica pattern)
Reveal Answer
Answer: B. Annular / constricting / napkin-ring
The sigmoid colon has a narrow lumen and carries formed stool — carcinomas here encircle the wall circumferentially, producing the classic annular 'napkin-ring' stricture that causes obstruction and alters stool calibre. The polypoid/fungating pattern is characteristic of right-sided (caecum/ascending) CRC, which presents with anaemia rather than obstruction. Linitis plastica is a diffuse gastric pattern, not typical of the colon.