Page 16 of 28
PA23.8 | Colorectal Carcinoma — SDL Guide (Part 3)
Histopathology — Microscopic Features and Grading
Colorectal Adenocarcinoma: Microscopic Features and Grading
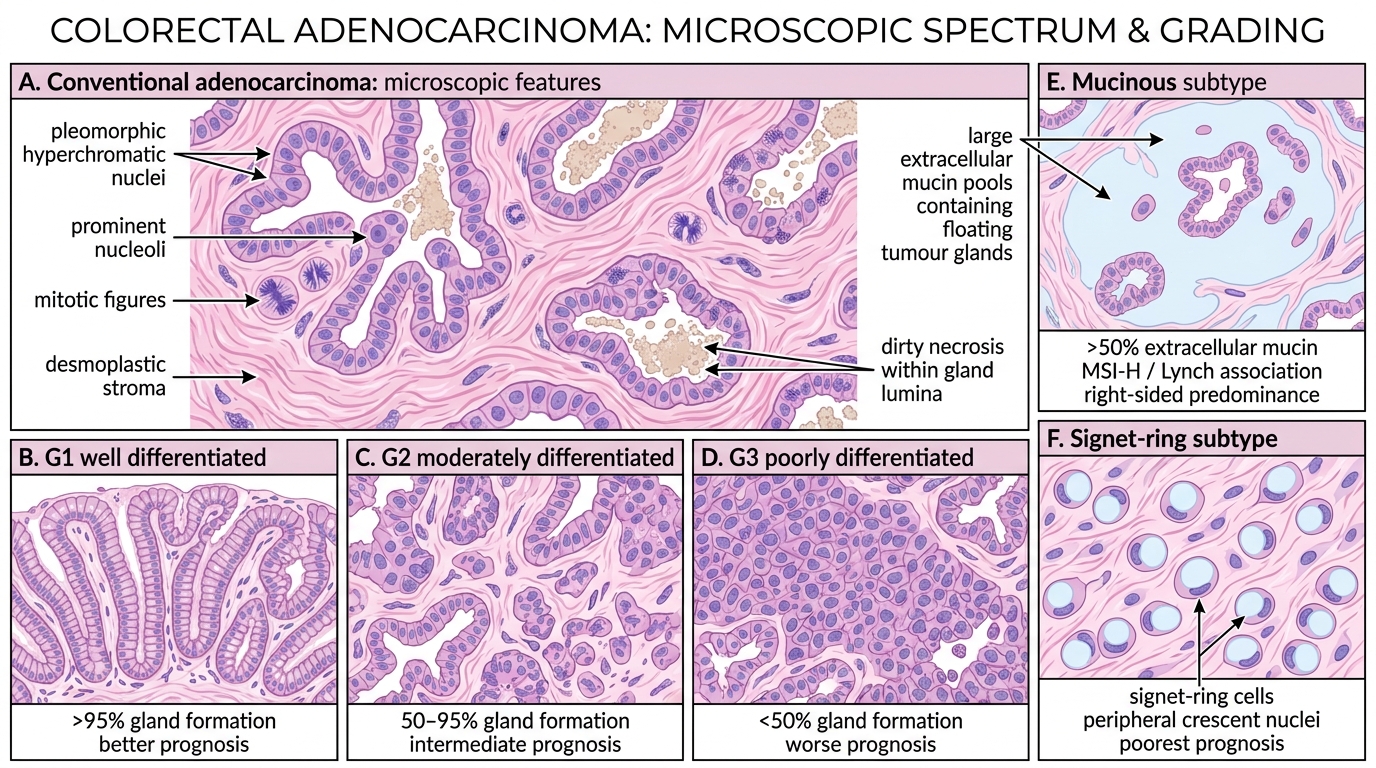
Conventional adenocarcinoma (most common)
- Gland-forming tumour cells with nuclear pleomorphism, prominent nucleoli, and mitotic activity.
- "Dirty necrosis" — a distinctive feature: necrotic cellular debris within the tumour gland lumina (intraluminal necrosis), producing a characteristic dirty appearance on H&E. This helps distinguish colorectal from other gland-forming metastases.
- Desmoplastic stroma surrounds the glands.
Grading (WHO):
| Grade | Gland formation | Behaviour |
|---|---|---|
| Well-differentiated (G1) | >95% glandular | Better prognosis |
| Moderately differentiated (G2) | 50–95% glandular | Intermediate |
| Poorly differentiated (G3) | <50% glandular | Worse prognosis |
Special subtypes:
- Mucinous adenocarcinoma (>50% extracellular mucin pools): associated with MSI-H/Lynch; right-sided predominance; classified G3 by default.
- Signet-ring cell carcinoma (<10% of CRC): single cells with intracytoplasmic mucin displacing the nucleus to periphery; poorest prognosis; associated with Lynch syndrome.
Tumour budding (isolated single cells or clusters of <5 cells at the invasive front) is an independent adverse prognostic feature now reported routinely.
Spread and Routes of Metastasis
Routes of Metastasis in Colorectal Carcinoma
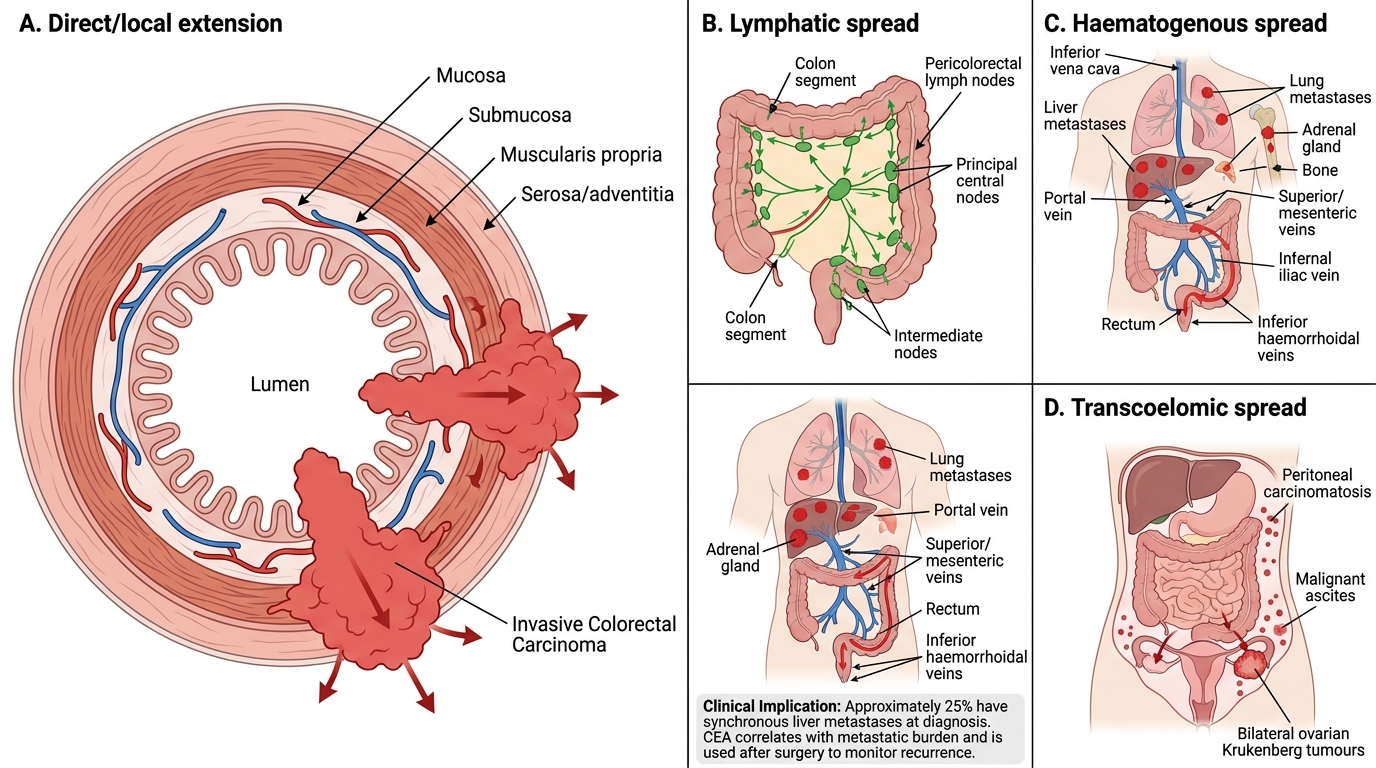
CRC spreads by four classical routes:
- Direct/local extension: Through the bowel wall layers (mucosa → submucosa → muscularis propria → pericolorectal fat → adjacent organs). Determines the T-stage.
- Lymphatic spread: To pericolorectal lymph nodes → intermediate nodes → principal (central) nodes. Number of involved nodes is a major prognostic determinant (N-stage).
- Haematogenous spread: Via the portal vein → liver (most common distant metastatic site). Subsequently, pulmonary, adrenal and osseous metastases. Rectal carcinoma may also spread via the inferior haemorrhoidal veins to the systemic circulation, bypassing the liver (direct lung metastases).
- Transcoelomic (peritoneal) spread: Seeding of the peritoneal cavity → peritoneal carcinomatosis; malignant ascites; Krukenberg tumour (bilateral ovarian metastases from mucin-secreting CRC).
Clinical implication: At time of diagnosis, ~25% of patients have synchronous liver metastases. CEA level correlates with metastatic burden and is used post-operatively to monitor for recurrence.
Staging — Dukes and TNM
Colorectal Carcinoma Staging: Dukes and TNM
Two staging systems are used in parallel — you must know both.
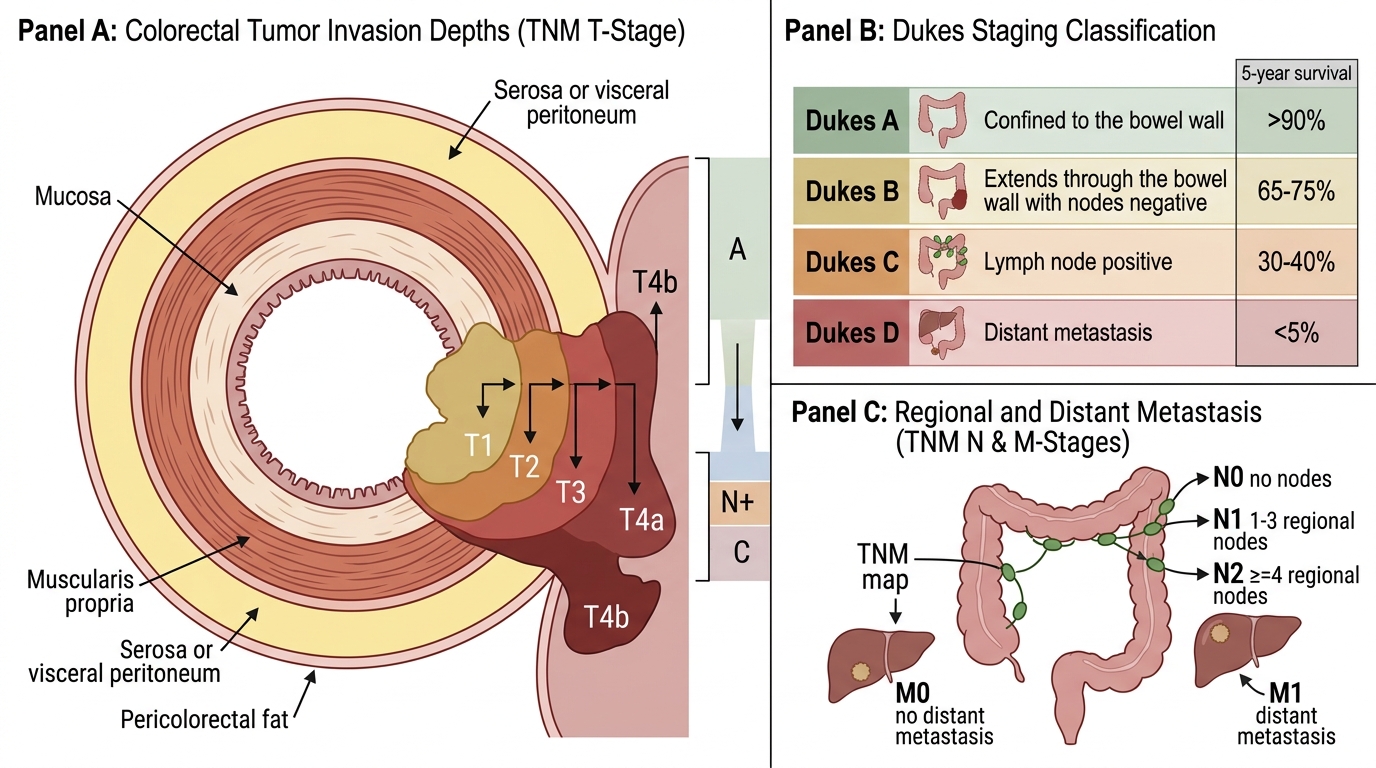
Dukes Staging (original + modified Astler-Coller):
| Stage | Extent | 5-Year Survival |
|---|---|---|
| Dukes A | Confined to bowel wall (not beyond muscularis propria) | >90% |
| Dukes B | Through bowel wall into pericolorectal fat; nodes negative | 65–75% |
| Dukes C | Any wall depth; lymph node positive | 30–40% |
| Dukes D | Distant metastases (added by later modifications) | <5% |
TNM Staging (AJCC/UICC):
- T (Tumour): T1 = submucosa; T2 = muscularis propria; T3 = pericolorectal tissues; T4a = visceral peritoneum; T4b = adjacent organs.
- N (Nodes): N0 = none; N1 = 1–3 regional nodes; N2 = ≥4 regional nodes.
- M (Metastasis): M0 = none; M1 = distant.
- Stages I–IV roughly correspond to Dukes A, B, C, D.
Key prognostic factors beyond stage: grade, margin status (R0/R1), vascular invasion, perineural invasion, tumour budding, MSI status.
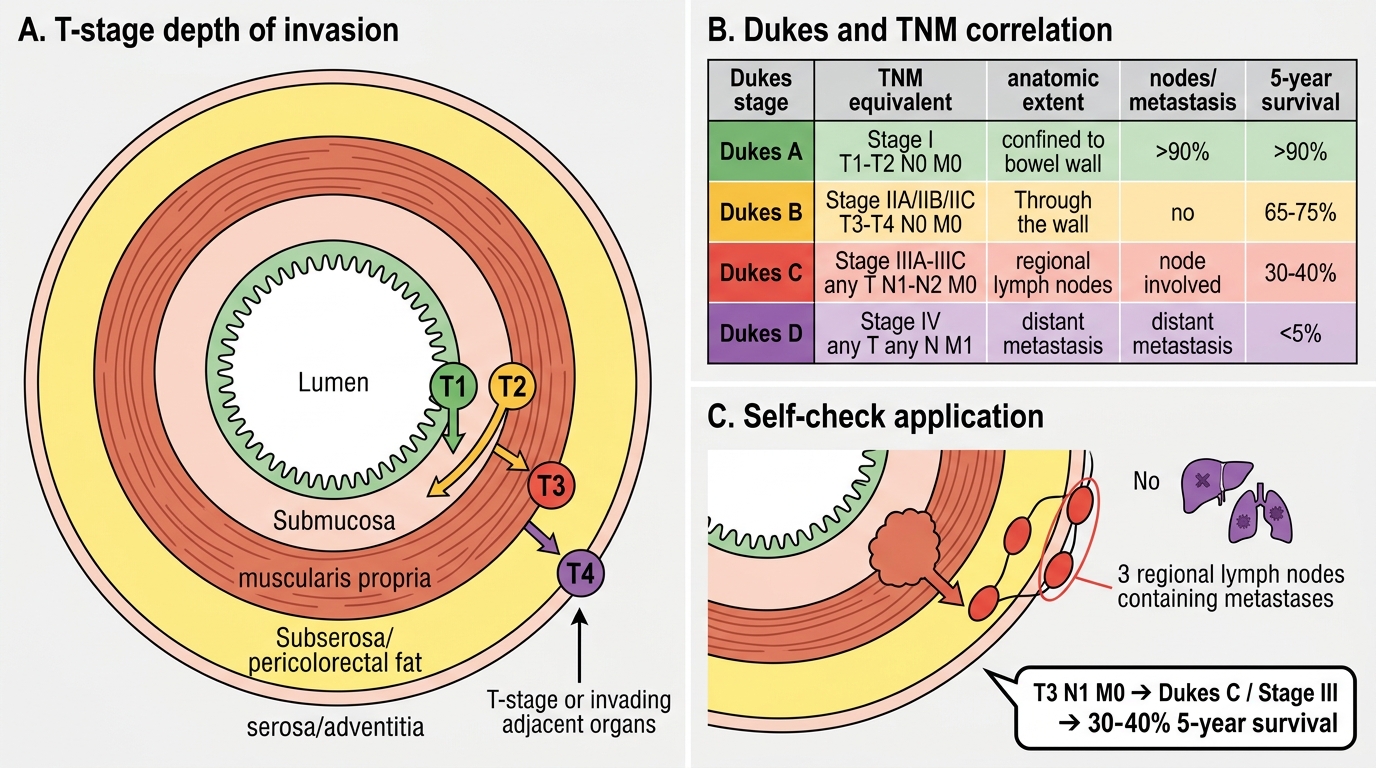
Colorectal Carcinoma: Dukes and TNM Staging
SELF-CHECK
A resected colorectal carcinoma invades through the muscularis propria into pericolorectal fat. Three of twelve harvested lymph nodes contain metastatic carcinoma. No distant metastasis. What is the Dukes stage and approximate 5-year survival?
A. Dukes A; >90% survival
B. Dukes B; 65–75% survival
C. Dukes C; 30–40% survival
D. Dukes D; <5% survival
Reveal Answer
Answer: C. Dukes C; 30–40% survival
Lymph node involvement at any depth of wall invasion = Dukes C. The wall invasion (through muscularis propria into pericolorectal fat = T3) is less important for the Dukes classification than the presence of nodal metastases. No distant metastases rules out Dukes D. Five-year survival for Dukes C is 30–40%, compared with >90% for Dukes A (confined within the wall, node-negative).