Page 17 of 28
PA23.8 | Colorectal Carcinoma — SDL Guide (Part 4)
Tumour Markers and Screening
CEA and Colorectal Cancer Screening
Carcinoembryonic antigen (CEA)
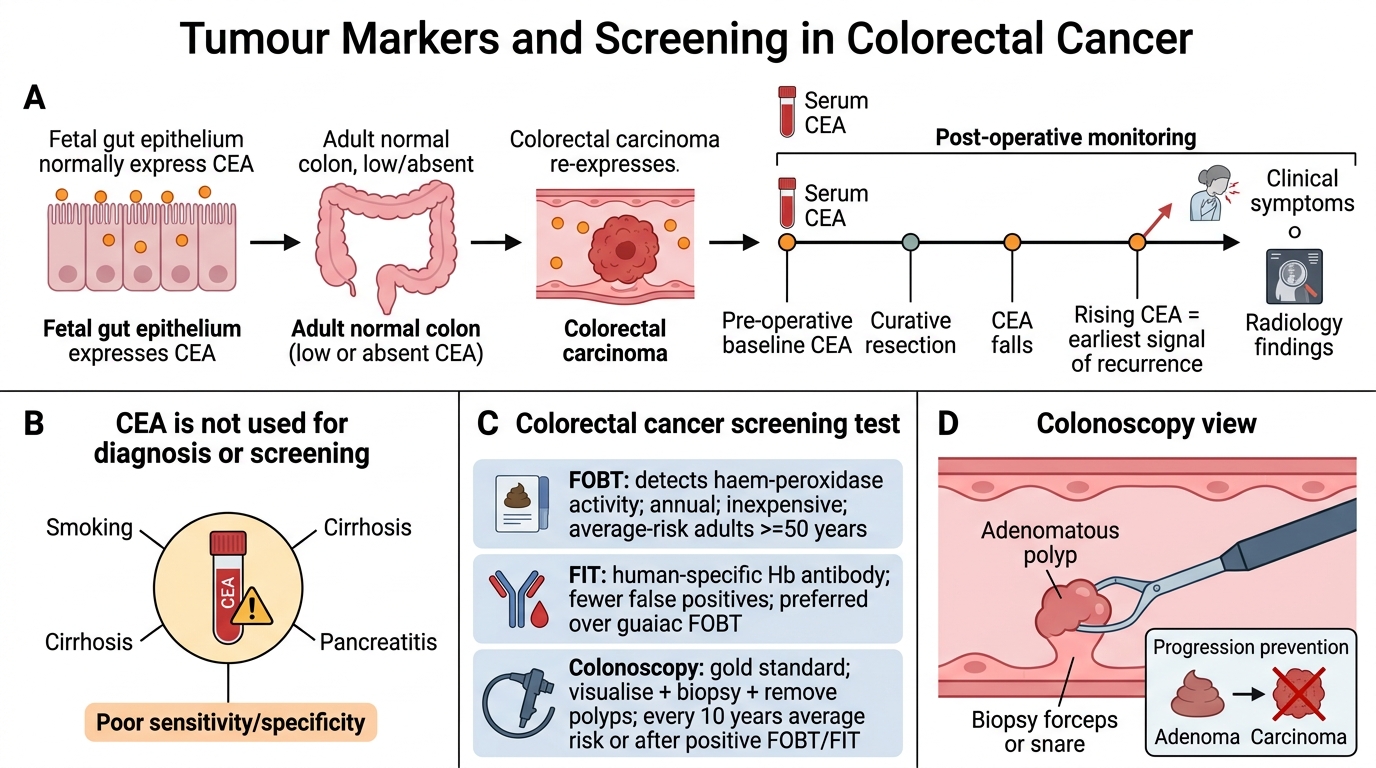
- CEA is an oncofetal glycoprotein normally expressed in fetal gut; re-expressed in CRC.
- Sensitivity/specificity for diagnosis: poor — elevated in smokers, cirrhosis, pancreatitis; NOT used for diagnosis or screening.
- Primary role: Post-operative monitoring for recurrence. Pre-operative CEA establishes baseline; rising CEA after curative resection is the earliest signal of recurrence (may precede clinical/radiological signs by months).
- Elevated pre-operative CEA correlates with advanced stage and poorer prognosis.
Screening (NMC-relevant):
| Method | Description | Population |
|---|---|---|
| FOBT (Faecal Occult Blood Test) | Detects haem-peroxidase activity; annual; inexpensive | Average-risk adults ≥50 years |
| Faecal immunochemical test (FIT) | Human-specific Hb antibody; fewer false positives than guaiac FOBT | Preferred over guaiac |
| Colonoscopy | Gold standard — visualise + biopsy polyps; removes adenomas | Every 10 years (average risk) or following positive FOBT |
| CT colonography | For incomplete/contraindicated optical colonoscopy | Selective use |
Key teaching point: Screening finds and removes adenomas before they become invasive — interrupting the adenoma-carcinoma sequence. This is why CRC is largely preventable.
CLINICAL PEARL
The two CRC presentations to instantly recognise in clinical exam:
- Elderly woman + iron-deficiency anaemia + positive FOBT + no visible bleeding → Right-sided CRC (caecum/ascending) — anaemia from occult blood loss through the exophytic fungating tumour into a wide, liquid-filled lumen.
- Middle-aged person + LIF pain + obstruction + pencil-thin stools + rectal bleeding → Left-sided CRC (sigmoid/rectum) — the napkin-ring lesion in a narrow, stool-packed lumen.
Remember: the same carcinoma at the molecular level but completely different presentations due solely to anatomy and luminal content. The classic USMLE/MBBS trap is attributing both presentations to a single image — left-sided lesions obstruct; right-sided lesions bleed silently.
SELF-CHECK
Which of the following is the CORRECT primary clinical application of CEA (carcinoembryonic antigen) in colorectal carcinoma?
A. Population screening in average-risk adults
B. Primary diagnosis when colonoscopy is unavailable
C. Post-operative monitoring for disease recurrence
D. Distinguishing adenocarcinoma from lymphoma histologically
Reveal Answer
Answer: C. Post-operative monitoring for disease recurrence
CEA lacks adequate sensitivity and specificity for diagnosis or screening — it is elevated in many benign conditions (smoking, cirrhosis) and is normal in ~40% of CRC at diagnosis. Its validated role is post-operative monitoring: a rising CEA after curative resection is the earliest indicator of recurrence and prompts imaging/re-staging. Pre-operative CEA level is also used as a prognostic baseline.