Page 19 of 28
PA23.9 | GI Morphology — Practical — SDL Guide
Learning Objectives
- Describe the gross and microscopic features of peptic ulcer, including the four-zone histological pattern.
- Identify and distinguish the microscopic features of TB, Crohn disease, ulcerative colitis, and typhoid ulcers.
- Recognise microscopic patterns of common GI tumours: oesophageal SCC, gastric adenocarcinoma (intestinal and diffuse types), colorectal adenocarcinoma, and adenomatous polyps.
- Distinguish benign inflammatory ulcers from malignant ulcers using gross and microscopic criteria.
- Apply a systematic approach — site → gross pattern → micro architecture → diagnostic label — when reading GI specimens.
INSTRUCTIONS
In Pathology practical examinations, GI specimens are among the most commonly tested. Being able to read a slide or photograph systematically and name the lesion — rather than memorising isolated facts — is the skill examiners test. This module walks you through each major GI entity with specimen-reading checkpoints so you can practise the thought process, not just recall the criteria.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 17 (Gastrointestinal Tract) (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 19 (GI Tract) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are handed a glass slide labelled 'stomach biopsy'. Under low power you see a large area of ulceration with layered zones beneath it. Under high power one zone shows actively proliferating capillaries and fibroblasts, and the deepest zone is dense, hypocellular, pink collagen. A nearby slide is labelled 'colorectum' and shows irregular, gland-forming epithelium with central dirty necrosis in the lumen. Two completely different diseases — yet the practical exam will ask you to name both in under two minutes. This module gives you the reading framework that makes that possible.
RECALL
Before starting, anchor your baseline:
- What are the four layers of the bowel wall from mucosa outward?
- Where in the stomach does peptic ulcer most commonly occur, and which nerve supplies the parietal cell?
- Name one microscopic difference between an intestinal-type and a diffuse-type carcinoma.
If any of these pause you, revisit your GI anatomy and SDL 1 (Normal Histology) before proceeding — they are the skeleton on which this module hangs.
The Systematic Reading Approach
Systematic Reading Approach for GI Specimens
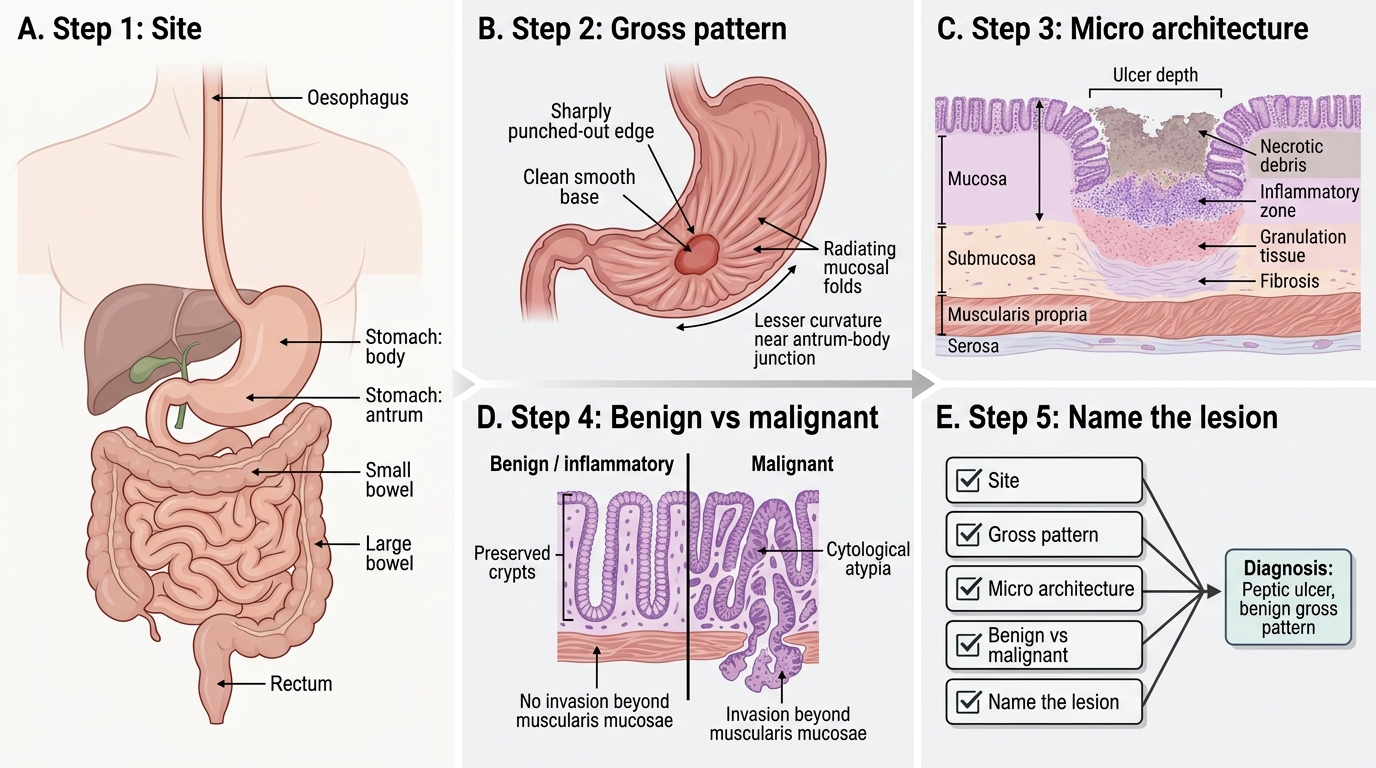
Every GI specimen — ulcer, tumour, or polyp — yields a diagnosis if you apply the same five-step scaffold:
- Site: Oesophagus? Stomach (body vs antrum)? Small bowel? Large bowel? The site constrains the differential immediately.
- Gross pattern: Single or multiple? Size and shape? Edge (punched-out vs rolled/heaped-up)? Base (clean vs necrotic)? Mucosal folds (converging vs destroyed)?
- Micro architecture (low power first): Ulceration depth (mucosal vs transmural)? Layered zones? Granuloma present? Gland formation? Mucin pattern?
- Benign/inflammatory vs malignant: Preserved crypt architecture? Cytological atypia? Invasion beyond muscularis mucosae?
- Name the lesion: Commit to the diagnosis using the features gathered above.
Training yourself to narrate these five steps — even on a photograph in an exam — prevents the most common student error: jumping to a memorised label without reading the slide.
Peptic Ulcer — Gross Features
Peptic Ulcer: Gross Features and Malignant Ulcer Contrast
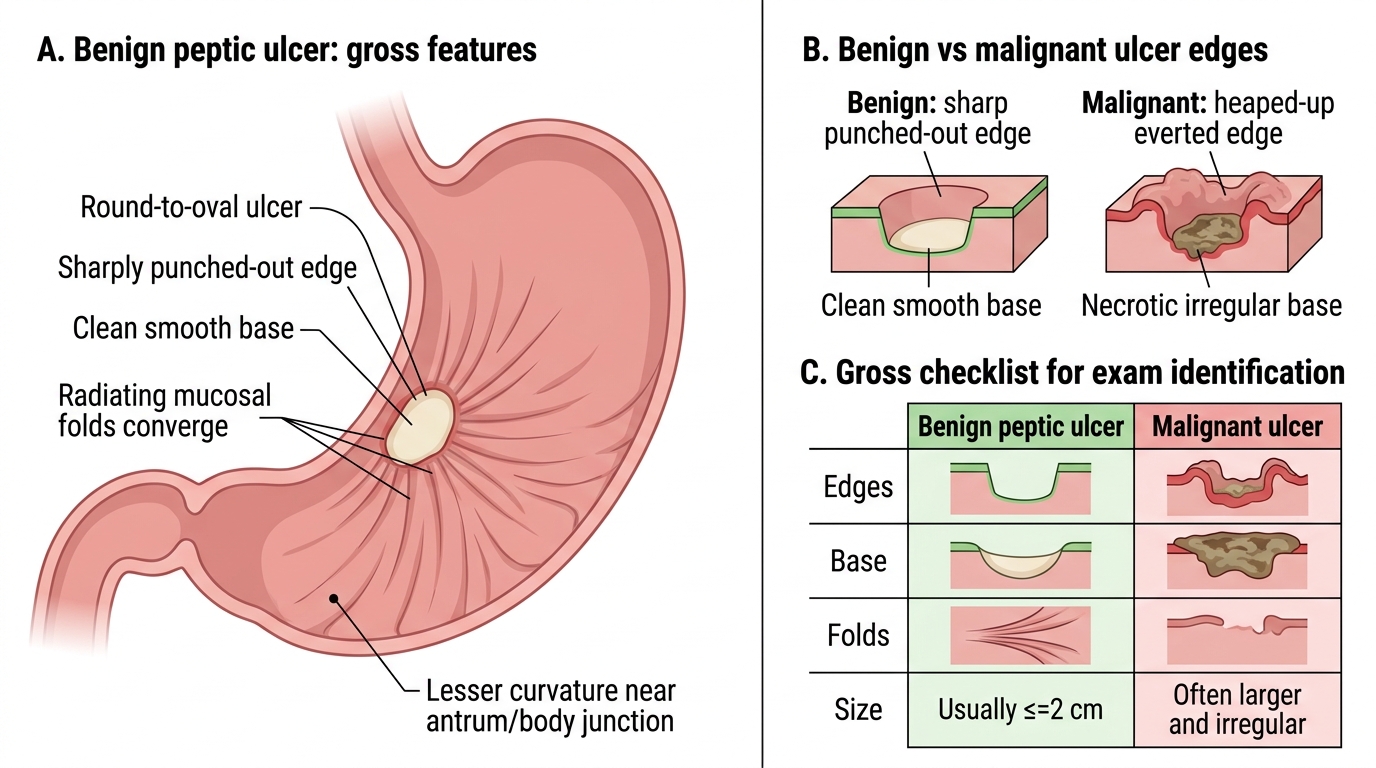
A peptic ulcer on gross examination has a set of features that together distinguish it from a malignant ulcer.
Benign (peptic) ulcer gross checklist:
- Size: usually ≤2 cm (most), rarely >3 cm
- Shape: round to oval, occasionally linear
- Edges: sharply punched-out, overhanging edge absent
- Base: clean, smooth — often described as 'floor of an operating theatre'
- Surrounding mucosa: folds converge towards the ulcer margin ('radiating folds')
- Location: most common on the lesser curvature of the antrum/body junction; first part of duodenum
Contrast this with a malignant (carcinomatous) ulcer: heaped-up, irregular, everted edges; necrotic, dirty base; surrounding folds are blunted, do not converge, or are destroyed.
IMPORTANT: This gross distinction is tested frequently — learn it as a 4-cell comparison table.
| Feature | Benign | Malignant |
|---|---|---|
| Edges | Punched-out, sharp | Heaped-up, everted |
| Base | Clean, smooth | Necrotic, irregular |
| Surrounding folds | Converging | Destroyed / blunted |
| Size | Usually ≤2 cm | Often >3 cm |
SELF-CHECK
A gastric resection specimen shows a 1.8 cm ulcer on the lesser curvature with sharply cut edges, a smooth pale base, and mucosal folds converging towards the margin. Which single gross feature most reliably supports a benign peptic ulcer over a malignant ulcer?
A. Size less than 2 cm
B. Converging mucosal folds
C. Smooth pale base
D. Location on the lesser curvature
Reveal Answer
Answer: B. Converging mucosal folds
Converging (radiating) mucosal folds are the most discriminating gross feature — they indicate that the surrounding mucosa is intact and contracting toward the ulcer, which occurs in reactive fibrosis of a benign peptic ulcer. Malignant ulcers destroy or disrupt these folds. Size <2 cm, smooth base, and lesser-curvature location are all supportive but individually less specific (small malignant ulcers and early carcinoma can share any one of these).
Peptic Ulcer — The Four Histological Zones
Peptic Ulcer: Four Histological Zones
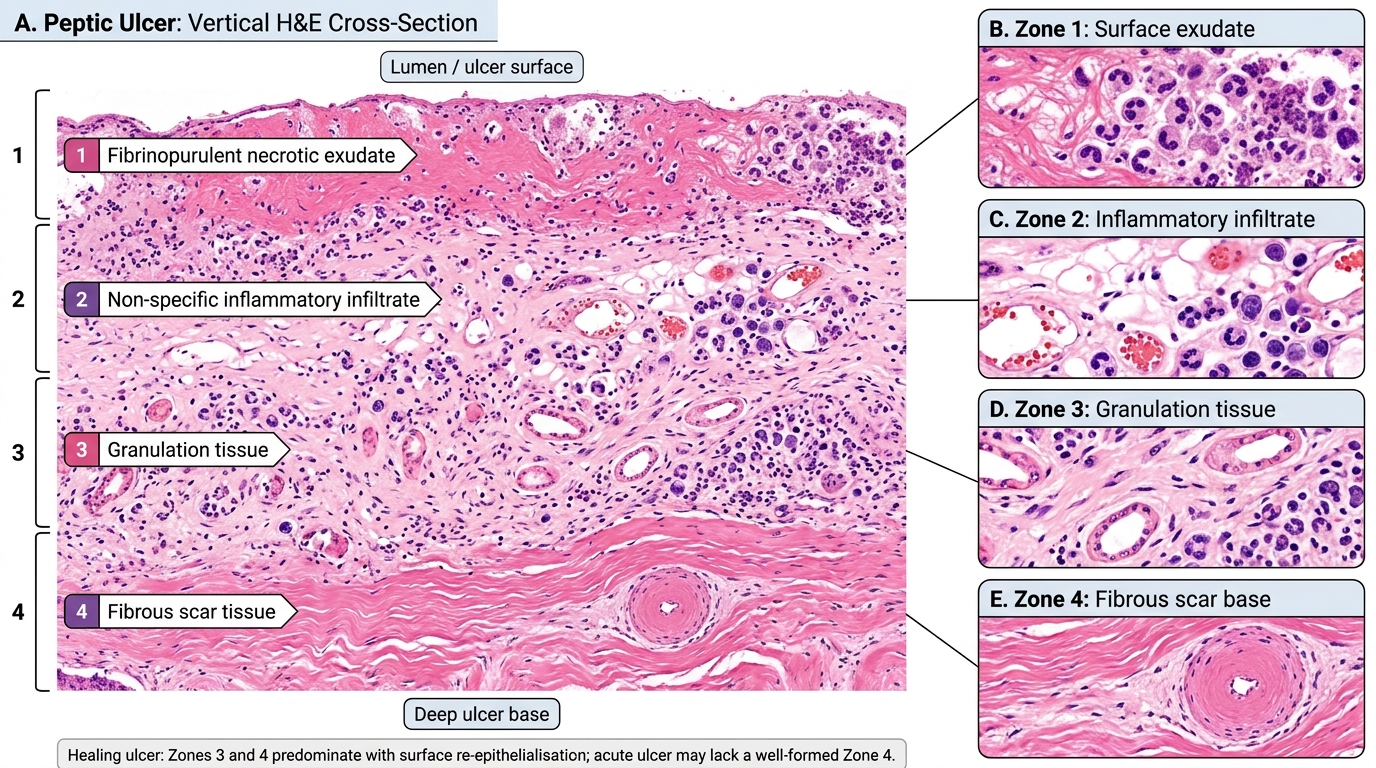
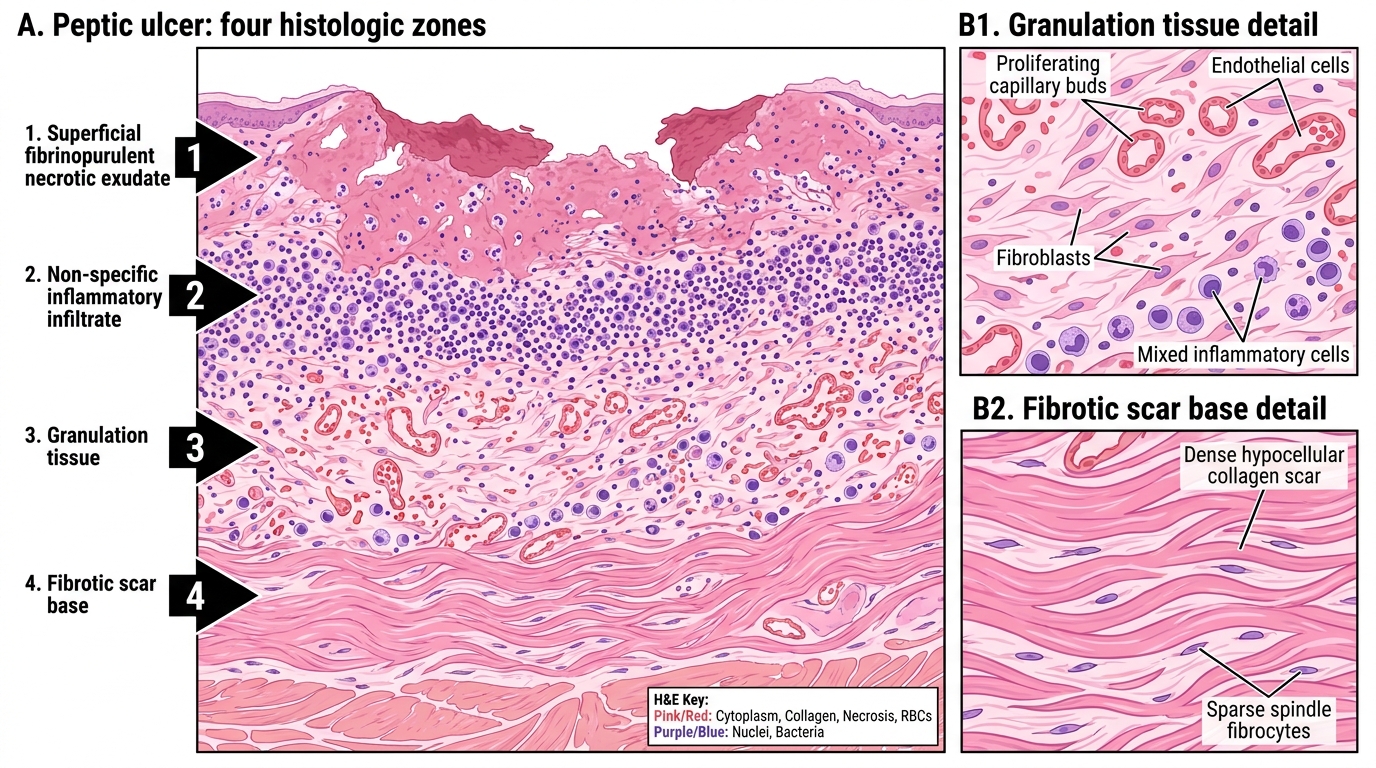
Under the microscope a peptic ulcer in its active phase shows four concentric zones from the lumen surface downward. Memorise them in order — the exam question usually asks you to label or sequence them.
Zone 1 — Fibrinopurulent necrotic exudate: The luminal surface. Fibrin, dead cell debris, neutrophils. Bright eosinophilic smear on H&E.
Zone 2 — Non-specific inflammatory infiltrate: Beneath the exudate. Oedema, vascular dilatation, neutrophils and mononuclear cells. Granulation tissue beginning to form at its lower border.
Zone 3 — Granulation tissue: Proliferating capillaries (endothelial buds), plump fibroblasts, mixed inflammatory cells. This zone indicates active healing attempt.
Zone 4 — Fibrous/scar tissue: The deepest zone. Dense, hypocellular collagen. In a chronic ulcer this layer is thick and may include arteries with endarteritis obliterans (thickened, hyalinised walls — this is why peptic ulcer bleeds: the artery cannot contract when eroded).
IMPORTANT: A healing ulcer shows zones 3 and 4 predominating with surface re-epithelialisation. An acute ulcer may lack a well-formed zone 4.
Histologic Zones of Chronic Peptic Ulcer
SELF-CHECK
On a peptic ulcer section you see plump spindle cells, delicate new capillaries, and mixed inflammatory cells in the middle layers of the ulcer floor. Which zone are you viewing, and what is its clinical significance?
A. Zone 1 (fibrinopurulent exudate) — indicates active bacterial infection
B. Zone 2 (non-specific inflammation) — indicates chronicity
C. Zone 3 (granulation tissue) — indicates healing attempt
D. Zone 4 (fibrosis) — indicates erosion of a vessel wall
Reveal Answer
Answer: C. Zone 3 (granulation tissue) — indicates healing attempt
Zone 3 is granulation tissue: proliferating capillary endothelial buds + fibroblasts + mixed inflammatory cells. Its presence confirms an active healing response. Zones are in order from the lumen down (1→4), so granulation tissue sits in the mid-floor. Zone 4 (fibrosis/scar) is the deepest; it is the layer in which arteries with endarteritis obliterans are found, making haemorrhage the key risk when this zone erodes.