Page 20 of 28
PA23.9 | GI Morphology — Practical — SDL Guide (Part 2)
Intestinal Ulcers — A Comparative Framework
Comparative Framework of Intestinal Ulcers
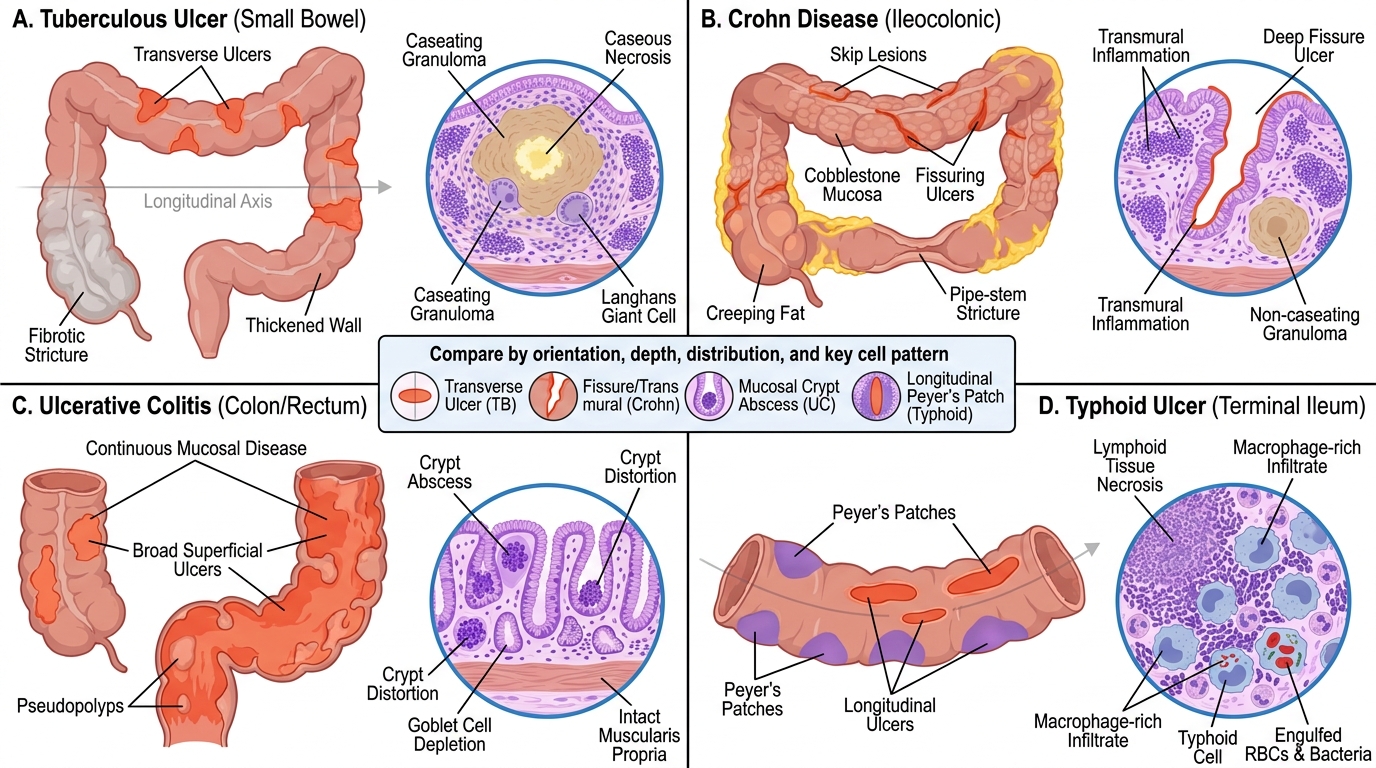
Four inflammatory ulcers of the intestine appear regularly in Pathology practicals. Read them as a comparison group, not as isolated facts.
Tuberculous (TB) ulcer (small bowel, ileocaecal region most common):
- Gross: transverse orientation (crosses the bowel axis), multiple, irregular; healed lesions form strictures
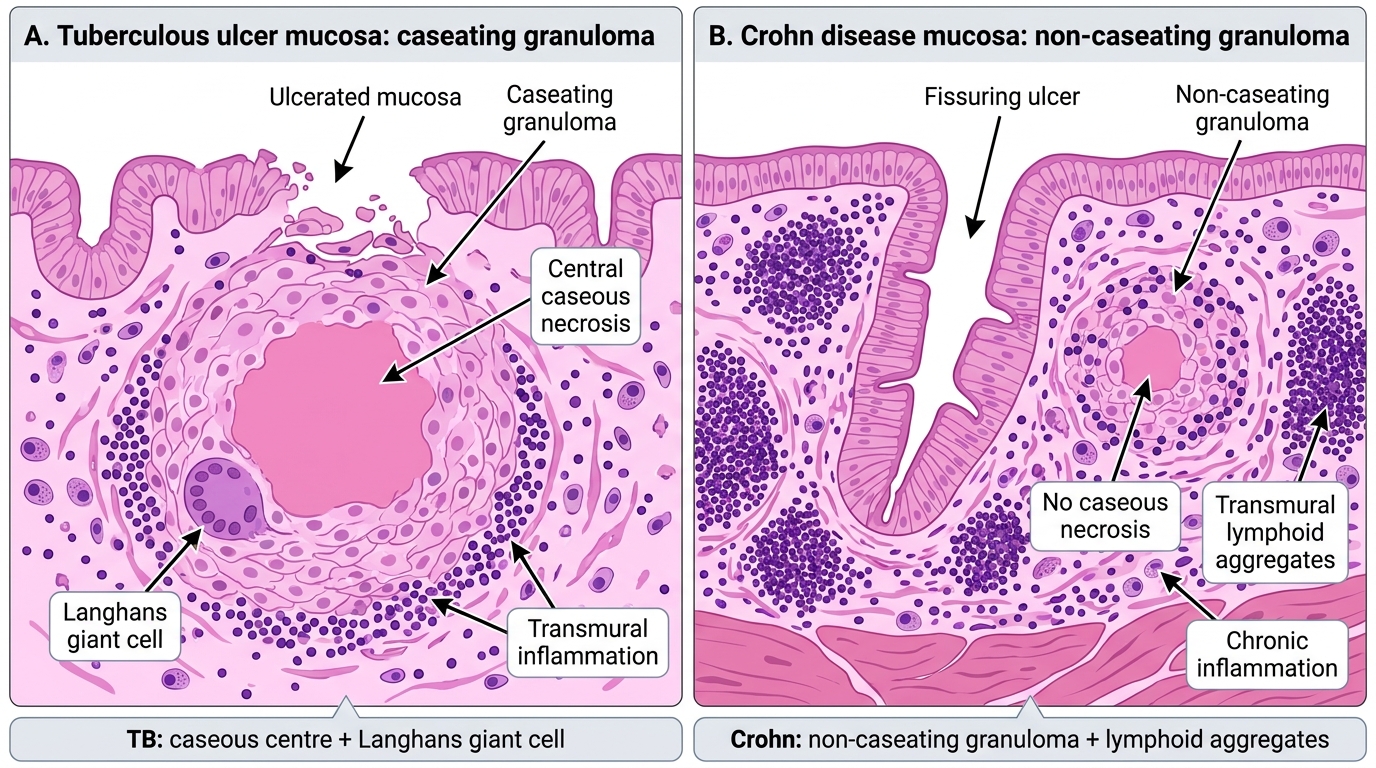
- Micro: caseating granulomas in the submucosa and deeper layers; Langhans giant cells present; central caseous necrosis; transmural inflammation
Crohn disease (ileocaecal most common, skip lesions anywhere):
- Gross: cobblestone mucosa (linear/fissuring ulcers between oedematous islands), skip lesions, creeping fat, pipe-stem strictures
- Micro: non-caseating granulomas (the key negative: no caseous centre); transmural inflammation; lymphoid aggregates in all layers; fissure ulcers; no crypt abscesses (in contrast to UC)
Ulcerative colitis (UC) (rectum upward, continuous):
- Gross: continuous mucosal involvement; pseudopolyps (islands of surviving inflamed mucosa between ulcers)
- Micro: ulceration confined to mucosa and superficial submucosa; crypt abscesses (neutrophils within crypts); crypt architectural distortion; goblet cell depletion; no granulomas; no transmural involvement
Typhoid ulcer (terminal ileum, Peyer's patches):
- Gross: longitudinal ulcers along the axis; located over Peyer's patches
- Micro: macrophage infiltration with engulfed red blood cells and bacteria (typhoid cells); necrosis of lymphoid tissue; Salmonella-specific picture
TB Ulcer vs Crohn Disease: Granuloma Histology
SELF-CHECK
A section from the terminal ileum shows transmural inflammation, non-caseating granulomas in the submucosa, and fissure ulcers penetrating toward the muscularis propria. Crypt abscesses are absent. The most likely diagnosis is:
A. Ulcerative colitis
B. Crohn disease
C. Tuberculous enteritis
D. Typhoid ulcer
Reveal Answer
Answer: B. Crohn disease
The combination of transmural inflammation + non-caseating granulomas + fissure ulcers + absence of crypt abscesses is the diagnostic fingerprint of Crohn disease. TB granulomas are caseating (central caseous necrosis). UC is mucosal only and characterised by crypt abscesses without granulomas. Typhoid shows macrophage-rich infiltrate (typhoid cells) over Peyer's patches, not granulomas.
CLINICAL PEARL
Granuloma type is the fastest discriminator between TB and Crohn. In the exam hall: look under medium power for the granuloma centre — if it is pink, amorphous, and structureless, it is caseation (TB). If the granuloma has a neat lymphocytic rim but a clear centre or just epithelioid histiocytes with no necrosis, it is non-caseating (Crohn). A common trap is mistaking the central eosinophilic material in a reactive/foreign-body granuloma for caseation — the distinction is sharpness: caseous necrosis is ghost-cell debris without nuclei, not refractile material.
GI Tumours — Systematic Microscopic Recognition
Microscopic Recognition of Common GI Tumours
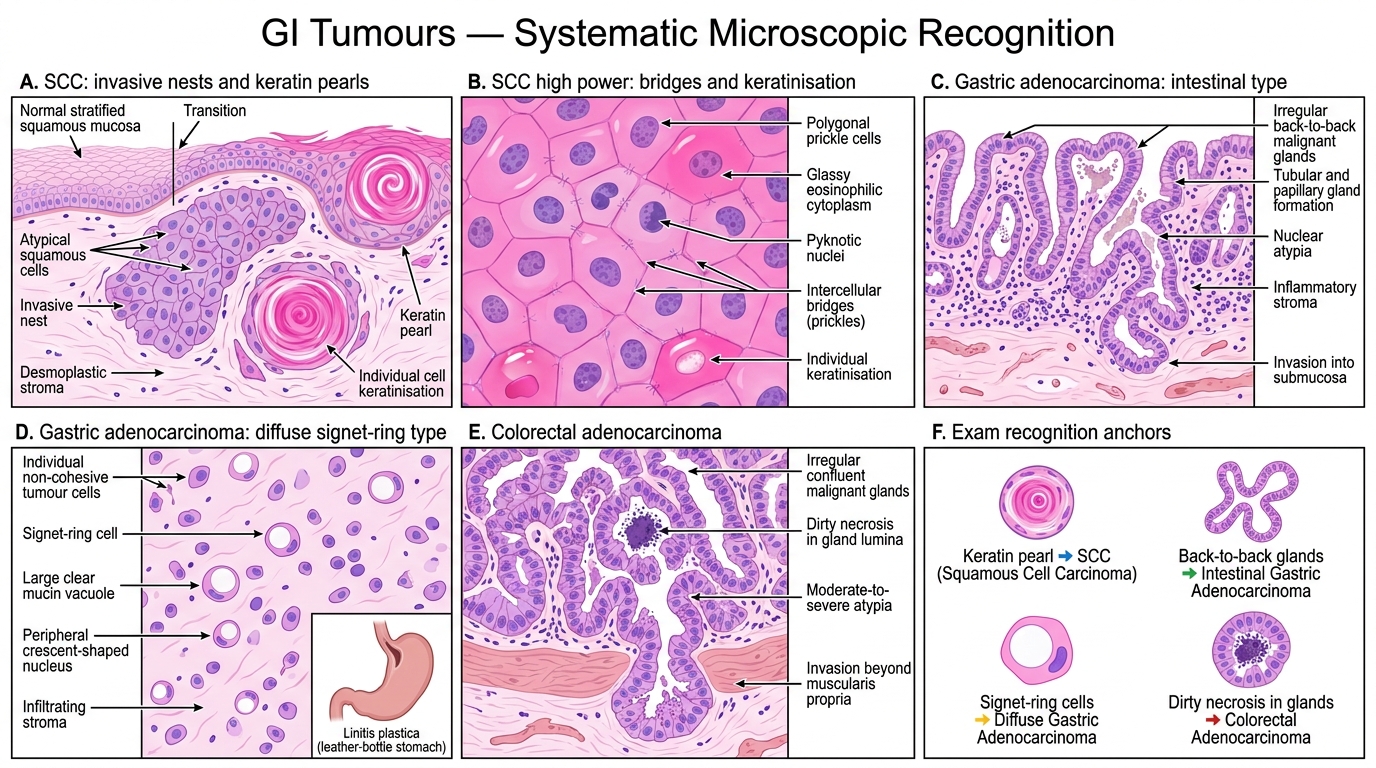
The practical exam presents tumour slides in groups. Anchor each tumour to its characteristic micro pattern.
Oesophageal / Oral squamous cell carcinoma (SCC):
- Pattern: sheets and nests of squamous cells with central keratin pearls (concentric whorls of pink, keratinised cells)
- Individual cell keratinisation (glassy pink cytoplasm, pyknotic nucleus) and intercellular bridges (prickle cells) on high power
- Stromal desmoplasia around invasive nests
Gastric adenocarcinoma — intestinal type:
- Pattern: irregular, back-to-back glands with moderate-to-severe cytological atypia; glandular architecture is recognisable (tubular or papillary)
- Invasion into the submucosa or deeper
- Inflammatory stroma; intestinal metaplasia often present in adjacent mucosa
Gastric adenocarcinoma — diffuse (signet-ring cell) type:
- Pattern: individual cells infiltrating the stroma, no gland formation
- Signet-ring cells: large intracytoplasmic mucin vacuole pushes the nucleus to the periphery, giving a 'signet ring' appearance on H&E
- Infiltrates diffusely through all layers; may cause linitis plastica (leather-bottle stomach) grossly
Colorectal adenocarcinoma:
- Pattern: irregular, confluent glands with moderate-to-severe atypia; luminal dirty necrosis (dark, granular, necrotic cell debris within gland lumina) is a classic clue
- Invasion through the muscularis propria; perineural or vascular invasion may be visible
- Tumour budding at the invasive front on low power
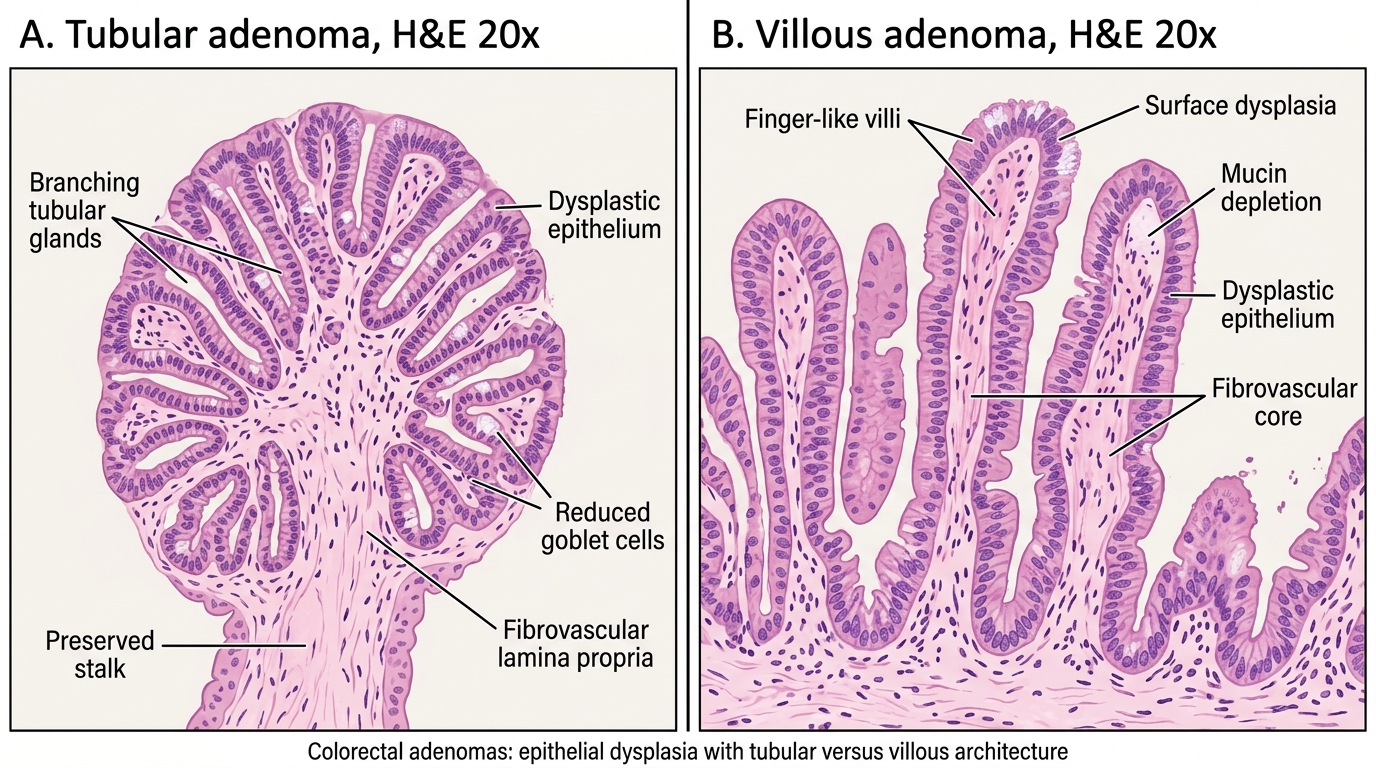
Adenomatous polyp (tubular vs villous):
- Tubular adenoma: branching tubular glands lined by dysplastic columnar epithelium; stalk present; low-grade dysplasia most common
- Villous adenoma: finger-like villi projecting from the surface; higher dysplasia risk; larger size
- Both are intramucosal dysplastic lesions — malignant transformation requires invasion through the muscularis mucosae
Tubular Adenoma versus Villous Adenoma
Four-Panel Composite: GI Specimen Identification Activity

GI Specimen Identification: Key Histologic Lesions
Use the image below as an H5P Image Hotspots identification exercise. For each panel, identify the lesion and its key diagnostic feature before expanding the hotspot.
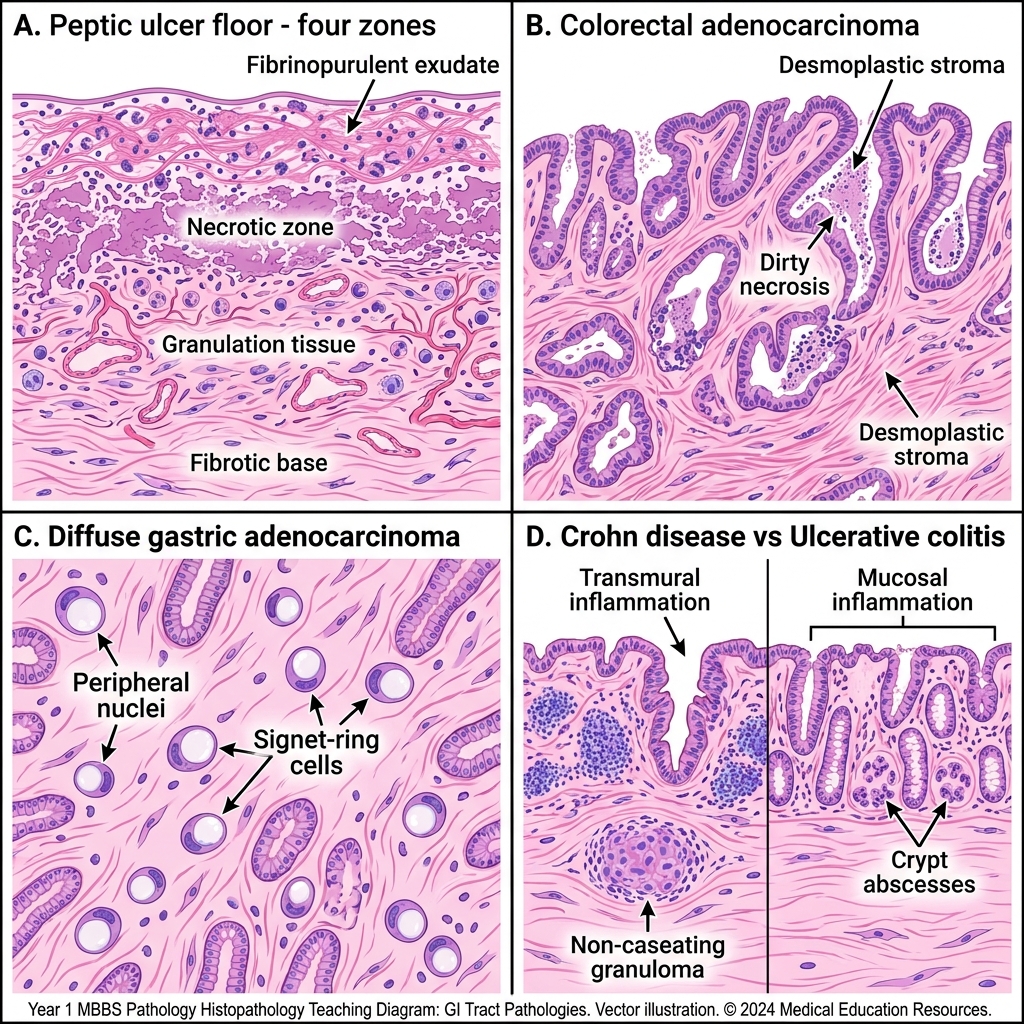
GI Histopathology: Ulcers and Adenocarcinoma Patterns
SELF-CHECK
A colorectal resection slide shows irregular malignant glands with central dark granular material filling the gland lumina. This finding is referred to as:
A. Caseous necrosis
B. Dirty necrosis
C. Comedonecrosis
D. Colliquative necrosis
Reveal Answer
Answer: B. Dirty necrosis
Dirty necrosis — dark, granular, necrotic tumour cell debris within malignant gland lumina — is a hallmark of colorectal adenocarcinoma on H&E. It contrasts with caseous necrosis (amorphous, pale, ghost-cell debris in TB granulomas) and comedonecrosis (central necrosis in cribriform ducts, classically DCIS of the breast). Dirty necrosis in a gland-forming tumour of the colorectum is essentially pathognomonic in the exam context.
SELF-CHECK
A gastric biopsy shows individually scattered cells with a large, clear intracytoplasmic vacuole displacing the nucleus to the cell periphery. These cells infiltrate the lamina propria without forming recognisable glands. Which tumour type and subtype does this describe?
A. Intestinal-type gastric adenocarcinoma
B. Diffuse-type gastric adenocarcinoma (signet-ring cell)
C. Gastric MALT lymphoma
D. Metastatic lobular breast carcinoma
Reveal Answer
Answer: B. Diffuse-type gastric adenocarcinoma (signet-ring cell)
The description — solitary cells with mucin vacuole pushing nucleus to periphery, no gland formation, diffuse infiltration — is the classic signet-ring cell pattern of diffuse-type gastric adenocarcinoma. Intestinal-type forms recognisable glands. MALT lymphoma shows lymphoid cells with lymphoepithelial lesions. Metastatic lobular carcinoma from the breast can produce an identical picture (both are signet-ring patterns) — clinical context and immunohistochemistry (CDX2, CK20 for gastric; ER, GATA3 for breast) distinguish them.