Page 21 of 28
PA23.9 | GI Morphology — Practical — SDL Guide (Part 3)
Distinguishing Benign from Malignant Ulcer — Micro Criteria
Benign vs Malignant Gastric Ulcer: Microscopic Criteria
Gross features were covered earlier; now consolidate the microscopic criteria.
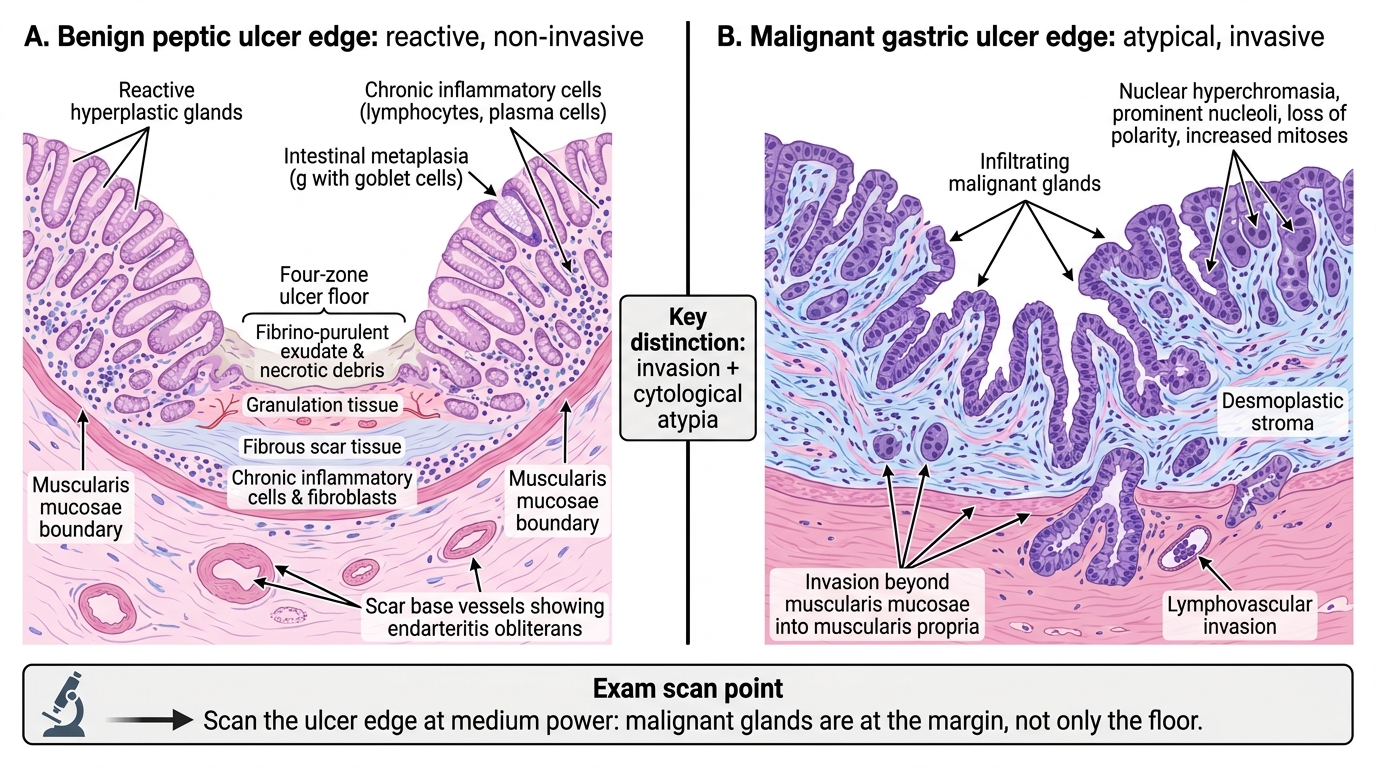
Benign peptic ulcer micro:
- Ulceration with the four-zone floor
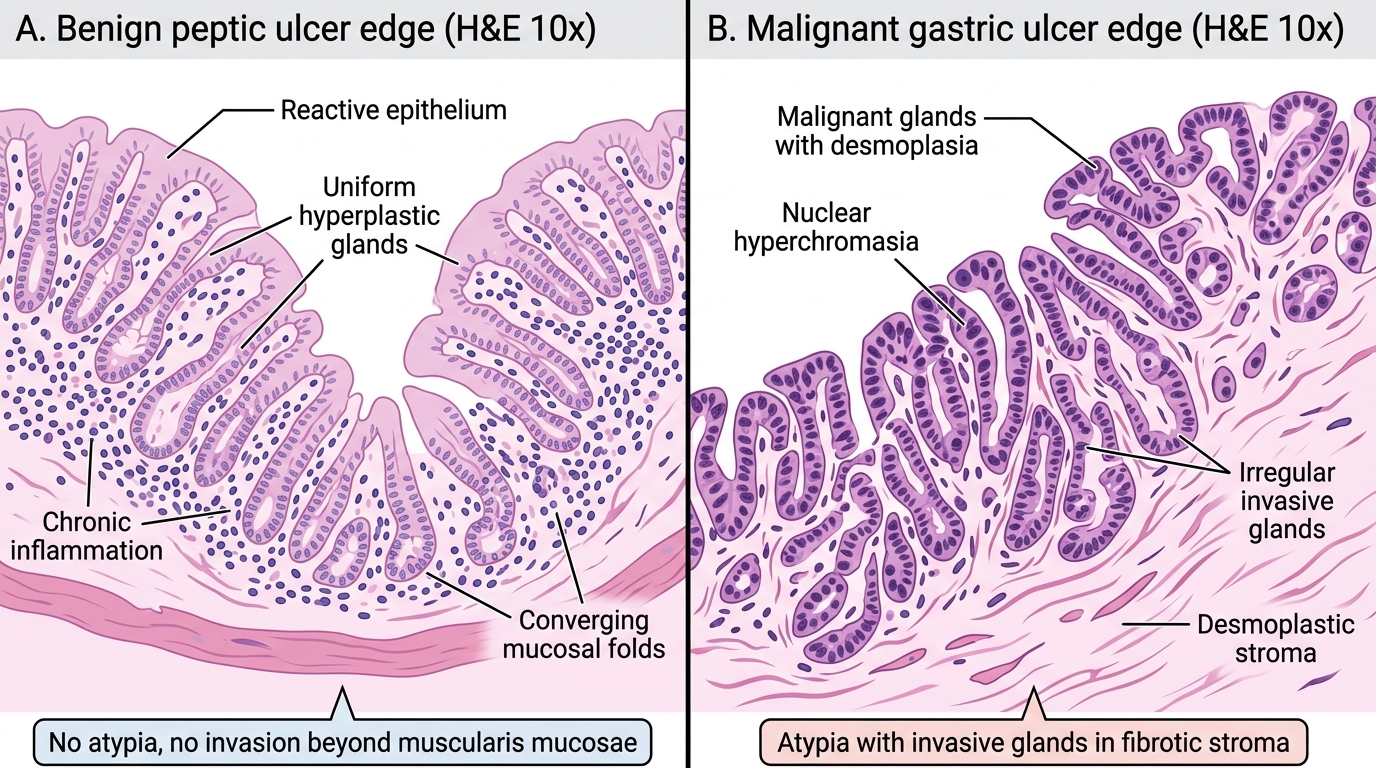
- Surrounding mucosa shows intestinal metaplasia, hyperplastic glands (reactive), and chronic inflammation — but NO cytological atypia in the glands
- No invasion beyond the muscularis mucosae in the surrounding epithelium
- Vessels with endarteritis obliterans in the scar base
Carcinomatous ulcer micro:
- Irregular malignant glands at the ulcer edge and base (intestinal type) OR signet-ring cells (diffuse type)
- Stromal desmoplasia (reactive fibrous stroma around invasive glands)
- Invasion beyond muscularis mucosae, often into muscularis propria or deeper
- Cytological atypia: hyperchromatic nuclei, prominent nucleoli, loss of polarity, increased mitoses
- Lymphovascular invasion may be present at the edge
Practical tip: In an exam slide of a gastric ulcer, always scan the edge of the ulcer at medium power — malignant glands are found at the ulcer margin, not just in the floor. Benign reactive epithelium at the edge is flat or slightly hyperplastic but nuclei are uniform.
Benign vs Malignant Gastric Ulcer Edge: Microscopy
CLINICAL PEARL
The most important three words in a GI pathology practical report are: site, architecture, cytology. Site tells you the differential. Architecture (glands present or absent? granulomas? transmural or mucosal?) narrows it. Cytology (atypia, signet-ring, keratin pearls, mitoses?) clinches benign vs malignant and specific tumour type. Every slide yields to these three questions in order — do not reverse them.
SELF-CHECK
A student reads a gastric ulcer slide and reports: 'The ulcer edge shows mildly enlarged nuclei but they are uniform and the glands are regular.' The most appropriate interpretation is:
A. Reactive (regenerative) epithelial changes — consistent with benign ulcer
B. High-grade dysplasia requiring repeat biopsy
C. Signet-ring cell carcinoma — must report urgently
D. Intestinal metaplasia with early malignant transformation
Reveal Answer
Answer: A. Reactive (regenerative) epithelial changes — consistent with benign ulcer
Mildly enlarged but uniform nuclei with regular gland architecture at the edge of a peptic ulcer are reactive/regenerative changes — not dysplasia. Regenerating epithelium has increased nucleocytoplasmic ratio and mitotic activity but retains nuclear uniformity, polarity, and orderly gland architecture. High-grade dysplasia requires marked nuclear pleomorphism, loss of polarity, and architectural complexity. Signet-ring carcinoma has solitary cells with mucin vacuoles, not glands. Intestinal metaplasia is a specific goblet-cell change, not what's described here.