Page 9 of 28
PA23.5-7 | Intestinal TB, Appendicitis, IBD & Malabsorption — SDL Guide
Learning Objectives
- Describe the etiology, pathogenesis, and pathological forms of intestinal tuberculosis, and distinguish it from Crohn disease
- Explain the pathogenesis and morphological stages of acute appendicitis, including complications
- Compare Crohn disease and ulcerative colitis across distribution, gross morphology, microscopy, complications, and extraintestinal manifestations
- Enumerate the causes of malabsorption syndrome and describe the laboratory approach to its diagnosis
INSTRUCTIONS
Gastrointestinal pathology is a high-yield area in Indian clinical medicine — intestinal tuberculosis mimics Crohn disease on endoscopy, appendicitis is the commonest surgical emergency, and tropical sprue is a diagnosis you will make in your own patient population. This module links pathological mechanisms directly to clinical presentations and investigations you will order as a doctor.
References
- Robbins & Kumar Basic Pathology, 11th ed., Ch 14 (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 17 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old woman from rural Tamil Nadu presents with 3 months of right iliac fossa pain, weight loss, and a palpable mass. Colonoscopy shows ulceration and narrowing at the ileocaecal junction. The gastroenterologist and the surgeon are debating: is this Crohn disease or intestinal tuberculosis? The biopsy report arrives — and the pathologist's words will determine whether she gets steroids or anti-TB therapy. One wrong call is life-threatening. By the end of this module, you will know exactly what to look for on that biopsy.
WHY THIS MATTERS
India carries the world's highest burden of intestinal tuberculosis. Appendicitis is the most common acute surgical abdomen you will manage as a house officer. Inflammatory bowel disease is rising in urban India. Coeliac disease and tropical sprue cause preventable nutritional failure. These four conditions together underlie a large fraction of the gastrointestinal surgery and medicine admissions in any Indian tertiary hospital.
RECALL
Before you start, recall from Year-1:
• Mycobacterium tuberculosis — acid-fast bacillus, caseating granuloma as the hallmark lesion.
• The appendix — a blind-ended diverticulum of the caecum; lymphoid tissue is prominent in childhood.
• Autoimmune disease concept — immune response targeting self or luminal antigens.
• Malabsorption — failure to absorb nutrients in the small intestine; leads to steatorrhoea and nutritional deficiencies.
Hold these in mind as we build on them.
Intestinal Tuberculosis — Forms and Pathogenesis
Intestinal Tuberculosis: Routes, Pathogenesis, and Forms
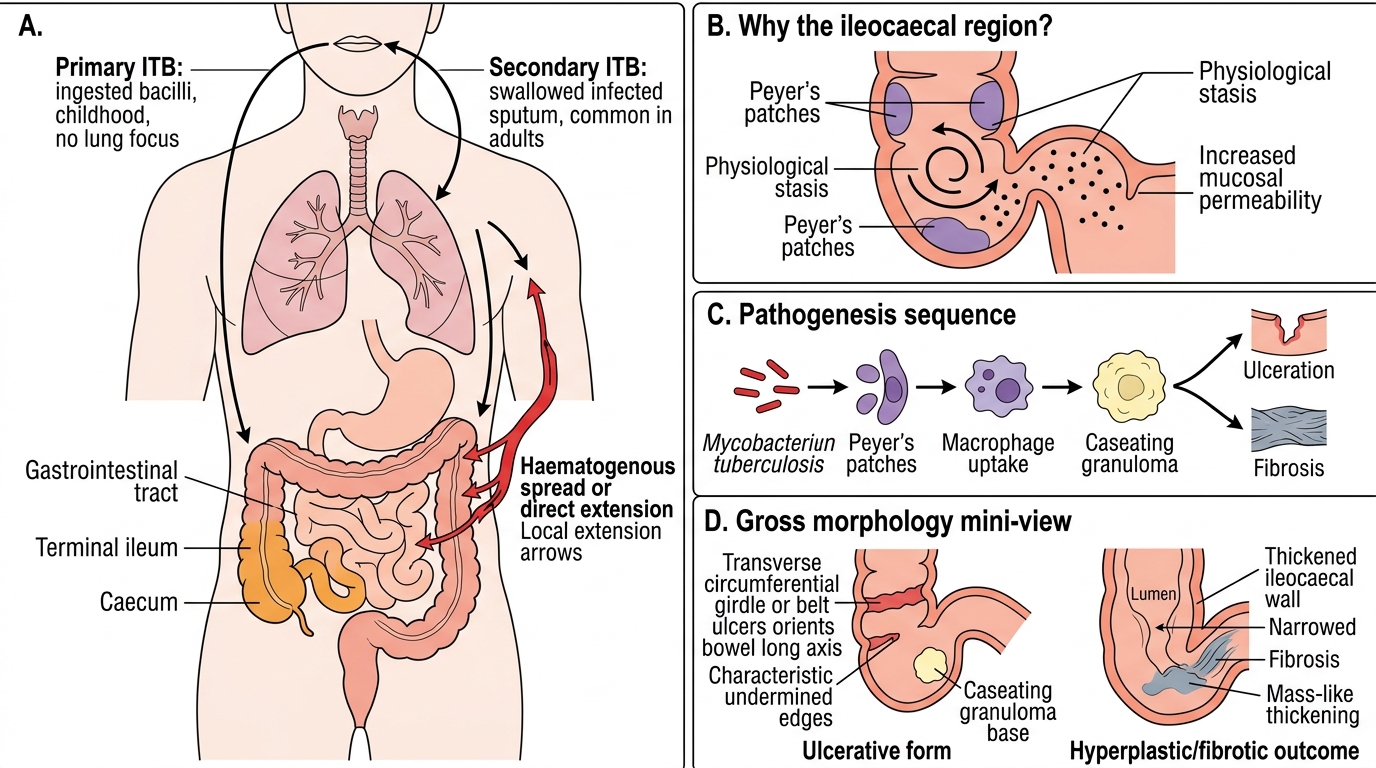
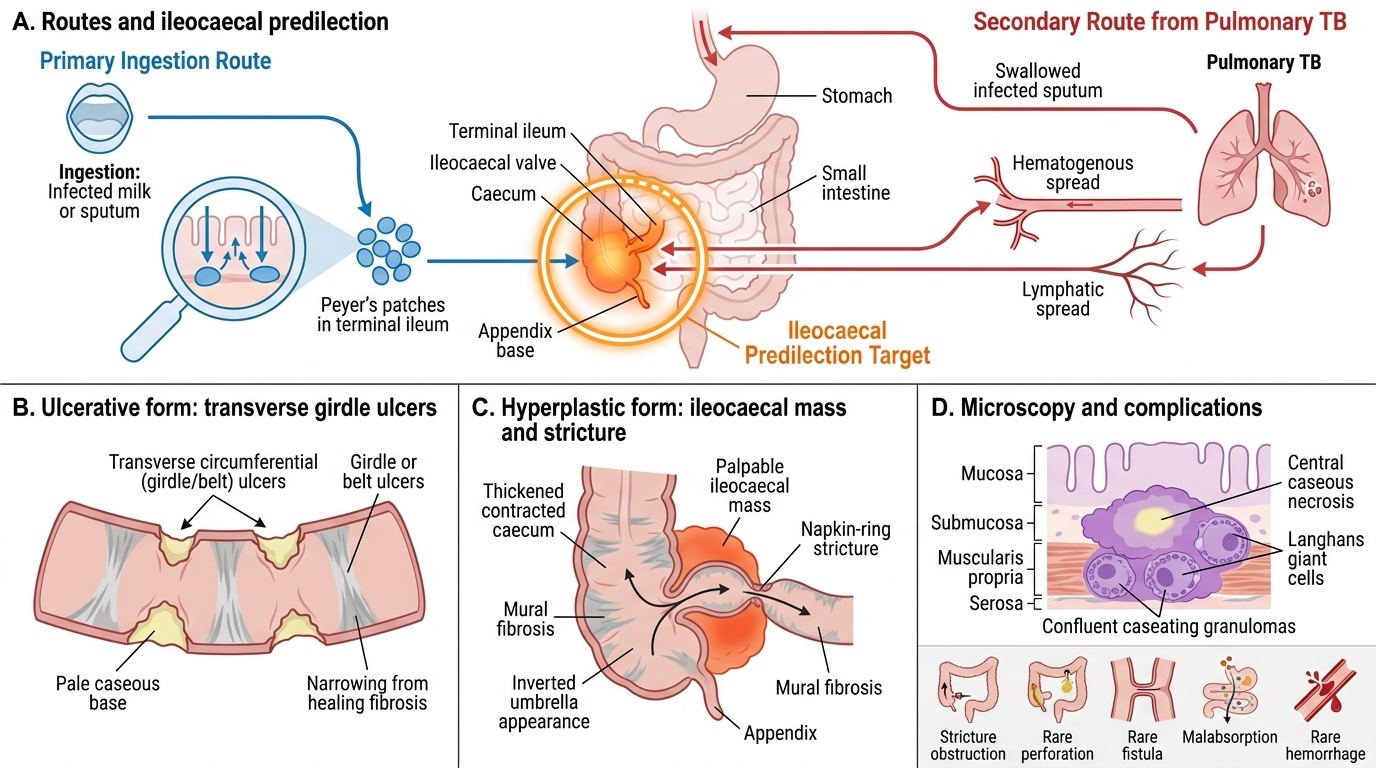
Intestinal tuberculosis (ITB) is caused by Mycobacterium tuberculosis (occasionally M. bovis from unpasteurised milk). It reaches the gut by one of three routes:
1. Primary ITB — ingestion of bacilli in childhood; no lung focus; Peyer's patches in the terminal ileum are the entry point.
2. Secondary ITB — swallowing infected sputum from pulmonary TB (most common in adults).
3. Haematogenous spread or direct extension from adjacent organs (less common).
Why the ileocaecal region? The terminal ileum and caecum are the preferred sites because of abundant lymphoid tissue (Peyer's patches), physiological stasis, and increased mucosal permeability at this junction — providing ideal conditions for mycobacterial implantation.
Pathogenesis: Bacilli enter Peyer's patches → macrophage uptake → caseating granuloma formation → ulceration or fibrosis depending on host immunity.
Intestinal Tuberculosis: Routes, Ileocaecal Predilection, and Morphology
Intestinal Tuberculosis — Morphological Forms
Morphological Forms of Intestinal Tuberculosis
Ulcerative form (more common, ~60%):
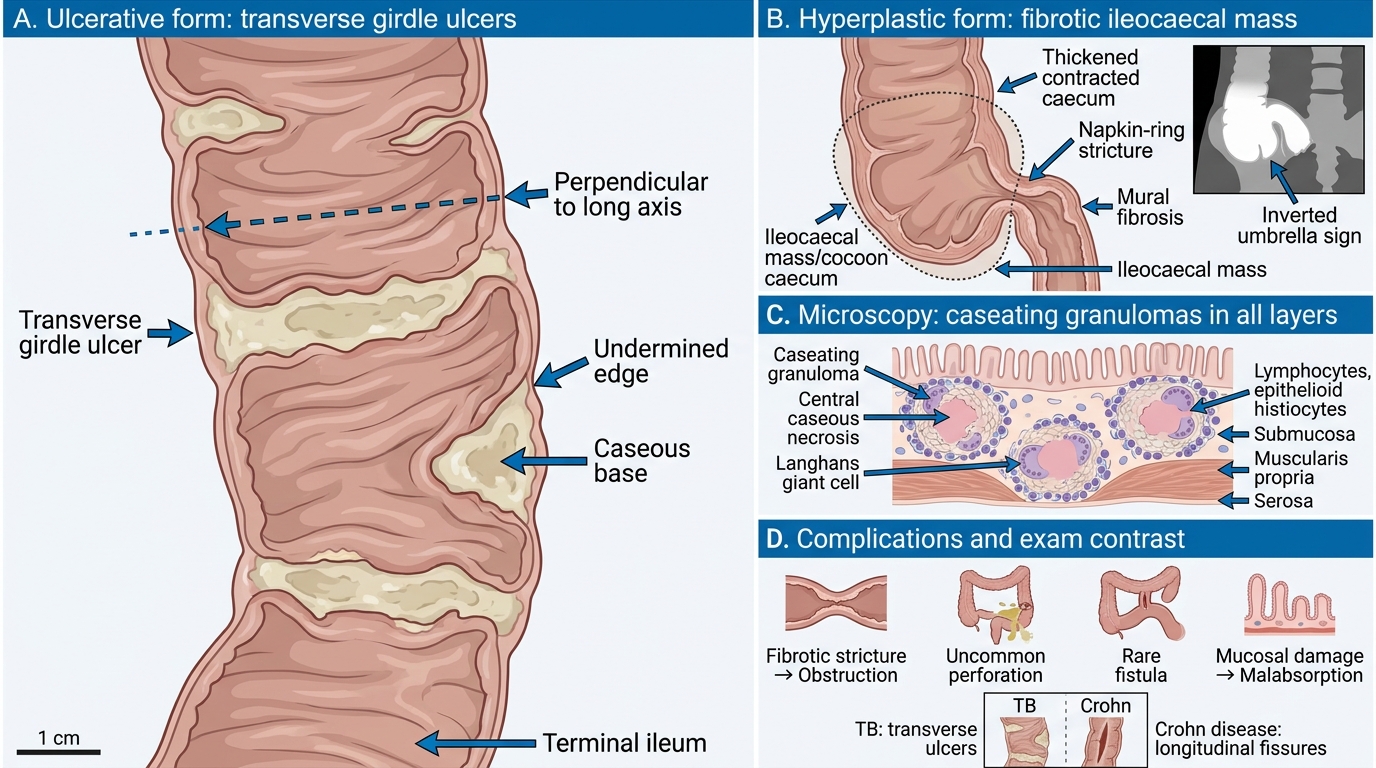
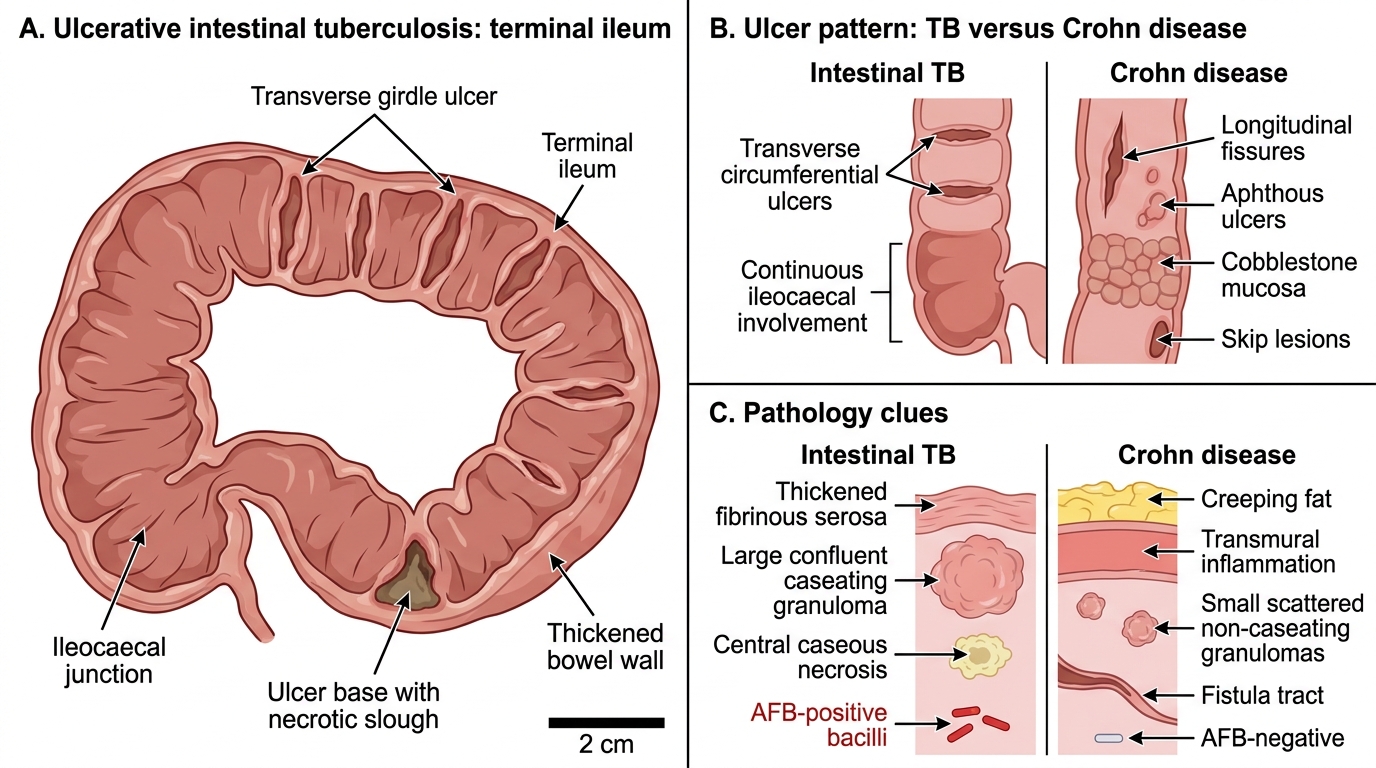
• Transverse ulcers that run around the circumference — hence called 'girdle' or 'belt' ulcers. This is the pathognomonic gross feature.
• Ulcers are perpendicular to the long axis of the bowel (contrast with Crohn's longitudinal fissures).
• Base shows caseating granulomas; edges are undermined.
• Heals with fibrosis → stricture.
Hyperplastic (hypertrophic) form (~40%):
• Marked fibrosis and mural thickening produce a napkin-ring stricture or a palpable ileocaecal mass (the 'cocoon' caecum).
• The caecum is thickened and contracted — radiologically the 'inverted umbrella' sign.
• More commonly confused with carcinoma or Crohn disease clinically.
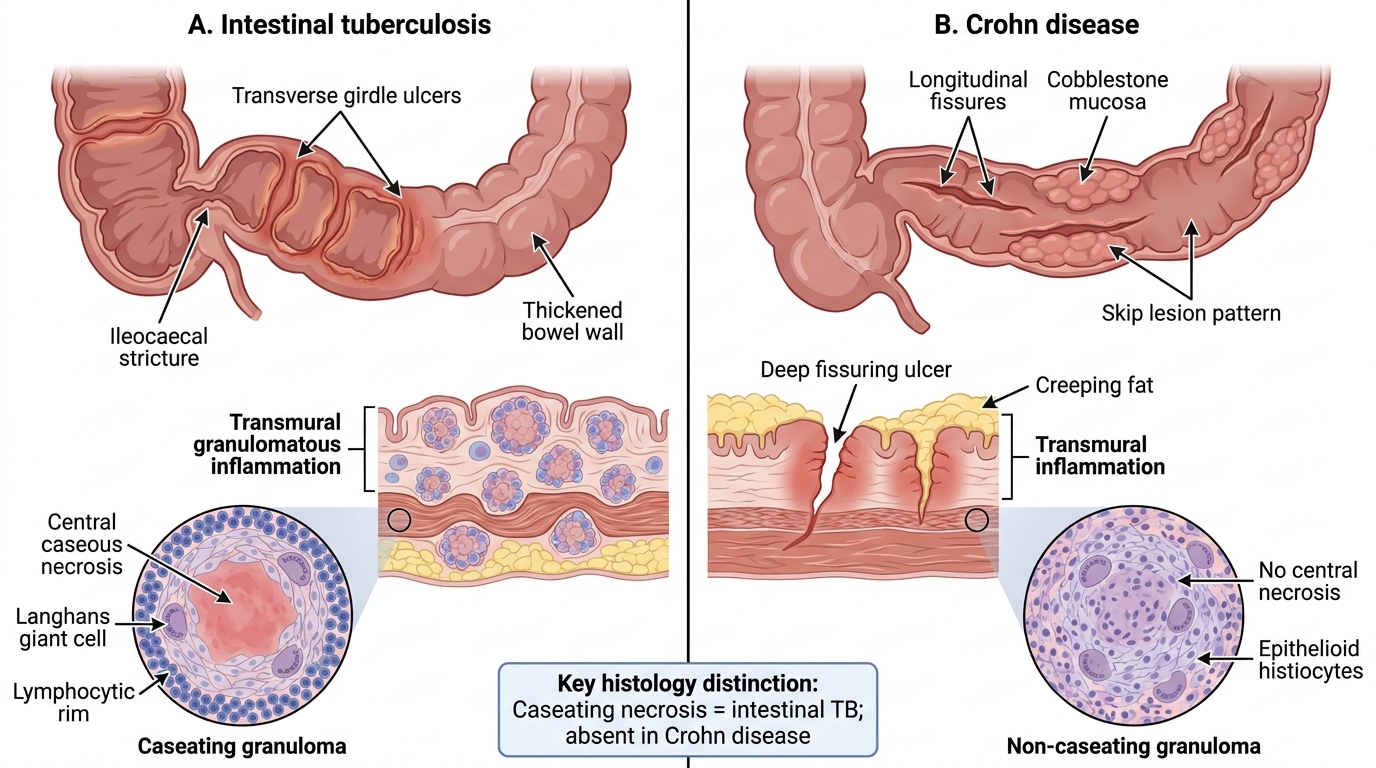
Microscopy (both forms): Caseating granulomas in all layers — submucosa, muscularis, serosa. Granulomas are larger, more numerous, and confluent compared with Crohn disease. Langhans giant cells are characteristic.
Complications: Stricture and obstruction (commonest), perforation (uncommon — fibrosis protects), fistulae (rare vs Crohn), malabsorption from mucosal damage, and rarely haemorrhage.
Intestinal TB vs Crohn Disease: Ileocaecal Clues
Intestinal TB vs Crohn Disease — The India-Critical Distinction
Intestinal TB vs Crohn Disease: Ileocaecal Clues
This comparison is tested in exams and saves lives in practice. Both cause ileocaecal disease with granulomas.
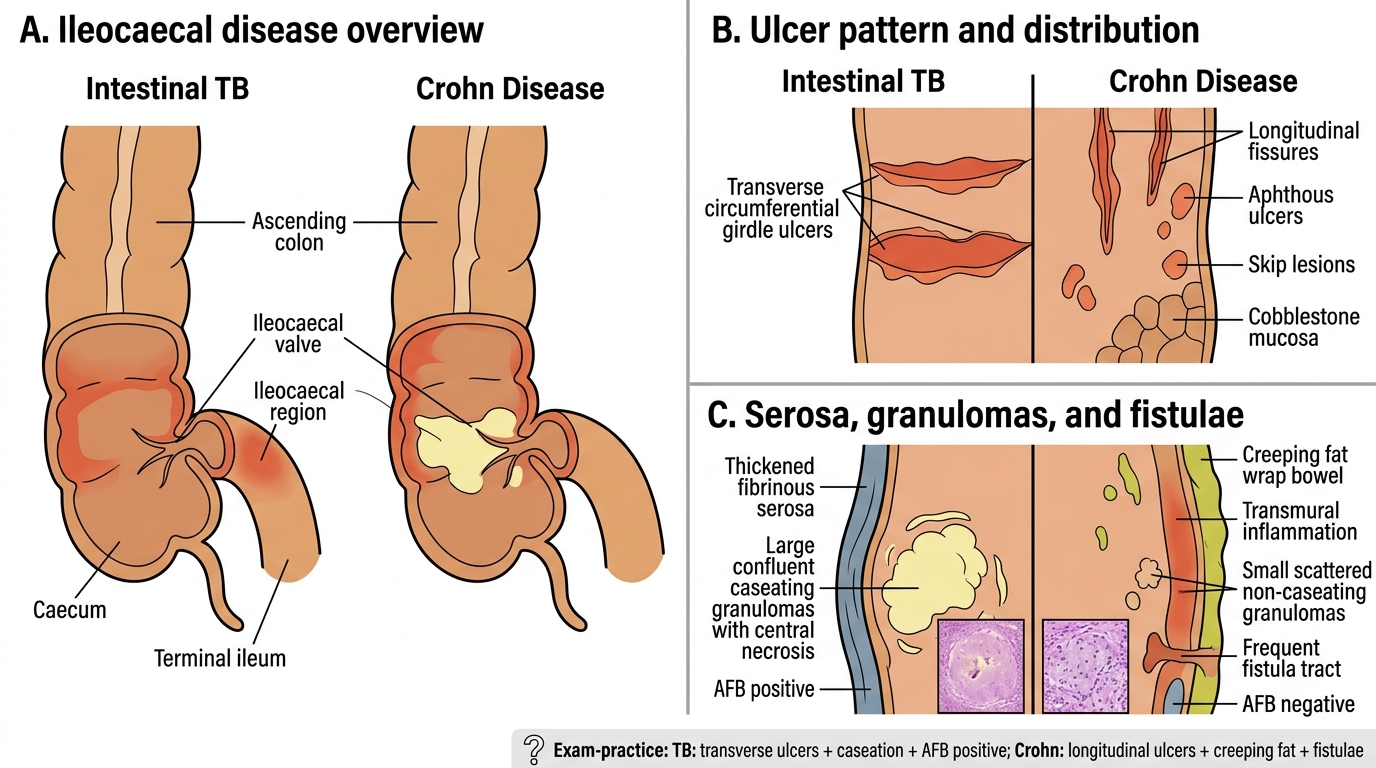
| Feature | Intestinal TB | Crohn Disease |
|---|---|---|
| Ulcer orientation | Transverse (girdle) | Longitudinal fissures + aphthous |
| Granulomas | Caseating, large, confluent | Non-caseating, small, scattered |
| Serosa | Thickened, fibrinous | Creeping fat wrapping |
| Fistulae | Rare | Very common |
| Skip lesions | No (usually continuous at site) | Yes |
| AFB smear/PCR | Positive (or culture) | Negative |
| Mantoux/IGRA | Usually positive | Negative |
| Response to steroids | Worsens (or masks) | Improves |
Clinical pearl: In India, NEVER start steroids for presumed Crohn disease without first excluding TB by Mantoux, IGRA, and biopsy PCR. Steroid immunosuppression converts latent TB to disseminated disease.
Intestinal TB vs Crohn Disease
SELF-CHECK
A biopsy from an ileocaecal stricture in a 28-year-old shows large, confluent granulomas with central caseous necrosis involving all bowel wall layers. Which single feature most definitively distinguishes intestinal tuberculosis from Crohn disease on histology?
A. Caseating necrosis within granulomas
B. Transmural inflammation
C. Presence of Langhans giant cells
D. Mucosal ulceration
Reveal Answer
Answer: A. Caseating necrosis within granulomas
Caseating necrosis is the histological hallmark of TB granulomas and is absent in Crohn disease. Both conditions show transmural inflammation and giant cells. Ulceration occurs in both. Caseous necrosis on biopsy, confirmed by AFB stain or PCR, drives the decision to treat as TB rather than IBD.