Page 10 of 28
PA23.5-7 | Intestinal TB, Appendicitis, IBD & Malabsorption — SDL Guide (Part 2)
Acute Appendicitis — Pathogenesis
Acute Appendicitis: Pathogenesis Cascade
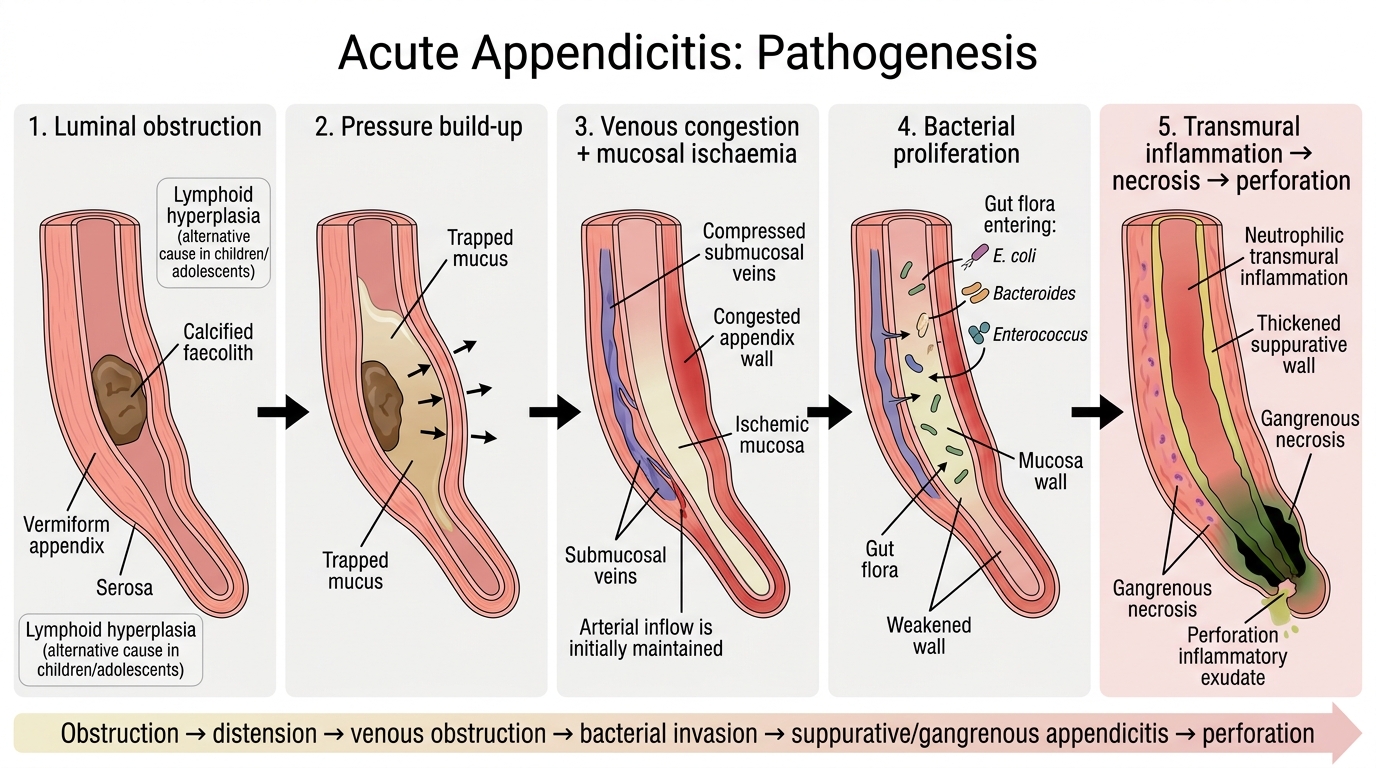
Acute appendicitis is the most common cause of an acute surgical abdomen worldwide. The pathogenetic sequence follows a logical cascade:
- Luminal obstruction — by a faecolith (calcified stool, ~35%), lymphoid hyperplasia (commonest in children/adolescents), foreign body, tumour, or inspissated mucus.
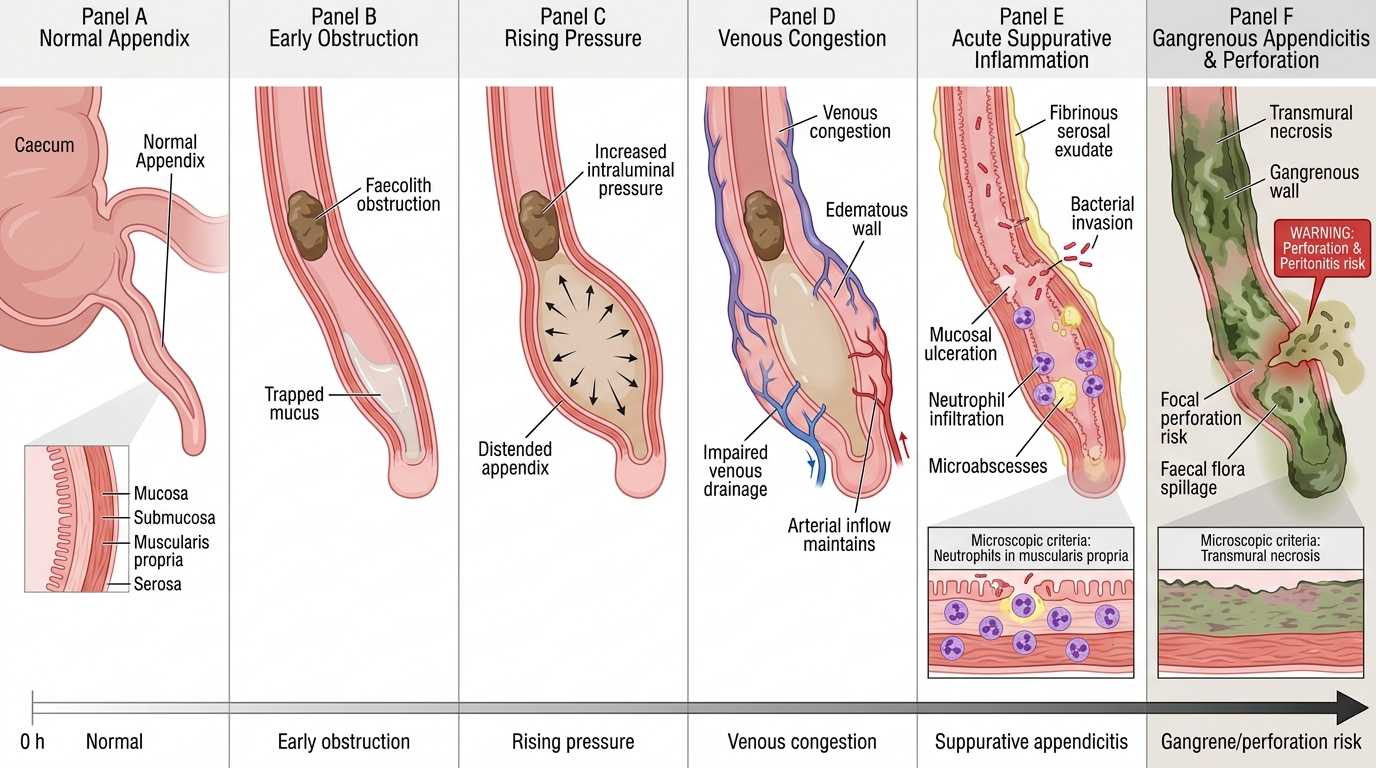
- Increased intraluminal pressure — continued mucous secretion behind the obstruction distends the lumen.
- Venous obstruction and mucosal ischaemia — rising pressure compresses submucosal veins; arterial supply initially maintained.
- Bacterial proliferation — mucosal ischaemia allows transmural invasion by gut flora (E. coli, Bacteroides, Enterococcus).
- Transmural inflammation — the appendix becomes acutely inflamed → suppurative → gangrenous → perforation.
Note: In children, lymphoid hyperplasia (from viral infections — adenovirus, measles) is the most common precipitant, not a faecolith.
Stepwise Pathogenesis of Acute Appendicitis
Acute Appendicitis — Morphology and Complications
Acute Appendicitis: Morphology and Complications
Gross and microscopic stages:
Acute (early) appendicitis:
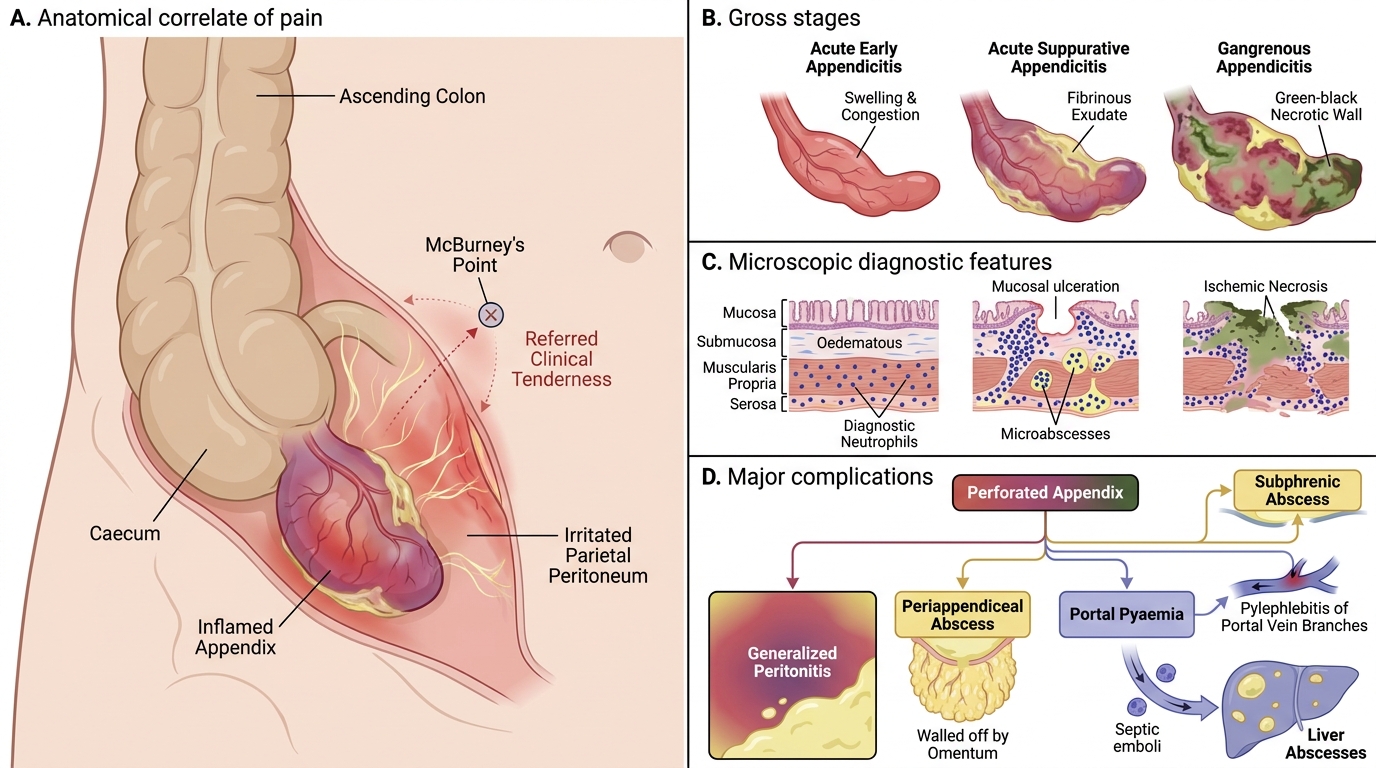
• Appendix mildly congested; serosal vessels dilated.
• Microscopy: neutrophil infiltration of the muscularis propria — this is the diagnostic criterion (neutrophils in the muscle layer, not just the mucosa).
Suppurative (acute suppurative) appendicitis:
• Appendix grossly swollen, tense, red-purple with fibrinous exudate on serosa.
• Microscopy: transmural neutrophil infiltration, mucosal ulceration, microabscesses.
Gangrenous appendicitis:
• Green-black discolouration, friable wall due to ischaemic necrosis.
• High risk of imminent perforation.
Complications (in order of frequency):
1. Perforation and generalised peritonitis — most feared; spillage of faecal flora.
2. Pericaecal/periappendiceal abscess — if omentum walls off the perforation.
3. Portal pyaemia — septic emboli via portal vein → hepatic abscesses (rare but life-threatening).
4. Pylephlebitis — suppurative thrombophlebitis of the portal vein branches.
5. Subphrenic abscess — if peritonitis tracks superiorly.
CLINICAL PEARL
Rovsing's sign, McBurney's point, rebound tenderness — all well-known clinically. The pathological correlate is peritoneal irritation from serosal inflammation. Once the appendix perforates, pain may paradoxically diminish briefly (pressure release) before intensifying as peritonitis generalises. Never be reassured by sudden pain relief in a child with appendicitis — it may signal perforation, not recovery.
SELF-CHECK
On histology of a surgically removed appendix, which finding is the minimum diagnostic criterion for acute appendicitis?
A. Neutrophils in the submucosal layer only
B. Neutrophil infiltration of the muscularis propria
C. Mucosal ulceration with goblet cell depletion
D. Fibrinous exudate on the serosa alone
Reveal Answer
Answer: B. Neutrophil infiltration of the muscularis propria
The diagnostic criterion for acute appendicitis on histology is neutrophil infiltration of the muscularis propria. Mucosal neutrophils can be found in other conditions (enteritis). Serosal fibrin alone is non-specific. The muscle layer involvement confirms transmural acute inflammation specific to appendicitis.
Inflammatory Bowel Disease — Overview and Crohn Disease
Crohn Disease: Gross and Microscopic Pathology
Inflammatory bowel disease (IBD) encompasses two chronic, relapsing immune-mediated disorders: Crohn disease (CD) and ulcerative colitis (UC). Both result from dysregulated mucosal immune responses to luminal antigens (gut microbiota) in genetically susceptible individuals.
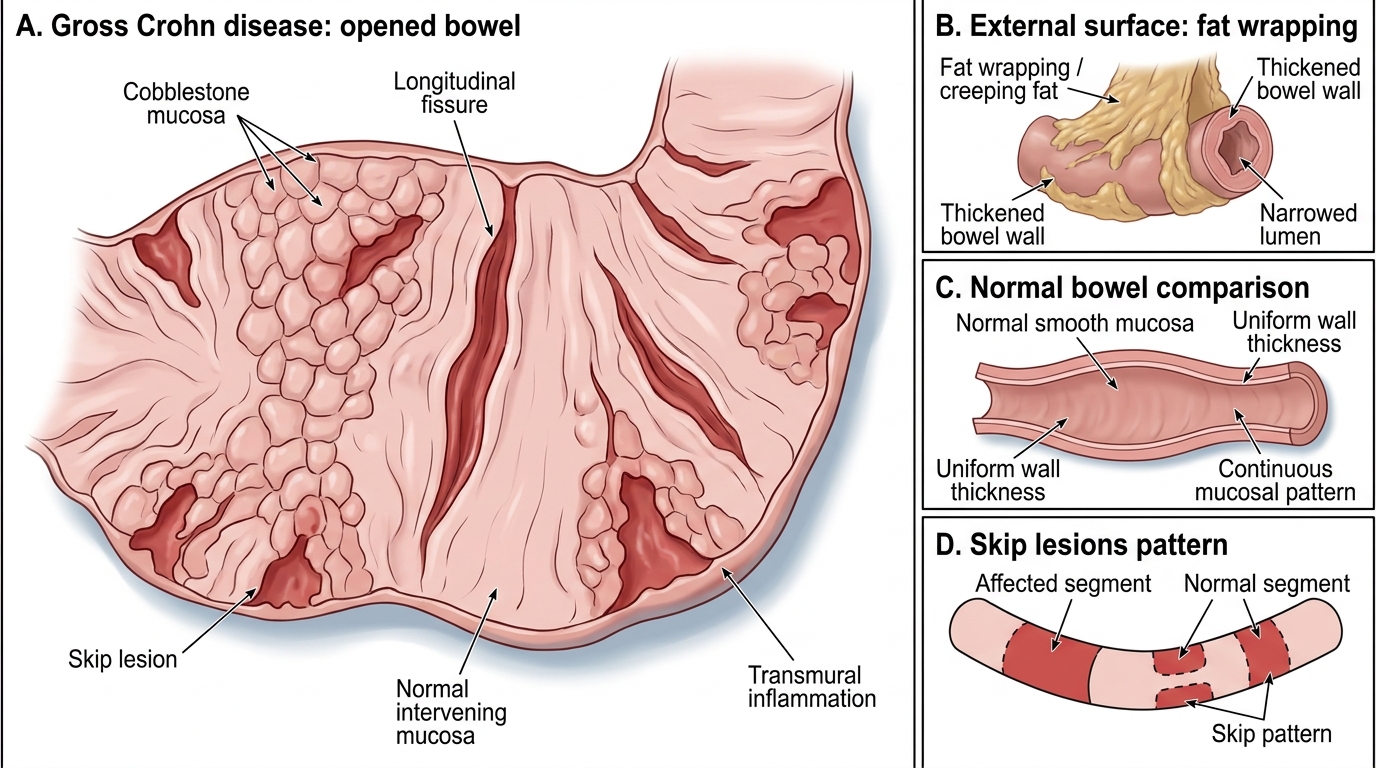
Crohn disease — key pathological features:
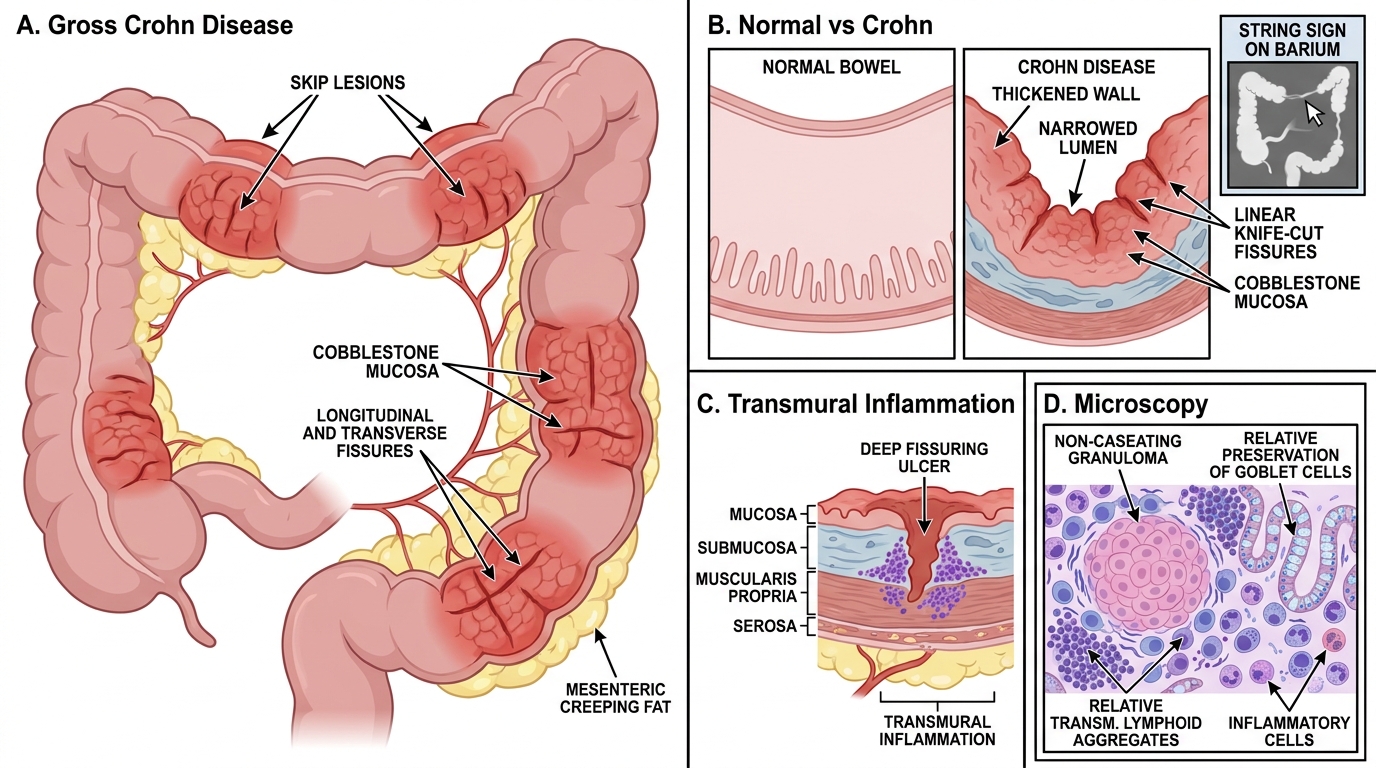
Distribution: Any segment from mouth to anus; most commonly terminal ileum and right colon (ileocolitis, 40%). Characterised by skip lesions — diseased segments separated by normal 'skip' areas.
Gross morphology:
• Cobblestone appearance — transverse fissures intersecting with longitudinal fissures between oedematous mucosa islands.
• Creeping fat (fat wrapping) — mesenteric fat extending over the serosal surface.
• Strictures — fibrous thickening of the wall → 'string sign' on barium.
• Fistulae — enteroenteric, enterocutaneous, perianal (hallmark of Crohn, very rare in UC).
• Linear 'knife-cut' fissures penetrating deep into the wall.
Microscopy:
• Transmural inflammation — all layers involved.
• Non-caseating granulomas in 50-60% of cases — the histological hallmark (absent in UC).
• Transmural lymphoid aggregates ('Crohn rosary').
• Fissuring ulcers extending into muscularis.
• Relative preservation of goblet cells.
Gross Pathology of Crohn Disease