Page 11 of 28
PA23.5-7 | Intestinal TB, Appendicitis, IBD & Malabsorption — SDL Guide (Part 3)
Ulcerative Colitis — Pathology and IBD Comparison
Ulcerative Colitis: Pathology and IBD Comparison
Ulcerative colitis (UC):
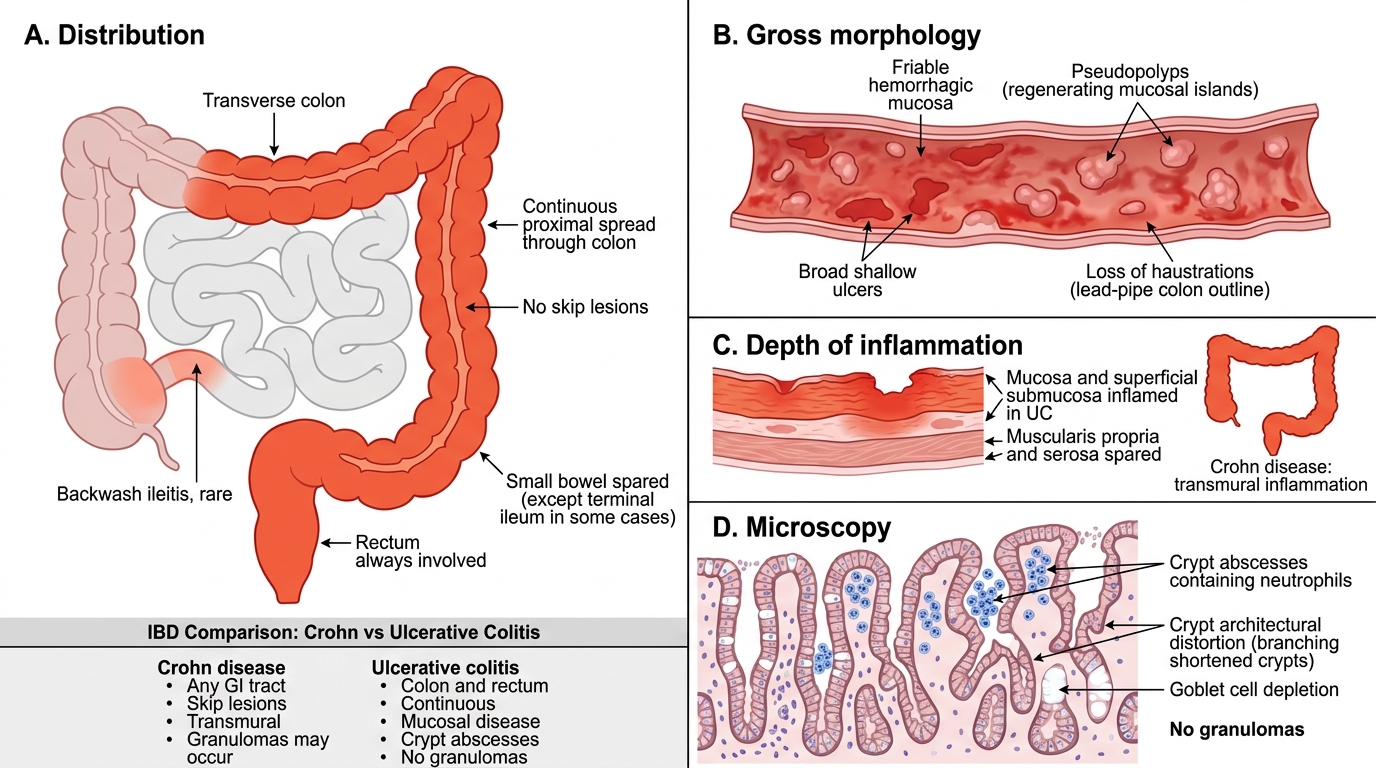
Distribution: Always involves the rectum (proctitis) and extends proximally in a continuous, uninterrupted pattern — never skip lesions. Limited to the colon and rectum (never small bowel, except 'backwash ileitis').
Gross morphology:
• Mucosal disease only (rarely submucosal) — no transmural involvement.
• Pseudopolyps (inflammatory polyps) — islands of regenerating mucosa surrounded by ulcerated areas; pathognomonic of UC.
• Lead-pipe colon on barium — loss of haustrations due to fibrosis and muscular hypertrophy (chronic disease).
• Friable, haemorrhagic mucosa with broad shallow ulcers.
Microscopy:
• Crypt abscesses — neutrophils within crypts, the histological hallmark of UC.
• Crypt architectural distortion — branching, shortened, irregular crypts (chronic change).
• Goblet cell depletion.
• No granulomas.
• Mucosal and submucosal inflammation only.
IBD Comparison Table — The High-Yield Summary:
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Distribution | Any GI, skip lesions | Colon/rectum, continuous |
| Depth | Transmural | Mucosal |
| Ulcers | Deep longitudinal fissures | Broad shallow |
| Microscopy hallmark | Non-caseating granulomas | Crypt abscesses |
| Fistulae | Very common | Rare (toxic megacolon risk) |
| Pseudopolyps | Occasional | Characteristic |
| Cancer risk | Small (small bowel > colon) | High (pancolitis >10 yr) |
| Surgery | Not curative | Colectomy = cure |
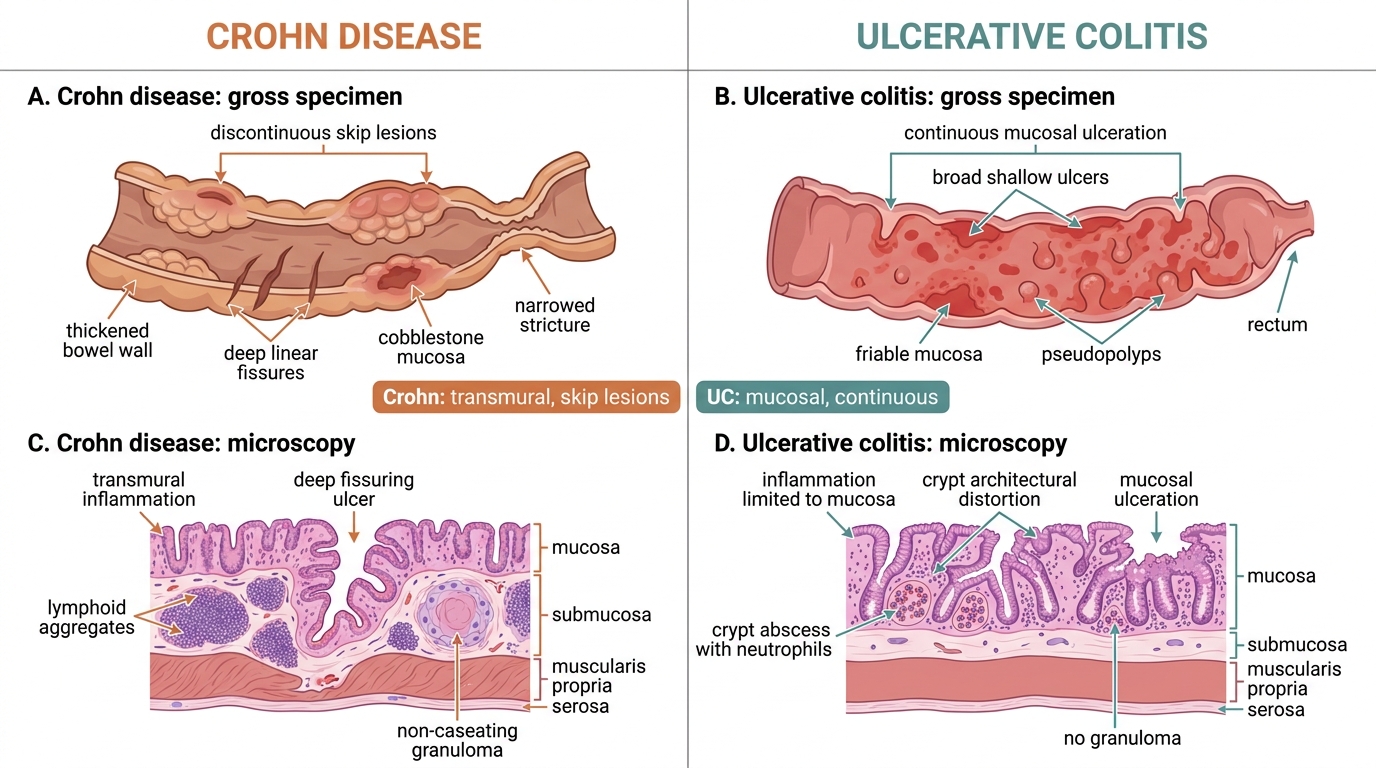
Crohn Disease vs Ulcerative Colitis: Gross and Microscopic Comparison
IBD — Complications and Extraintestinal Manifestations
⚑ AI image — pending faculty review (auto-QA score 9/10; best of 3 attempts)
IBD: Complications and Extraintestinal Manifestations
Complications of IBD:
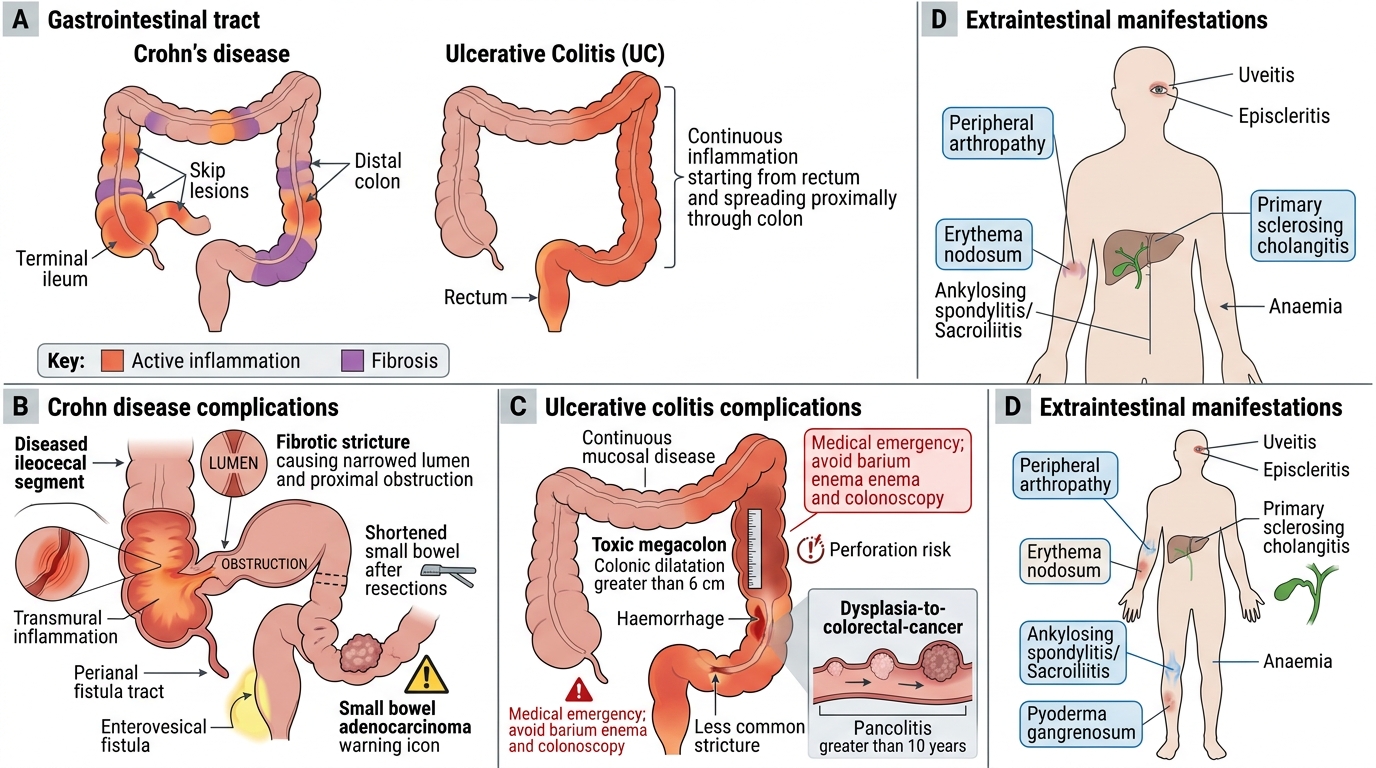
Crohn disease:
• Stricture and obstruction (fibrosis — 'fibrostenotic' phenotype).
• Fistulae — perianal fistulae, enterovesical, rectovaginal.
• Abscess formation.
• Short bowel syndrome after repeated surgical resections.
• Small bowel adenocarcinoma (rare but elevated risk vs general population).
Ulcerative colitis:
• Toxic megacolon — acute transmural inflammation → colonic dilatation > 6 cm → risk of perforation. Medical emergency. Barium enema and colonoscopy contraindicated.
• Colorectal cancer — risk rises steeply with pancolitis > 10 years (cumulative 10-20% at 20 years). Dysplasia surveillance colonoscopy is mandatory.
• Haemorrhage.
• Stricture (less common than Crohn).
Extraintestinal manifestations (shared by both, commoner in Crohn):
• Joints: peripheral arthropathy (parallels gut activity), ankylosing spondylitis/sacroiliitis (independent of activity).
• Skin: erythema nodosum (parallels gut activity), pyoderma gangrenosum (independent).
• Eyes: uveitis, episcleritis.
• Liver: primary sclerosing cholangitis (PSC) — strongly associated with UC (70% of PSC patients have UC); risk of cholangiocarcinoma.
• Blood: anaemia (iron/B12 deficiency or chronic disease).
SELF-CHECK
A 32-year-old presents with bloody diarrhoea for 8 weeks. Colonoscopy shows continuous mucosal erythema and friability from the rectum to the splenic flexure with multiple small pseudopolyps. Biopsy shows crypt abscesses and goblet cell depletion without granulomas. What is the most serious long-term complication to counsel this patient about?
A. Perianal fistula formation
B. Small bowel adenocarcinoma
C. Colorectal cancer with pancolitis duration
D. Primary biliary cirrhosis
Reveal Answer
Answer: C. Colorectal cancer with pancolitis duration
This is ulcerative colitis (continuous rectal disease, pseudopolyps, crypt abscesses, no granulomas). The most serious long-term complication is colorectal cancer, risk rising to 10-20% with pancolitis lasting >20 years, requiring regular dysplasia surveillance colonoscopy. Perianal fistulae are a feature of Crohn, not UC. PSC is associated with UC but is a hepatic complication, not the most serious intestinal complication. Primary biliary cirrhosis is not specifically associated with UC.
Malabsorption Syndrome — Causes and Pathophysiology
Malabsorption Syndrome: Causes and Pathophysiology
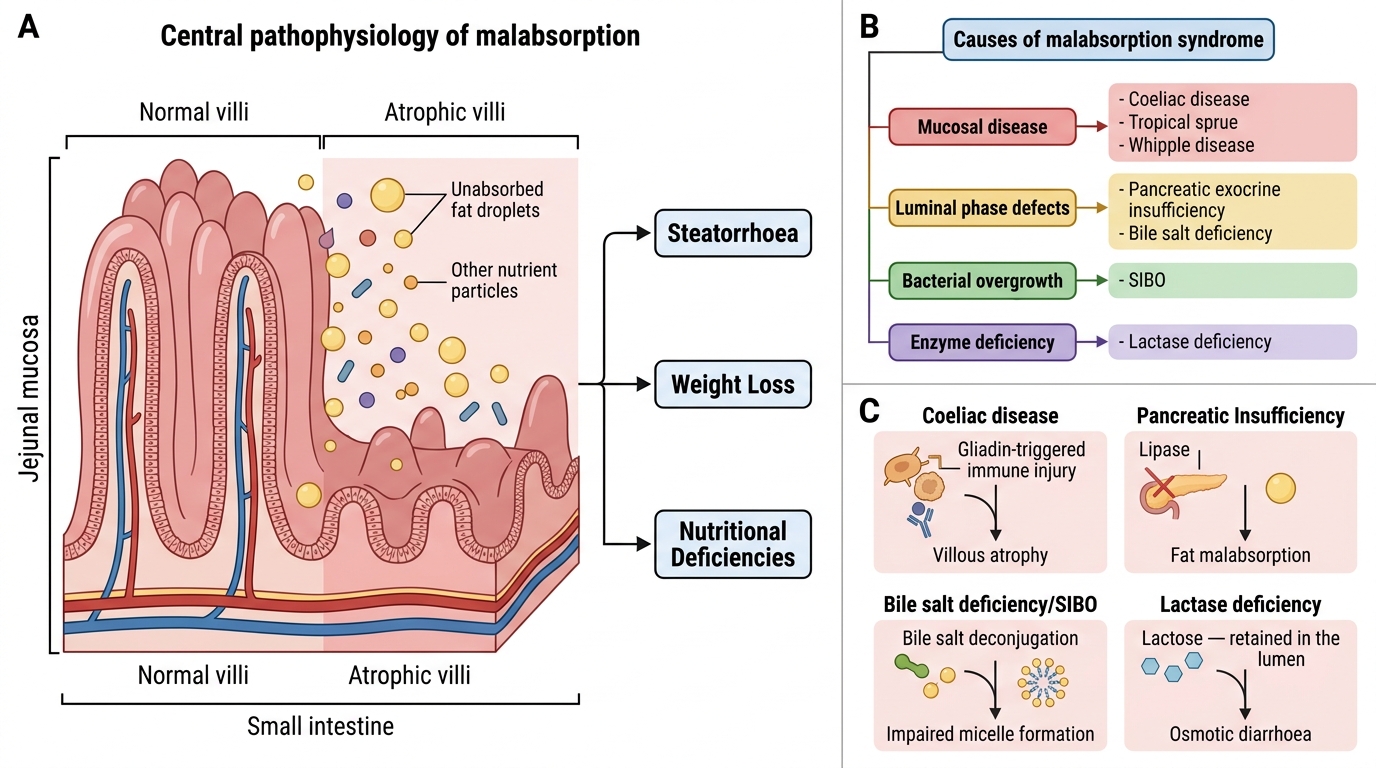
Malabsorption syndrome is defined as failure of the small intestine to absorb nutrients (fat, carbohydrates, proteins, vitamins, minerals) adequately. The cardinal clinical features are steatorrhoea (bulky, greasy, offensive stools), weight loss, and nutritional deficiencies.
Classification of causes:
Mucosal (absorptive surface) diseases:
• Coeliac disease (gluten-sensitive enteropathy) — immune-mediated villous atrophy triggered by gliadin (gluten component); anti-tissue transglutaminase (anti-tTG) and anti-endomysial antibodies; HLA-DQ2/DQ8 association.
• Tropical sprue — chronic malabsorption in tropical countries (India, SE Asia, Caribbean); likely infectious/bacterial cause; responds to tetracycline + folate.
• Whipple disease — rare; caused by Tropheryma whipplei; PAS-positive macrophages in lamina propria; systemic (arthritis, neurological).
Luminal phase defects:
• Pancreatic exocrine insufficiency — chronic pancreatitis, cystic fibrosis; deficient lipase → fat malabsorption.
• Bile salt deficiency — cholestatic liver disease, terminal ileum resection (bile salt reabsorption site), bacterial deconjugation.
Bacterial overgrowth:
• Small intestinal bacterial overgrowth (SIBO) — motility disorders, blind loops, strictures; bacteria deconjugate bile salts and consume nutrients.
Enzyme deficiency:
• Lactase deficiency — commonest worldwide; lactose malabsorption → osmotic diarrhoea; high prevalence in South Asians.
Structural reduction:
• Short bowel syndrome — after extensive surgical resection.