Page 12 of 28
PA23.5-7 | Intestinal TB, Appendicitis, IBD & Malabsorption — SDL Guide (Part 4)
Coeliac Disease — Pathology and India Context
Coeliac Disease: Pathology, Pathogenesis, and India Context
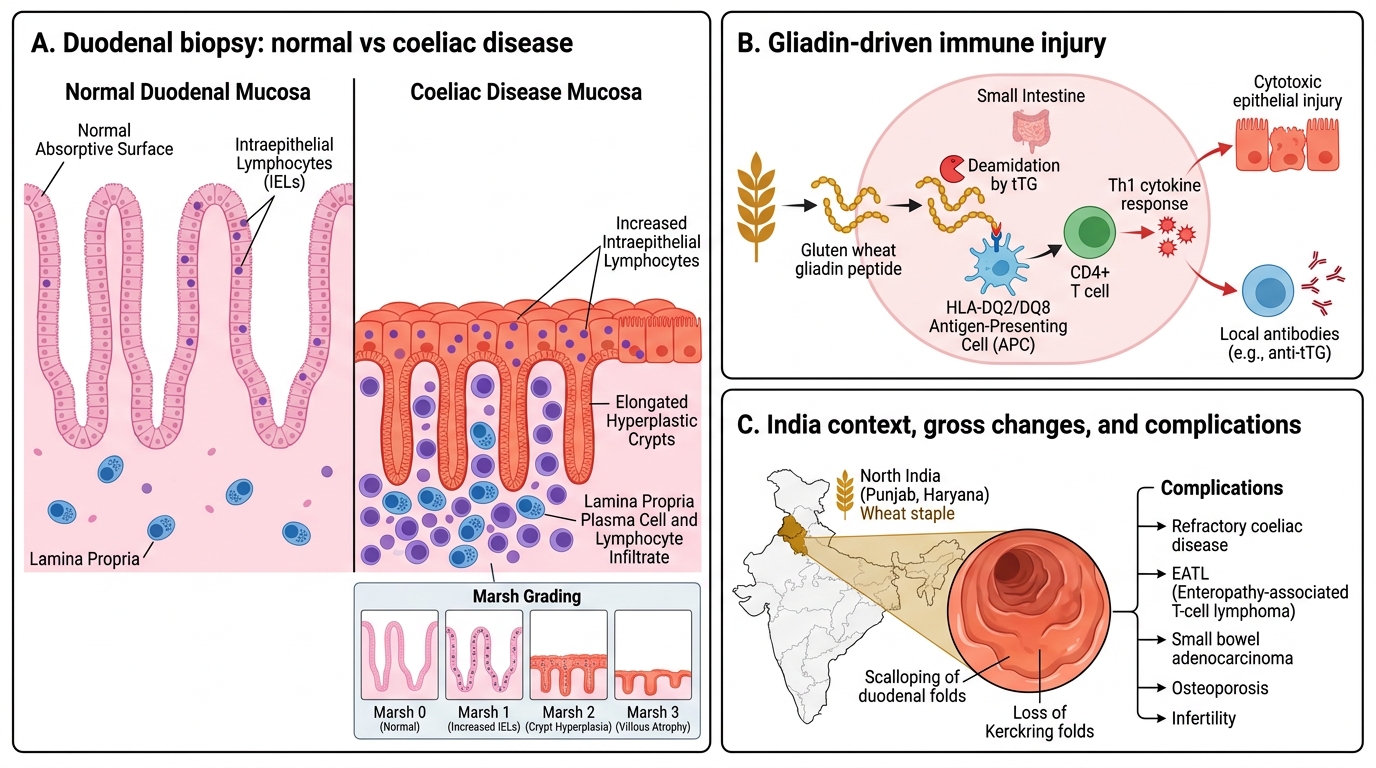
Coeliac disease deserves focused attention because its incidence in North India (Punjab, Haryana) rivals European rates — wheat is the dietary staple.
Pathogenesis: Dietary gliadin peptides are deamidated by tissue transglutaminase (tTG) → presented via HLA-DQ2/DQ8 to CD4+ T cells → Th1 response → villous destruction by cytotoxic T cells and local antibody production.
Biopsy findings — duodenum/proximal jejunum (Marsh classification):
• Villous atrophy — partial to total flattening of villi → loss of absorptive surface ('flat mucosa').
• Crypt hyperplasia — crypts elongate (compensatory proliferation).
• Intraepithelial lymphocytes (IELs) > 25 per 100 enterocytes — earliest, most sensitive change.
• Lamina propria plasma cell and lymphocyte infiltration.
Gross: Scalloping of duodenal folds on endoscopy; loss of Kerckring folds.
Response: Gluten-free diet → mucosal recovery within months.
Complications: Refractory coeliac disease, enteropathy-associated T-cell lymphoma (EATL) (rare but serious), small bowel adenocarcinoma, osteoporosis, infertility.
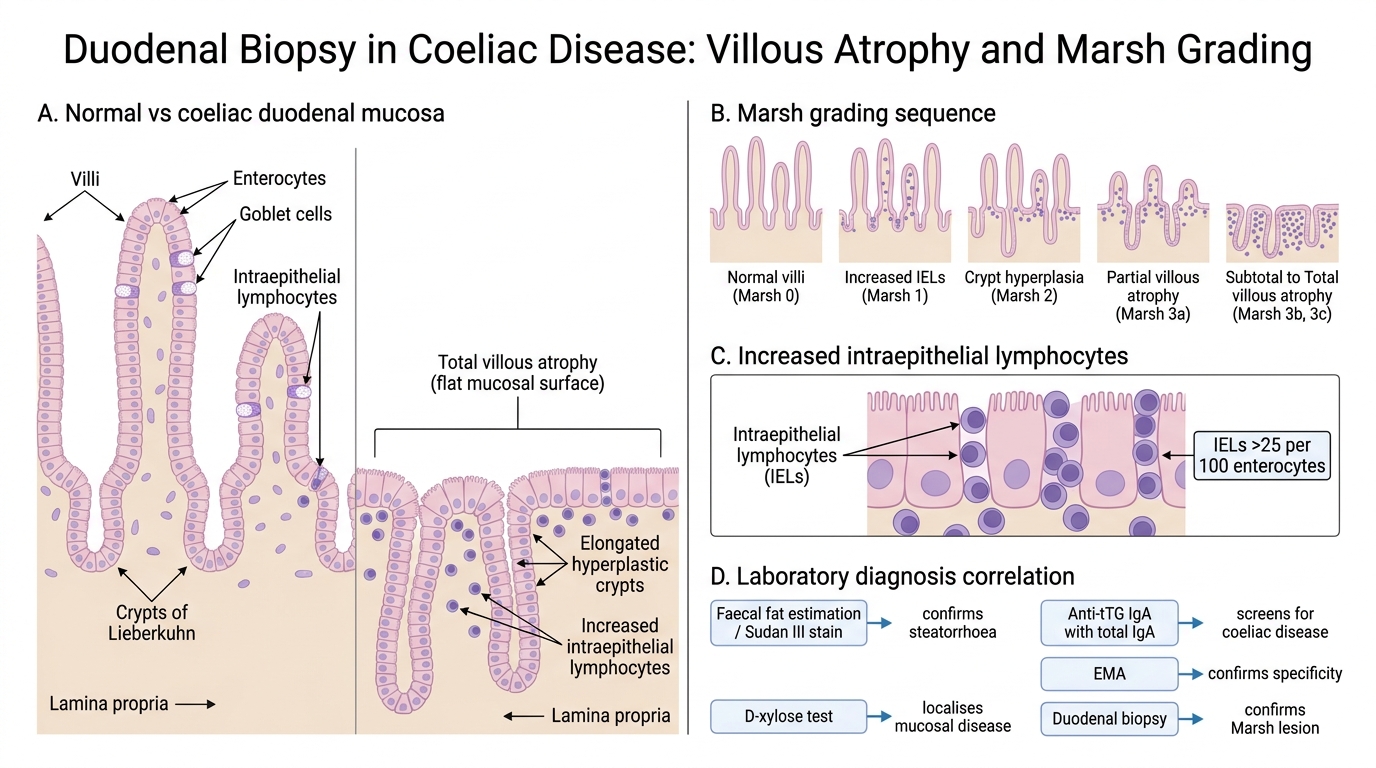
Coeliac Disease: Duodenal Biopsy and Marsh Grading
Malabsorption Syndrome — Laboratory Diagnosis
Laboratory Diagnosis of Malabsorption Syndrome
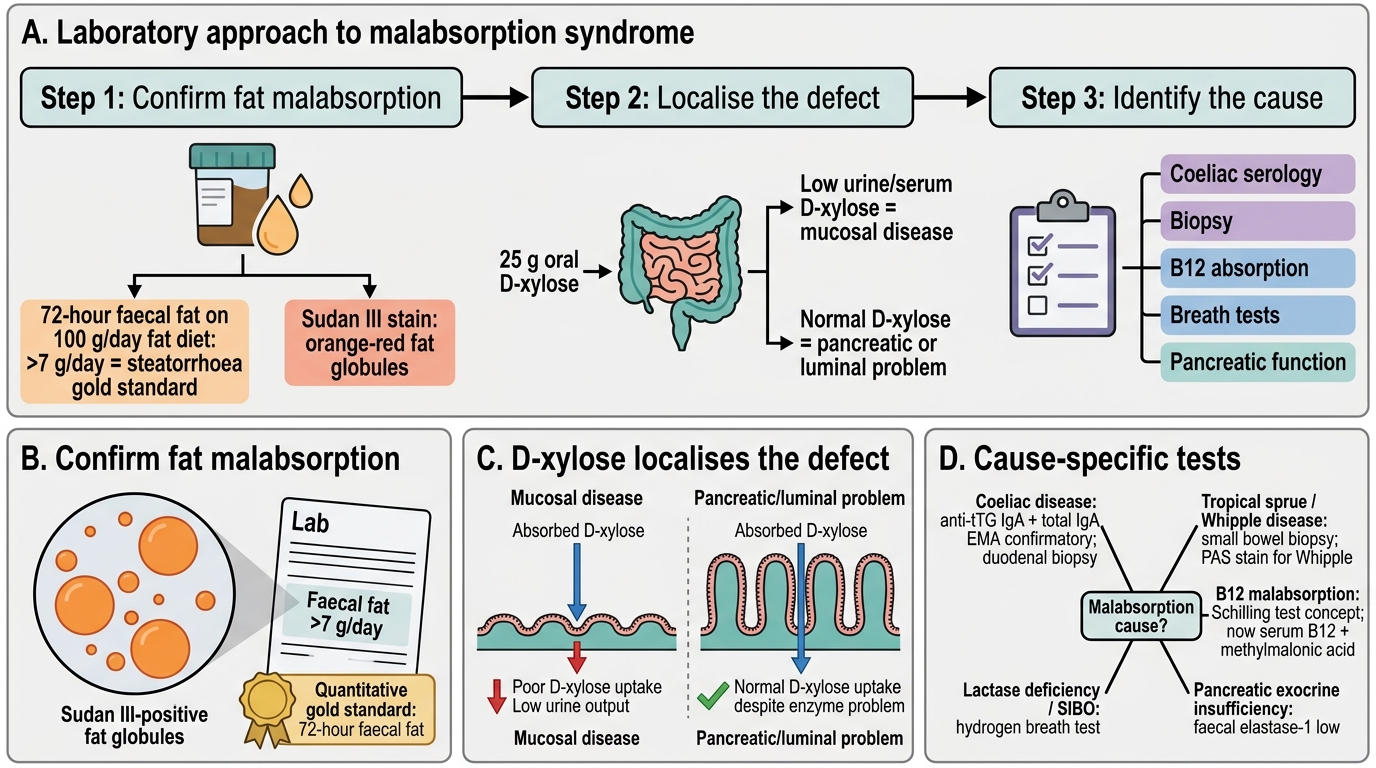
A systematic laboratory approach confirms malabsorption, localises it, and identifies the cause.
Step 1 — Confirm fat malabsorption:
• Faecal fat estimation (72-hour stool collection on 100 g/day fat diet) — >7 g/day = steatorrhoea; gold standard quantitative test.
• Sudan III stain of fresh stool — qualitative screen (fat globules).
Step 2 — Localise the defect (luminal vs mucosal):
• D-xylose absorption test — oral 25 g D-xylose → measure urine (5-hour) and/or serum (1-hour) levels.
- Low D-xylose → mucosal disease (coeliac, tropical sprue) — xylose requires mucosal transport.
- Normal D-xylose → pancreatic insufficiency or luminal problem (xylose absorbed without pancreatic enzymes).
Step 3 — Identify specific cause:
• Anti-tTG IgA (and total IgA) — highly sensitive/specific for coeliac disease; first-line serological test.
• Anti-endomysial antibody (EMA) — high specificity, operator-dependent; confirmatory.
• Small bowel biopsy (duodenal/jejunal) — definitive for coeliac, tropical sprue, Whipple (PAS stain).
• Schilling test — tests B12 absorption at each step (intrinsic factor, ileal mucosa, bacterial overgrowth); now largely replaced by serum B12 + methylmalonic acid but still asked in exams.
• Hydrogen breath test — lactase deficiency (lactose challenge), SIBO (glucose challenge).
• Faecal elastase-1 — screen for pancreatic exocrine insufficiency (low in chronic pancreatitis).
• Endoscopy + biopsy — gold standard for mucosal causes.
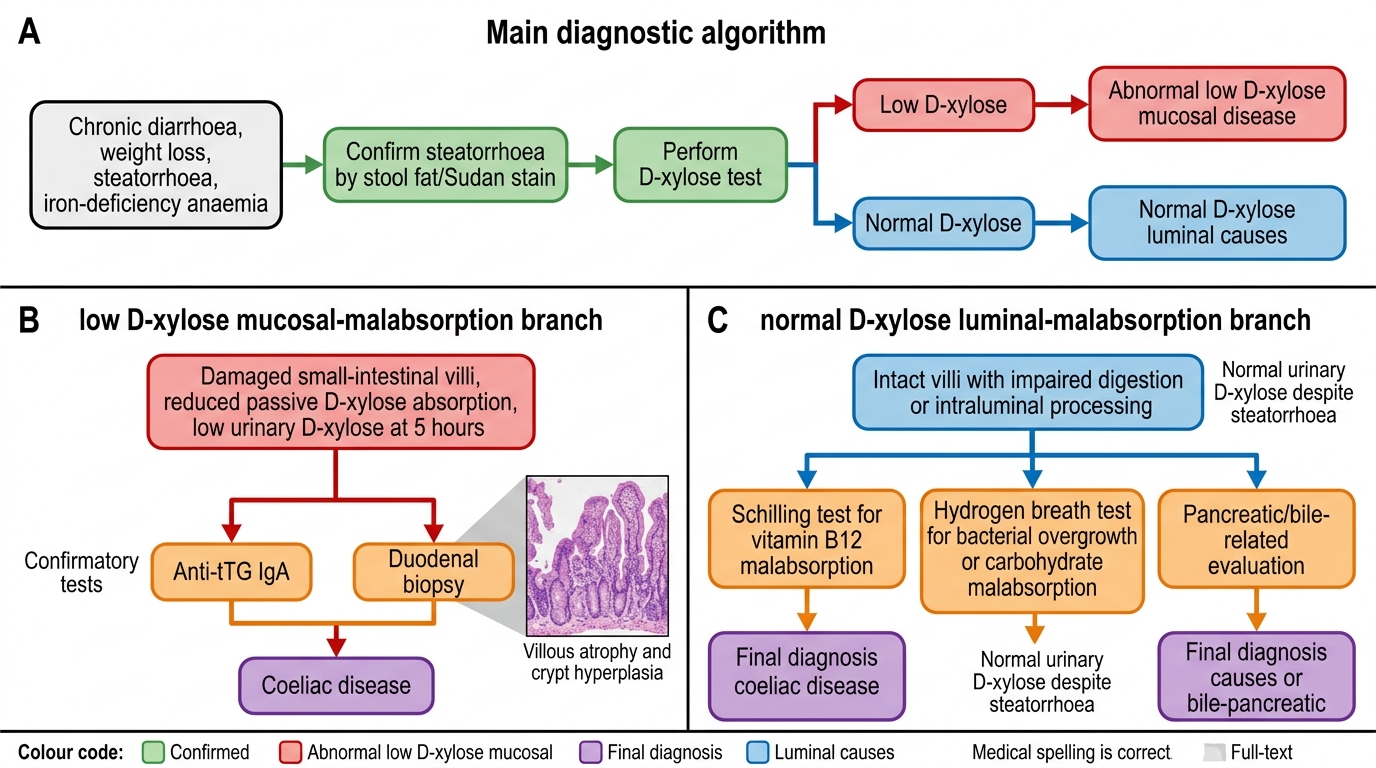
Laboratory Work-up of Malabsorption Syndrome
SELF-CHECK
A 19-year-old presents with steatorrhoea and iron-deficiency anaemia. Serum anti-tTG IgA is markedly elevated. D-xylose test shows low urinary excretion at 5 hours. Duodenal biopsy shows total villous atrophy with crypt hyperplasia. Which statement best explains why D-xylose excretion is low in this patient?
A. D-xylose requires pancreatic lipase for absorption
B. D-xylose requires bile salt micelles for uptake
C. D-xylose is metabolised before reaching the kidney
D. D-xylose is absorbed passively by intestinal mucosa, which is destroyed in coeliac disease
Reveal Answer
Answer: D. D-xylose is absorbed passively by intestinal mucosa, which is destroyed in coeliac disease
D-xylose is a pentose sugar absorbed passively by the intestinal mucosa without requiring pancreatic enzymes or bile salts. In coeliac disease, villous atrophy destroys the absorptive mucosa, directly reducing D-xylose uptake and urinary excretion. This contrasts with pancreatic insufficiency, where the mucosa is intact and D-xylose absorption is normal or near-normal, making the D-xylose test the key discriminator between mucosal and luminal causes of malabsorption.
CLINICAL PEARL
The India malabsorption differential: When you see a young adult from a tropical region with chronic diarrhoea, steatorrhoea, and folate/B12 deficiency, consider tropical sprue before coeliac disease — especially if anti-tTG is negative. Tropical sprue responds dramatically to tetracycline + folic acid supplementation for 3-6 months. Missing it means unnecessary gluten-free diet counselling and delayed cure.