Page 1 of 28
PA23.1-2 | Oral & Oesophageal Cancers — SDL Guide
Learning Objectives
- Enumerate the risk factors for oral squamous cell carcinoma with emphasis on India-specific exposures (tobacco, gutka, betel/areca nut, alcohol)
- Describe the premalignant lesions of the oral cavity — leukoplakia, erythroplakia, and oral submucous fibrosis — and their malignant transformation risk
- Explain the gross and microscopic features of oral SCC, including keratin pearl formation and histological grading
- Compare the epidemiology, aetiology, and pathological features of oesophageal SCC versus adenocarcinoma
- Outline the Barrett oesophagus metaplasia → dysplasia → adenocarcinoma sequence
- Describe the clinical presentation, routes of spread, and prognostic determinants of oesophageal carcinoma
INSTRUCTIONS
Oral and oesophageal cancers together account for a substantial burden of cancer morbidity in South Asia. India has the highest incidence of oral cancer in the world — tobacco chewing, gutka, and betel/areca nut are far more relevant exposures than in Western curricula. Oesophageal cancer presents late and carries a grim prognosis; understanding the two histological subtypes and the Barrett sequence is essential for clinico-pathological reasoning. This module builds directly on your Year-1 histology of stratified squamous epithelium and columnar epithelium, and maps to NMC competencies PA23.1 and PA23.2.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 17 (Oral Cavity) & Ch 16 (Gastrointestinal Tract — Oesophagus) (textbook)
- Harsh Mohan — Textbook of Pathology, 8th ed., Ch 18 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
India carries the world's highest burden of oral cancer — nearly one-third of all global cases. A 38-year-old construction worker walks in with a non-healing ulcer on the lateral border of his tongue. He has been chewing gutka twice daily since age 20. His mouth barely opens two fingers wide. What do his habits, the restricted opening, and the ulcer together tell you? By the time you finish this module, you will be able to name each step from mucosal irritation to invasive carcinoma — and understand why his prognosis depends on how long he waited to seek care.
WHY THIS MATTERS
Oral cancer is the most common cancer in Indian men. Tobacco in all its smokeless forms — gutka, pan masala, and khaini — contains potent carcinogens (tobacco-specific nitrosamines, polycyclic aromatic hydrocarbons). Combined with areca nut (a Group 1 carcinogen in its own right) and alcohol, these create a synergistic carcinogenic environment unique to South Asia. Recognising premalignant lesions in a primary care or outpatient setting is a directly examinable and clinically impactful skill — early detection reduces mortality by over 50 %.
RECALL
Before proceeding, bring to mind:
• The layers of stratified squamous non-keratinised epithelium (from Year-1 histology) — which layer do dysplastic changes begin in?
• The concept of metaplasia — a reversible change of one differentiated cell type to another, usually as an adaptive response to chronic injury.
• What is a dysplasia? How does it differ from carcinoma in situ?
• The oesophageal mucosa is normally stratified squamous in its upper two-thirds. What epithelium lines the stomach? (This transition matters for Barrett oesophagus.)
If any of these feel uncertain, spend two minutes reviewing the relevant Year-1 notes before continuing.
Risk Factors for Oral Cancer
Risk Factors for Oral Cancer
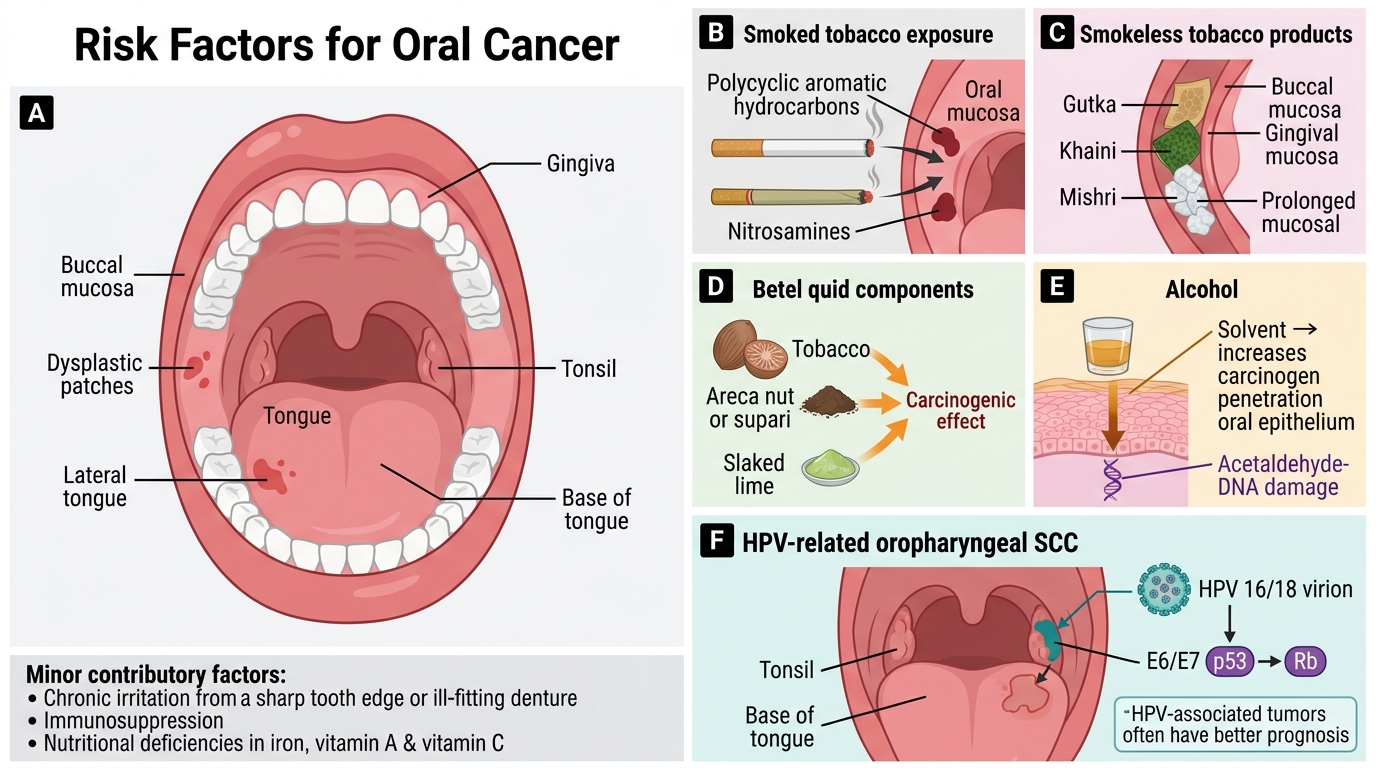
Oral cancer is not one disease but a spectrum driven by overlapping carcinogens.
Tobacco is the dominant risk factor worldwide. Smoked tobacco (cigarettes, bidi — highly prevalent in rural India) exposes the mucosa to polycyclic aromatic hydrocarbons and nitrosamines. Smokeless tobacco — gutka, khaini, mishri — is particularly insidious because contact with buccal and gingival mucosa is prolonged, and it is widely used by adolescents and women in India.
Areca nut (supari), with or without tobacco, is classified by IARC as a Group 1 carcinogen. Arecoline stimulates fibroblasts and causes oral submucous fibrosis (see next section). Combined exposure to areca nut + tobacco + slaked lime in betel quid (paan) is synergistically more carcinogenic than any single component.
Alcohol acts as a solvent enhancing mucosal penetration of carcinogens; it is also a direct carcinogen via acetaldehyde. The alcohol–tobacco combination multiplies risk multiplicatively, not just additively.
HPV (especially types 16 and 18) is increasingly implicated in oropharyngeal SCC (tonsil, base of tongue) in younger, non-smoking patients. HPV-associated tumours have a better prognosis (E6/E7 proteins disrupt p53 and Rb; wild-type p53 is retained in some, making them responsive to treatment).
Chronic irritation — ill-fitting dentures, sharp tooth edges — contributes locally but is rarely sufficient alone.
Immunosuppression and nutritional deficiencies (iron, vitamins A and C) lower mucosal repair capacity.
Premalignant Lesions of the Oral Cavity
Premalignant Lesions of the Oral Cavity
Three lesions demand recognition because they precede invasive cancer and are targets for early intervention.
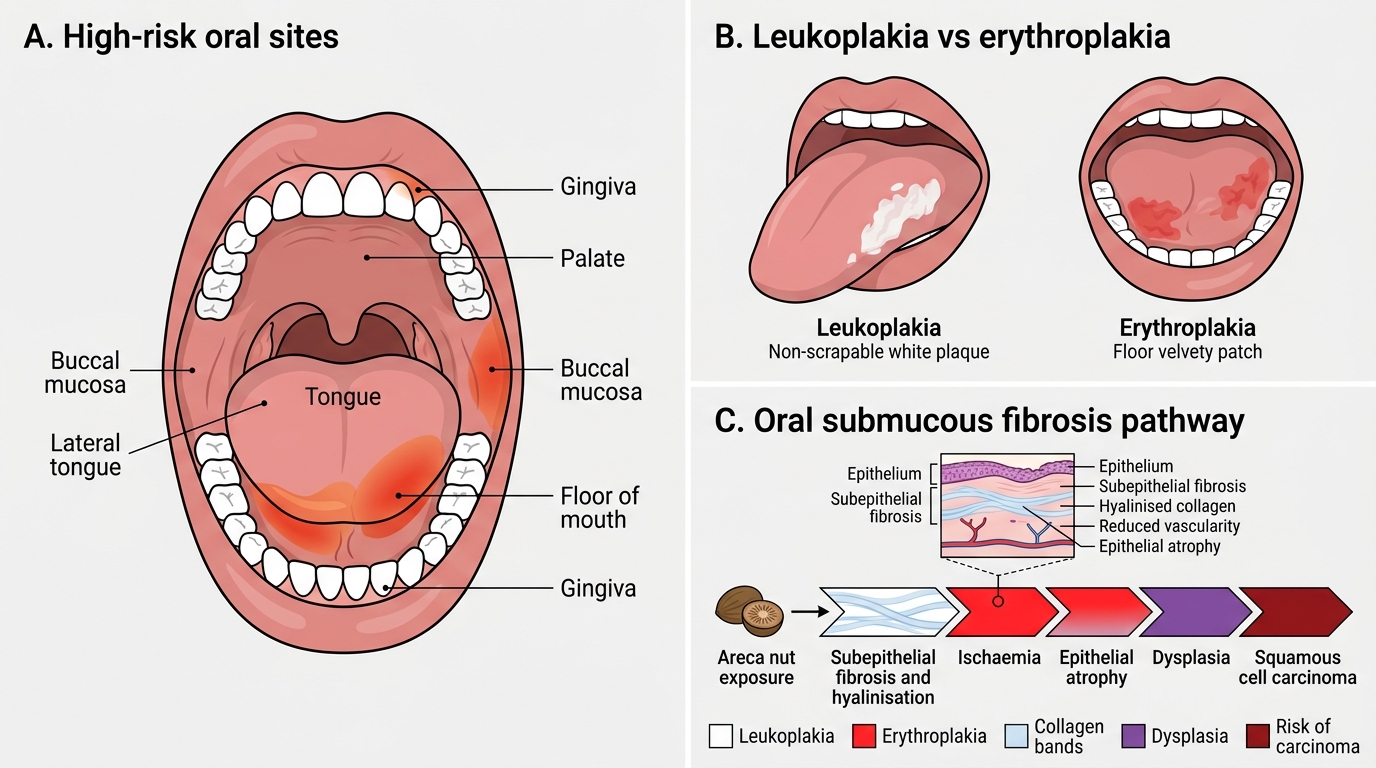
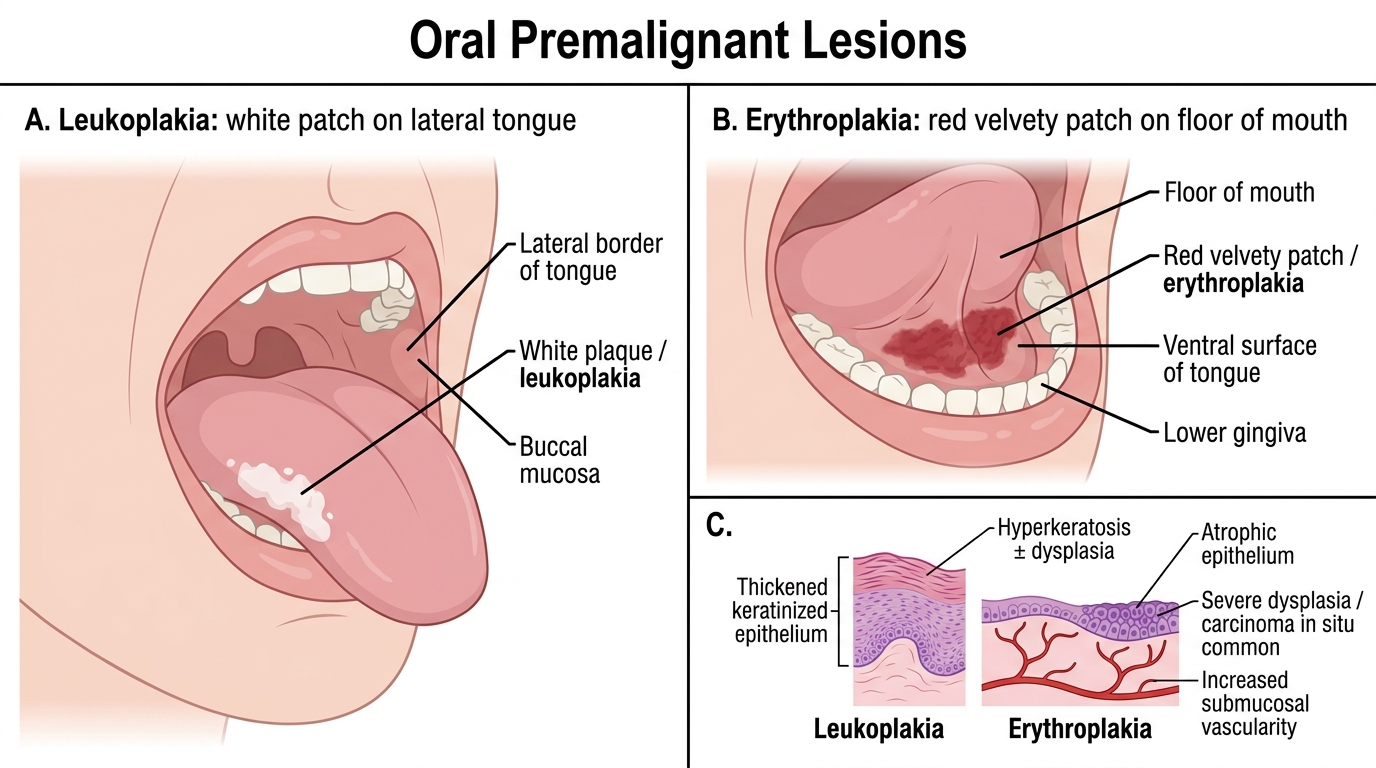
Leukoplakia is defined clinically as a white patch on oral mucosa that cannot be scraped off and cannot be attributed to any other known cause. It is a clinical term, not a histological diagnosis. Histologically, it may show hyperkeratosis without dysplasia (low risk, ~5 % transform) or epithelial dysplasia (moderate-to-high risk, up to 30 % transform). The floor of mouth and ventral tongue are high-risk sites.
Oral Premalignant Lesions: Leukoplakia vs Erythroplakia
Erythroplakia is a red velvety patch — it is far less common than leukoplakia but far more dangerous. Biopsy shows severe dysplasia or carcinoma in situ in ~90 % of cases. The rich vascularity reflects atrophic epithelium with increased submucosal vascularity.
Oral submucous fibrosis (OSMF) is a chronic, progressive, India-specific premalignant condition caused by areca nut alkaloids (arecoline). Pathologically: subepithelial fibrosis with hyalinisation → ischaemia → epithelial atrophy and dysplasia. Clinically: burning sensation, intolerance to spices, and progressive trismus (restricted mouth opening, as in our hook patient). Malignant transformation rate: 7–13 %. OSMF is listed under PA23.1 and is highly examinable.
Field cancerisation concept: chronic carcinogen exposure affects the entire oral mucosa simultaneously, creating multiple independent foci of dysplasia. This explains why oral cancer patients frequently develop second primary tumours in the same field — mouth, oropharynx, larynx, oesophagus.
SELF-CHECK
A 45-year-old woman presents with a 2 cm red, velvety patch on the floor of her mouth. She chews betel quid daily. Biopsy is most likely to show:
A. Hyperkeratosis without dysplasia
B. Moderate chronic inflammation only
C. Severe dysplasia or carcinoma in situ
D. Granulomatous inflammation
Reveal Answer
Answer: C. Severe dysplasia or carcinoma in situ
Erythroplakia carries the highest malignant potential among premalignant oral lesions — biopsy reveals severe dysplasia or carcinoma in situ in ~90 % of cases. The red colour reflects atrophic, poorly keratinised epithelium with increased submucosal vascularity, in contrast to leukoplakia which is thickened and hyperkeratotic.
Oral Squamous Cell Carcinoma — Pathology
Oral Squamous Cell Carcinoma: Gross and Microscopic Pathology
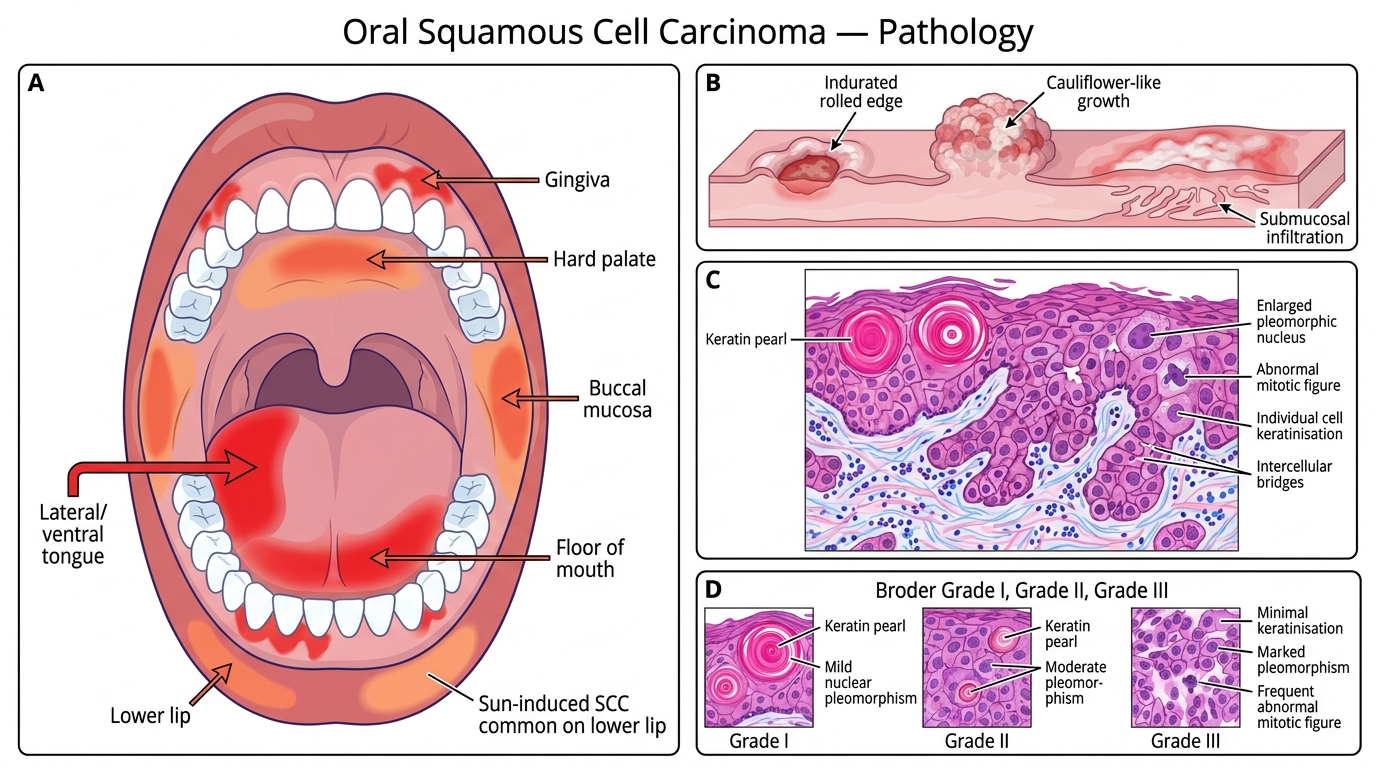
Over 90 % of oral cancers are squamous cell carcinoma (SCC). The sites in descending frequency are: lateral/ventral tongue > floor of mouth > gingiva > buccal mucosa > hard palate > lip (lower lip; lip SCC is largely sun-induced).
Gross features:
• Irregular ulcer with indurated (hardened, rolled) edges — the surrounding fibrosis gives firmness on palpation, distinguishing it from a benign aphthous ulcer
• Fungating/exophytic form: cauliflower-like growth
• Infiltrative form: flat, diffuse thickening with submucosal spread
Microscopic features:
Invasive nests and cords of malignant squamous cells breach the basement membrane and infiltrate submucosa, muscle, and bone. Key features:
• Keratin pearls (epithelial pearls): concentric whorls of squamous cells with central keratinisation — the hallmark of well-differentiated SCC
• Individual cell keratinisation: bright pink cytoplasm (eosinophilic)
• Intercellular bridges (desmosomes): visible between cells
• Nuclear pleomorphism, hyperchromasia, abnormal mitoses increase with dedifferentiation
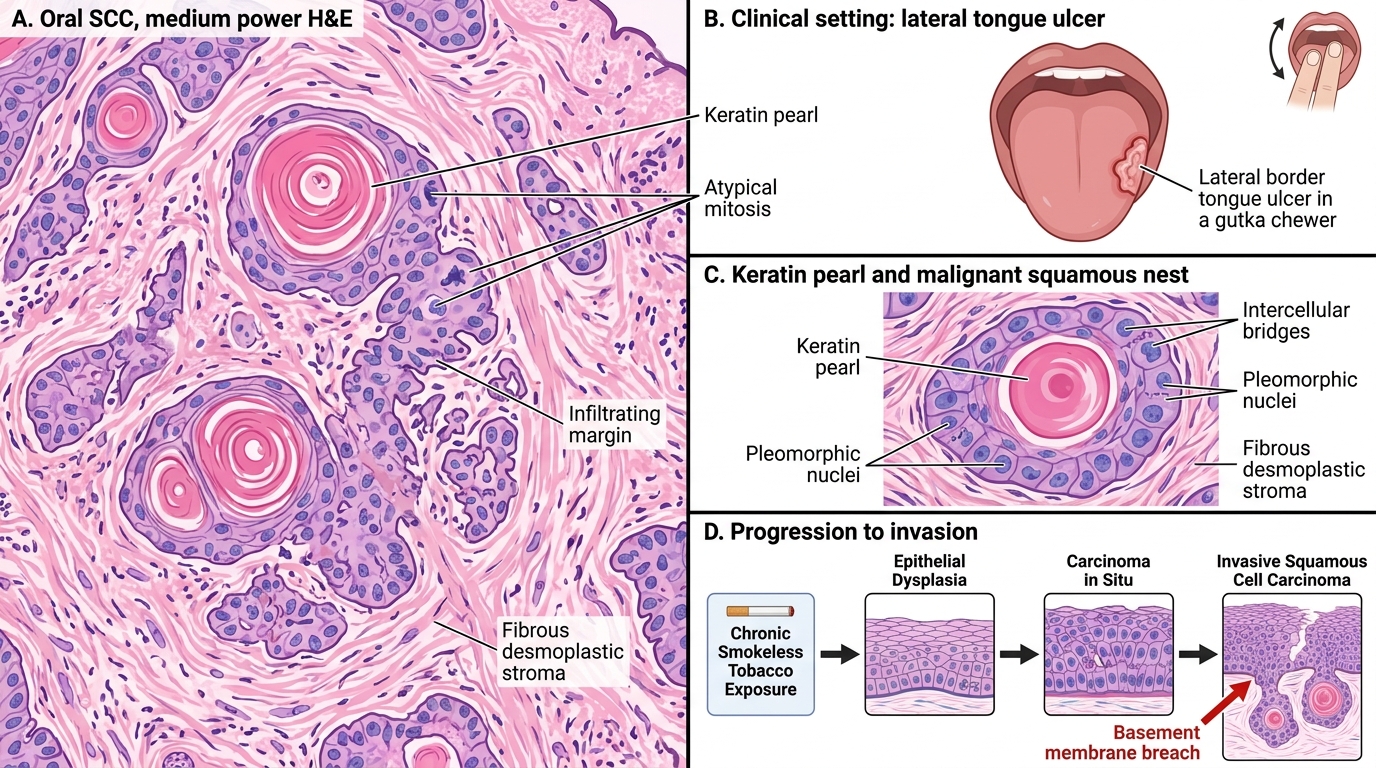
Oral Squamous Cell Carcinoma: Invasion and Keratin Pearls
Grading (Broder's system):
• Grade I (well-differentiated): abundant keratin pearls, mild pleomorphism
• Grade II (moderately differentiated): occasional pearls, moderate pleomorphism
• Grade III (poorly differentiated): rare/absent pearls, marked pleomorphism, high mitotic rate
Higher grade → worse prognosis, but stage (spread) outweighs grade prognostically.
Spread:
1. Local: tongue muscle, mandible/maxilla (bone invasion)
2. Lymphatic: to submandibular and deep cervical nodes (ipsilateral first, then bilateral)
3. Haematogenous: late; lung, liver, bone
Clinical features: non-healing ulcer >2–3 weeks (red flag), pain (often late), trismus (pterygoid/masseter invasion), cervical lymphadenopathy, dysphagia, weight loss.
CLINICAL PEARL
The Two-Week Rule for oral ulcers: any oral ulcer that has not healed within 2 weeks must be biopsied — no exceptions. Carcinoma can look exactly like a traumatic ulcer in early stages. The feature that distinguishes it on palpation is induration (hard, woody margins), whereas a benign ulcer is soft. In a tobacco/gutka user, the threshold for biopsy should be even lower. Remember: early T1/T2 oral SCC has a >80 % 5-year survival; T4 with nodal spread drops to <30 %.
SELF-CHECK
On histology of an oral SCC biopsy, you identify concentric whorls of squamous cells with central pink amorphous material. This finding is called:
A. Psammoma bodies
B. Keratin pearls
C. Mallory–Denk bodies
D. Call–Exner bodies
Reveal Answer
Answer: B. Keratin pearls
Keratin pearls (epithelial pearls) are the hallmark of well-differentiated SCC. They are concentric whorls of squamous cells progressively undergoing keratinisation toward the centre. Psammoma bodies are calcified concentric laminations seen in papillary thyroid carcinoma, meningioma, and serous ovarian tumours — not SCC.