Page 2 of 28
PA23.1-2 | Oral & Oesophageal Cancers — SDL Guide (Part 2)
Carcinoma Oesophagus — Overview and Types
Carcinoma Oesophagus: Overview and Types
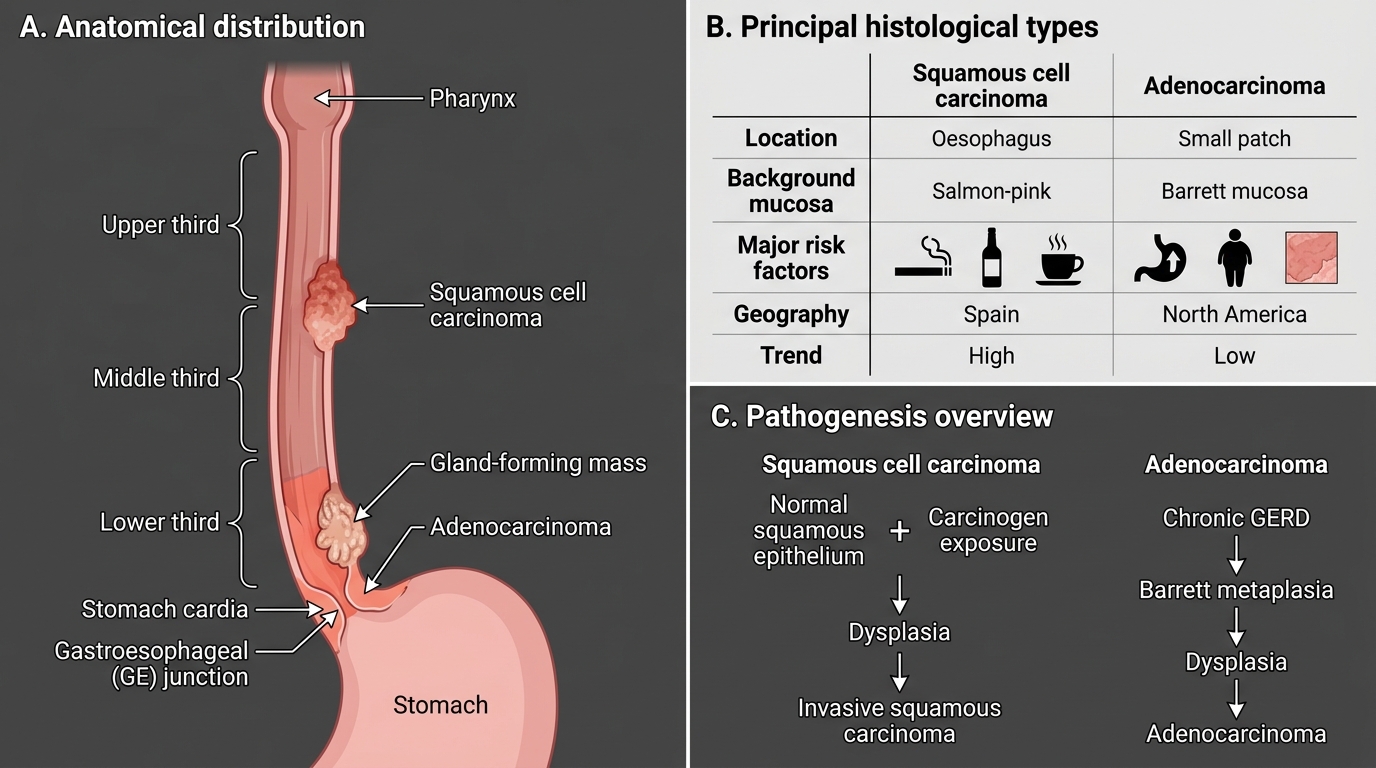
Oesophageal carcinoma has two principal histological types with distinct epidemiology, aetiology, location, and pathogenesis:
| Feature | Squamous Cell Carcinoma | Adenocarcinoma |
|---|---|---|
| Location | Upper/middle third | Lower third / GEJ |
| Background mucosa | Normal squamous | Barrett metaplasia |
| Risk factors | Tobacco, alcohol, hot beverages, achalasia, Plummer-Vinson, nitrosamines | Chronic GERD, obesity, Barrett oesophagus |
| Geography | Dominant type in India, China, Africa | Rising in Western countries |
| Trend | Stable/declining | Rapidly increasing in West |
Squamous cell carcinoma (SCC) accounts for the majority of oesophageal cancer globally and is the predominant type in India. Risk factors reflect the same mucosal carcinogen exposure as oral SCC:
• Tobacco and alcohol (synergistic, as in oral cavity)
• Hot beverages (tea/mate) — thermal injury to mucosa
• Achalasia — chronic stasis of food carcinogens
• Plummer-Vinson syndrome (iron-deficiency anaemia + dysphagia + oesophageal web + koilonychia) — mucosal atrophy predisposes; predominantly in women
• Dietary nitrosamines (preserved foods)
• Prior caustic stricture
Adenocarcinoma arises almost exclusively on a background of Barrett oesophagus (see next block). Its incidence has increased dramatically in Western countries over the last 40 years, paralleling the obesity and GERD epidemic.
Barrett Oesophagus — The Metaplasia–Dysplasia–Carcinoma Sequence
Barrett Oesophagus: Metaplasia-Dysplasia-Carcinoma Sequence
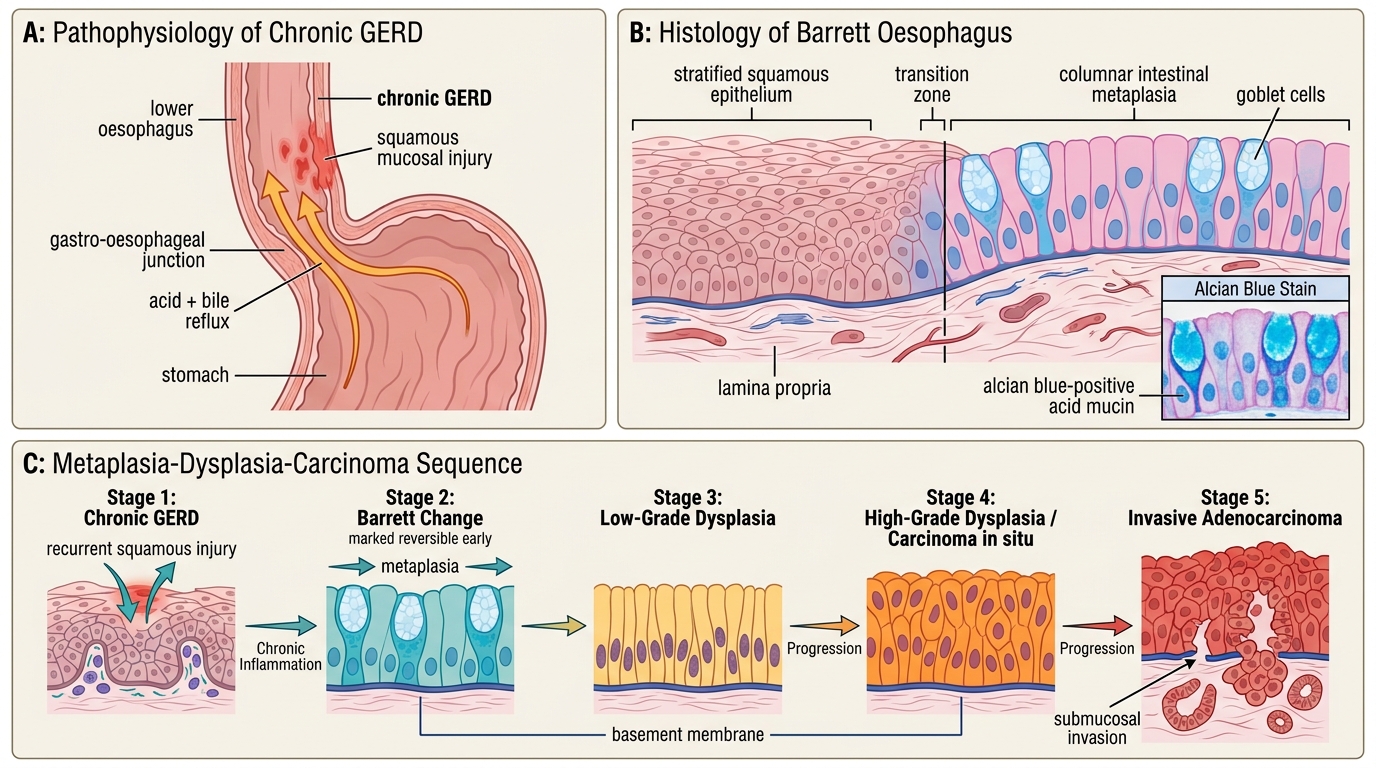
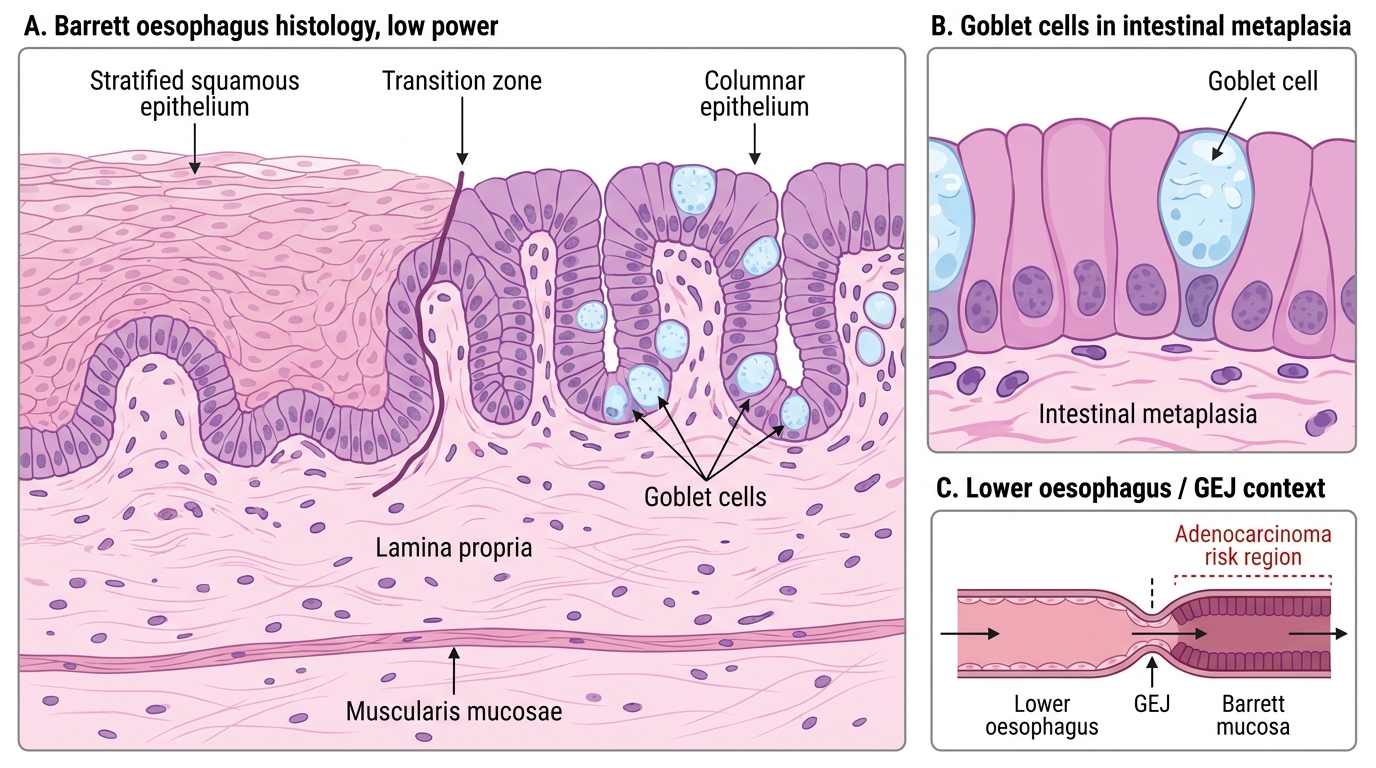
Barrett oesophagus is defined as the replacement of the normal stratified squamous epithelium of the lower oesophagus by specialised intestinal metaplasia — a columnar epithelium containing goblet cells. It is an adaptive response to chronic gastro-oesophageal reflux (GERD): acid + bile reflux chronically injures the squamous mucosa, and the regenerating stem cells differentiate into a more acid-tolerant columnar phenotype.
Barrett Oesophagus: Squamous-to-Columnar Transition
The sequence — must know each step:
1. Chronic GERD → recurrent squamous mucosal injury
2. Squamous → columnar intestinal metaplasia (Barrett change) — reversible in early stages
3. Metaplasia → low-grade dysplasia: nuclear crowding, hyperchromatism, loss of polarity confined to lower crypt
4. Low-grade → high-grade dysplasia (= carcinoma in situ): full-thickness dysplasia without invasion
5. High-grade dysplasia → invasive adenocarcinoma: basement membrane breach, submucosal invasion
Key points:
• Barrett is identified by goblet cells on biopsy (alcian blue stain highlights the acid mucin in goblet cells)
• Annual malignant transformation risk from Barrett without dysplasia: ~0.1–0.3 %/year; from high-grade dysplasia: ~6–10 %/year
• Barrett patients are enrolled in surveillance endoscopy programmes with biopsy every 1–2 years to catch high-grade dysplasia before invasion
• Obesity increases intra-abdominal pressure → GERD → Barrett → adenocarcinoma; this pathway explains the Western epidemic
SELF-CHECK
A 58-year-old man with a 15-year history of heartburn undergoes endoscopy. Biopsy of the lower oesophagus shows columnar epithelium with goblet cells. The MOST likely long-term complication if this lesion is not surveilled is:
A. Oesophageal squamous cell carcinoma
B. Oesophageal adenocarcinoma
C. Gastric MALT lymphoma
D. Achalasia cardia
Reveal Answer
Answer: B. Oesophageal adenocarcinoma
The biopsy description — columnar epithelium with goblet cells in the lower oesophagus — defines Barrett oesophagus (specialised intestinal metaplasia). Barrett is the established precursor of oesophageal adenocarcinoma (not SCC, which arises from normal squamous epithelium). Without surveillance, the metaplasia → dysplasia → adenocarcinoma sequence may go undetected until the tumour is advanced.
Oesophageal Carcinoma — Gross Patterns and Microscopy
Oesophageal Carcinoma: Gross Patterns and Microscopy
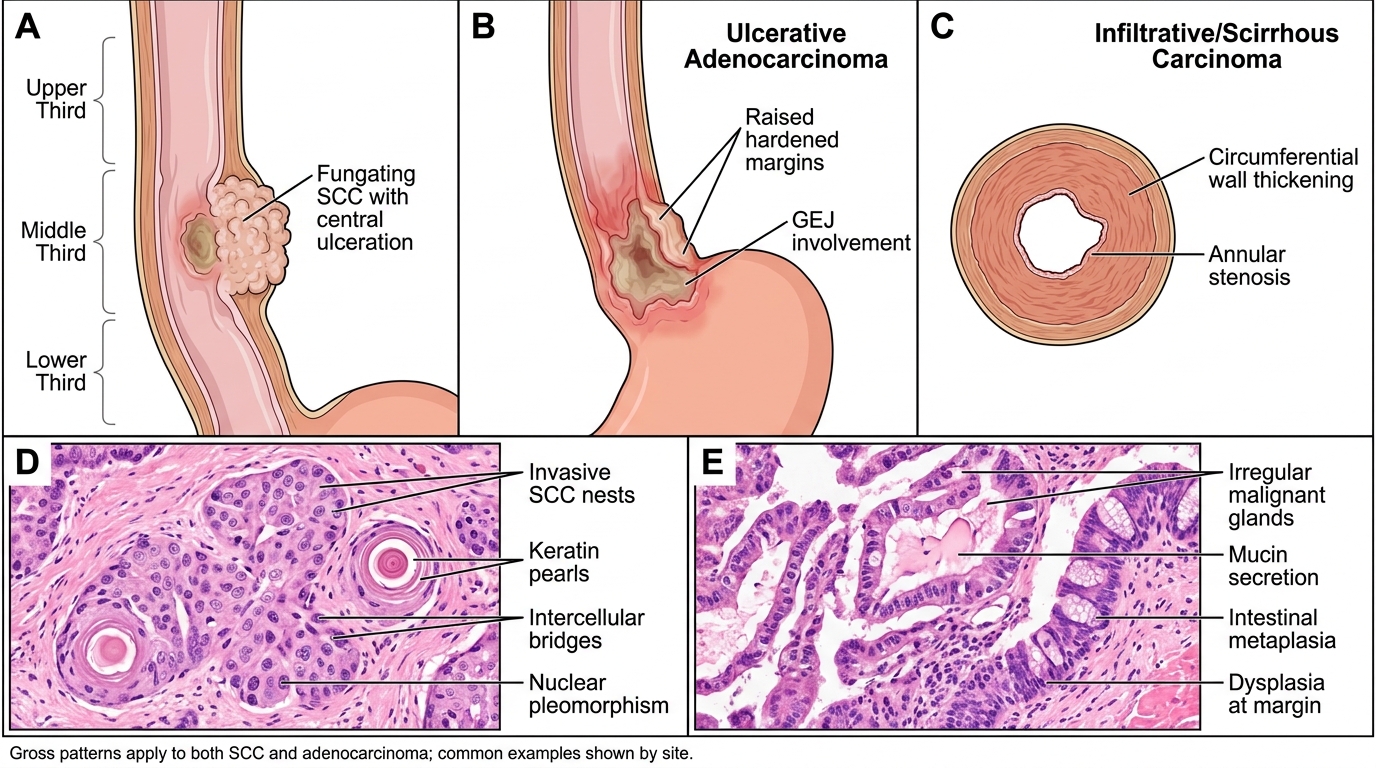
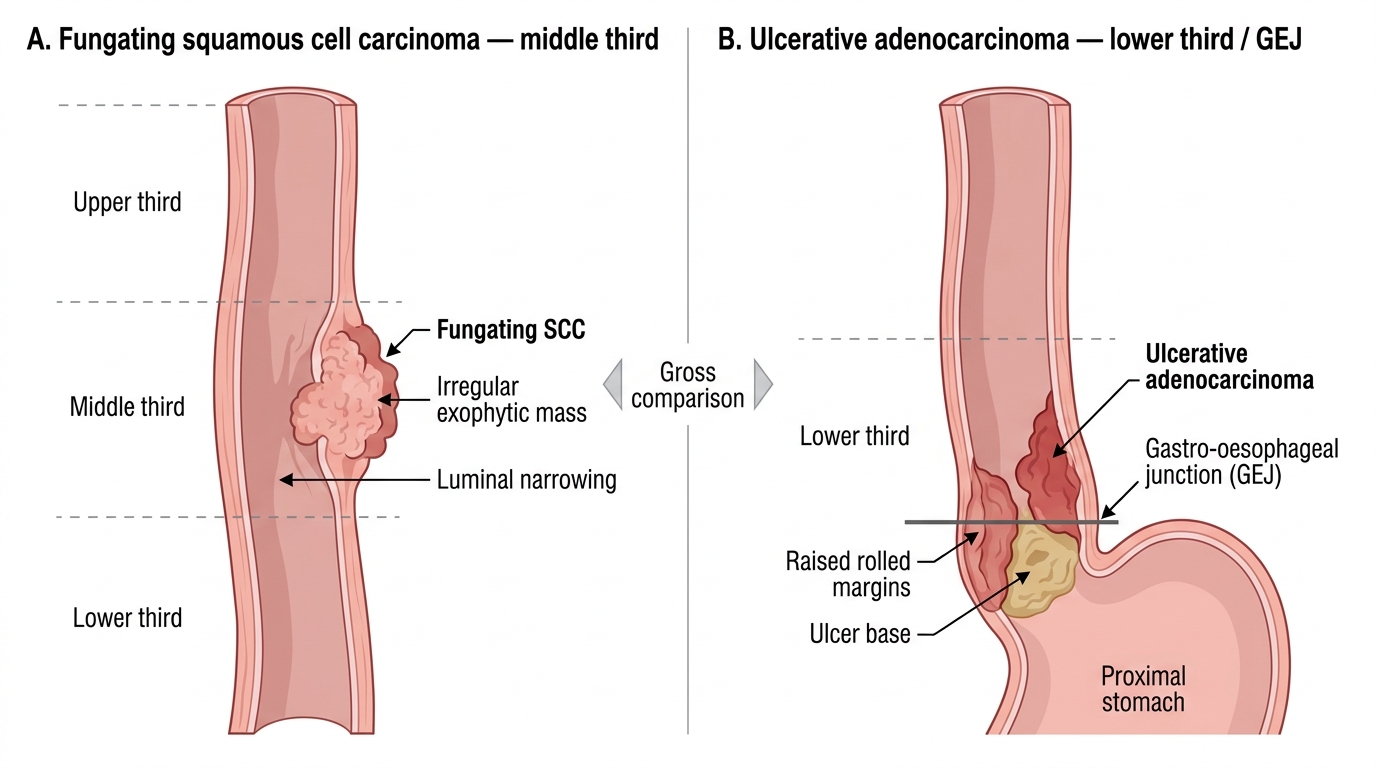
Gross patterns (apply to both SCC and adenocarcinoma):
• Fungating/polypoid: exophytic mass projecting into the lumen — may ulcerate at centre; most common pattern for SCC
• Ulcerative: flat ulcer with irregular edges, hardened margins; invades deeply
• Infiltrative/scirrhous: diffuse wall thickening without a discrete mass → linitis plastica-like stiffening; circumferential spread causes annular narrowing of the lumen
Gross Morphology of Oesophageal Carcinoma
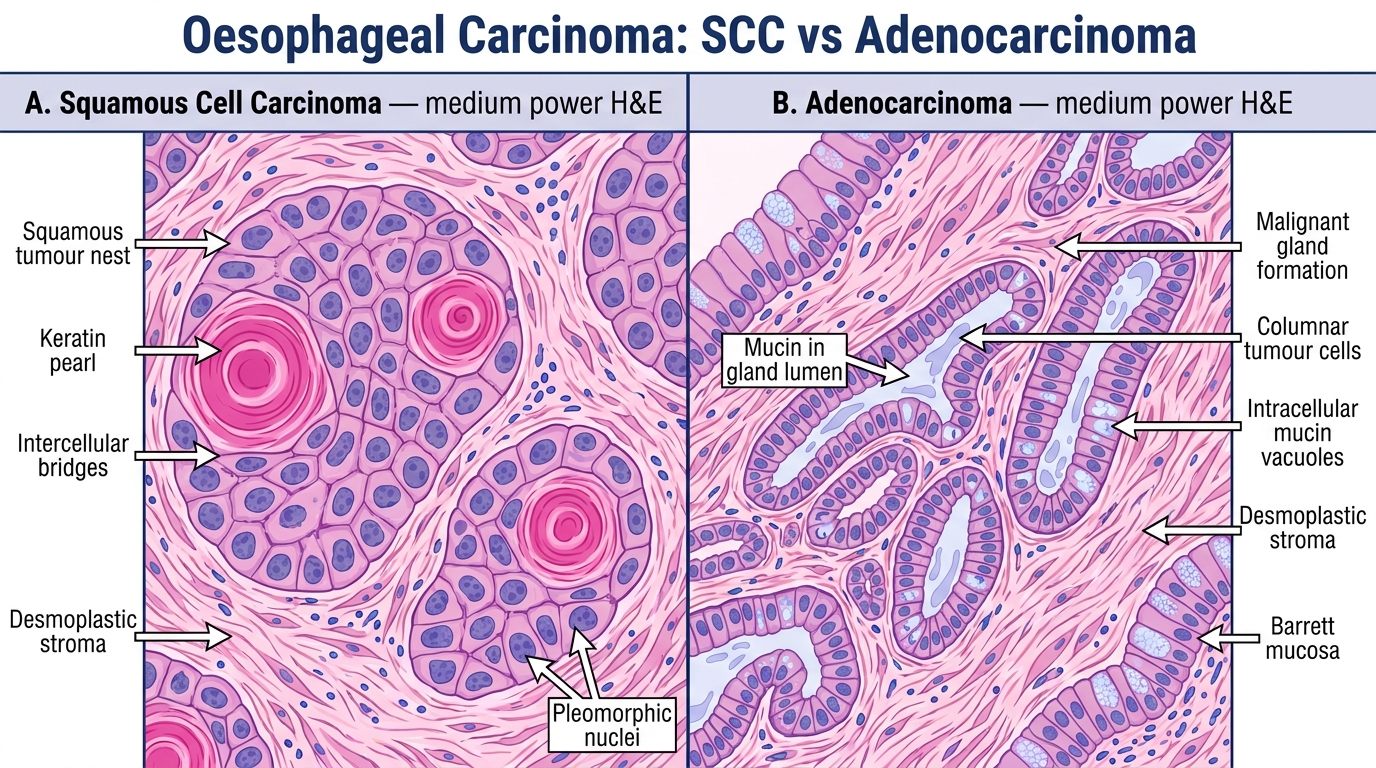
Microscopy of SCC: same as oral SCC — invasive nests of squamous cells, keratin pearls (well-diff), intercellular bridges, nuclear pleomorphism. Graded I–III as in oral SCC.
Microscopy of adenocarcinoma: gland-forming structures, mucin secretion, variable tubular/papillary/mucinous architecture, on a background of intestinal metaplasia and dysplasia at the margins.
Histology of Oesophageal SCC and Adenocarcinoma
Spread of oesophageal carcinoma:
• Intramural: longitudinal spread in the submucosal lymphatics — tumour extends well beyond visible margins (surgical implication: wide resection margins needed)
• Direct: trachea/bronchi (SCC), aorta, pericardium, recurrent laryngeal nerve (hoarseness)
• Lymphatic: cervical nodes (upper SCC), mediastinal nodes (mid SCC), coeliac/gastric nodes (lower third/adenocarcinoma)
• Haematogenous: liver, lung (late)