Page 3 of 28
PA23.1-2 | Oral & Oesophageal Cancers — SDL Guide (Part 3)
Clinical Features and Prognosis of Oesophageal Carcinoma
Clinical Features and Prognosis of Oesophageal Carcinoma
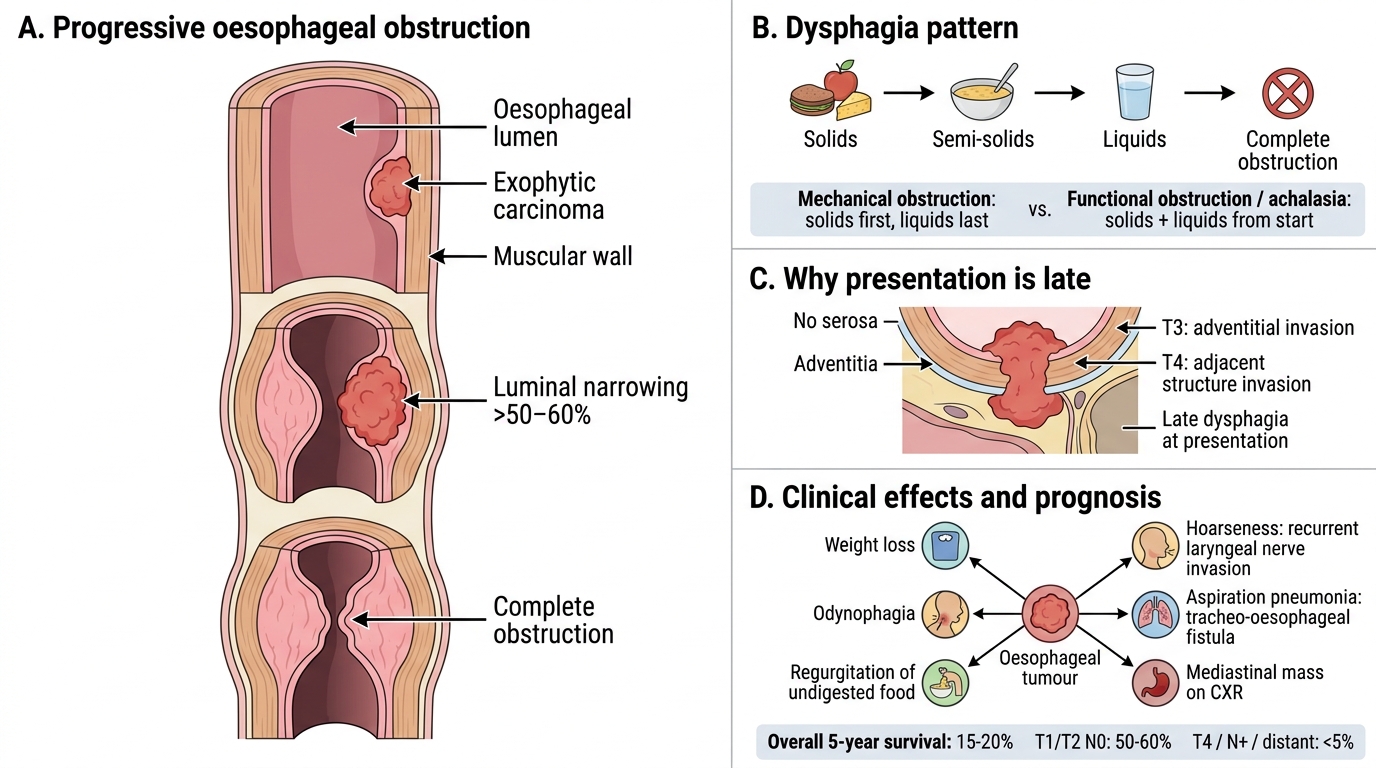
The cardinal symptom is progressive dysphagia — beginning with difficulty swallowing solids, progressing over weeks-to-months to difficulty with semi-solids, then liquids, and ultimately complete obstruction. This progressive pattern (solids first, liquids last) distinguishes mechanical obstruction (carcinoma, stricture) from functional obstruction (achalasia — dysphagia for solids AND liquids from the start).
Why does presentation come so late?
The oesophagus has no serosa. It can accommodate luminal encroachment until >50–60 % of the circumference is involved before dysphagia becomes manifest. By the time the patient presents with dysphagia, the tumour is usually T3 or T4 — hence the characteristically late stage at presentation.
Other clinical features:
• Odynophagia (painful swallowing)
• Weight loss — profound, multifactorial (mechanical obstruction + anorexia + tumour catabolism)
• Regurgitation of undigested food
• Hoarseness — recurrent laryngeal nerve invasion
• Aspiration pneumonia — tracheo-oesophageal fistula
• Haematemesis/malaena — ulceration into blood vessels
• Mediastinal mass on CXR
Prognosis is poor:
• Overall 5-year survival: ~15–20 %
• Stage at presentation is the dominant determinant — T1/T2 (submucosal/muscularis propria) with negative nodes: ~50–60 % 5-year survival; T4/N+ distant: <5 %
• Oesophageal SCC: slightly better surgical resectability than adenocarcinoma in some series
• Adenocarcinoma: if caught in Barrett surveillance at high-grade dysplasia stage → endoscopic resection with excellent outcomes
CLINICAL PEARL
Dysphagia red flags in practice: Progressive dysphagia in any patient >40 years is oesophageal carcinoma until proven otherwise — mandate urgent upper GI endoscopy and biopsy. Do not reassure and send home. The distinction between SCC and adenocarcinoma has therapeutic implications: SCC is more radiosensitive (relevant when surgical resection is not feasible); adenocarcinoma responds to trastuzumab if HER2-positive. In India, oesophageal SCC predominantly affects the mid-oesophagus; in the West, adenocarcinoma of the lower third dominates. Knowing this shapes your index of suspicion by geography.
SELF-CHECK
A 55-year-old man presents with a 3-month history of progressive dysphagia — initially to solids, now to semi-solids — along with 8 kg weight loss. He is a bidi smoker and consumes alcohol daily. Barium swallow shows an irregular 'rat-tail' narrowing in the mid-oesophagus. The MOST likely histological diagnosis is:
A. Squamous cell carcinoma
B. Adenocarcinoma with Barrett oesophagus
C. Carcinoid tumour
D. Leiomyosarcoma
Reveal Answer
Answer: A. Squamous cell carcinoma
Mid-oesophageal location + tobacco/alcohol exposure + Indian demographic profile = oesophageal SCC. Adenocarcinoma arises in the lower third on a Barrett (GERD) background and is the dominant type in obese Western patients. Carcinoid and leiomyosarcoma are rare oesophageal tumours and do not cause the progressive 'rat-tail' narrowing pattern.
Comparing Oral SCC and Oesophageal Carcinoma — Integrative Perspective
Oral SCC and Oesophageal Carcinoma: Shared Risks and Key Contrasts
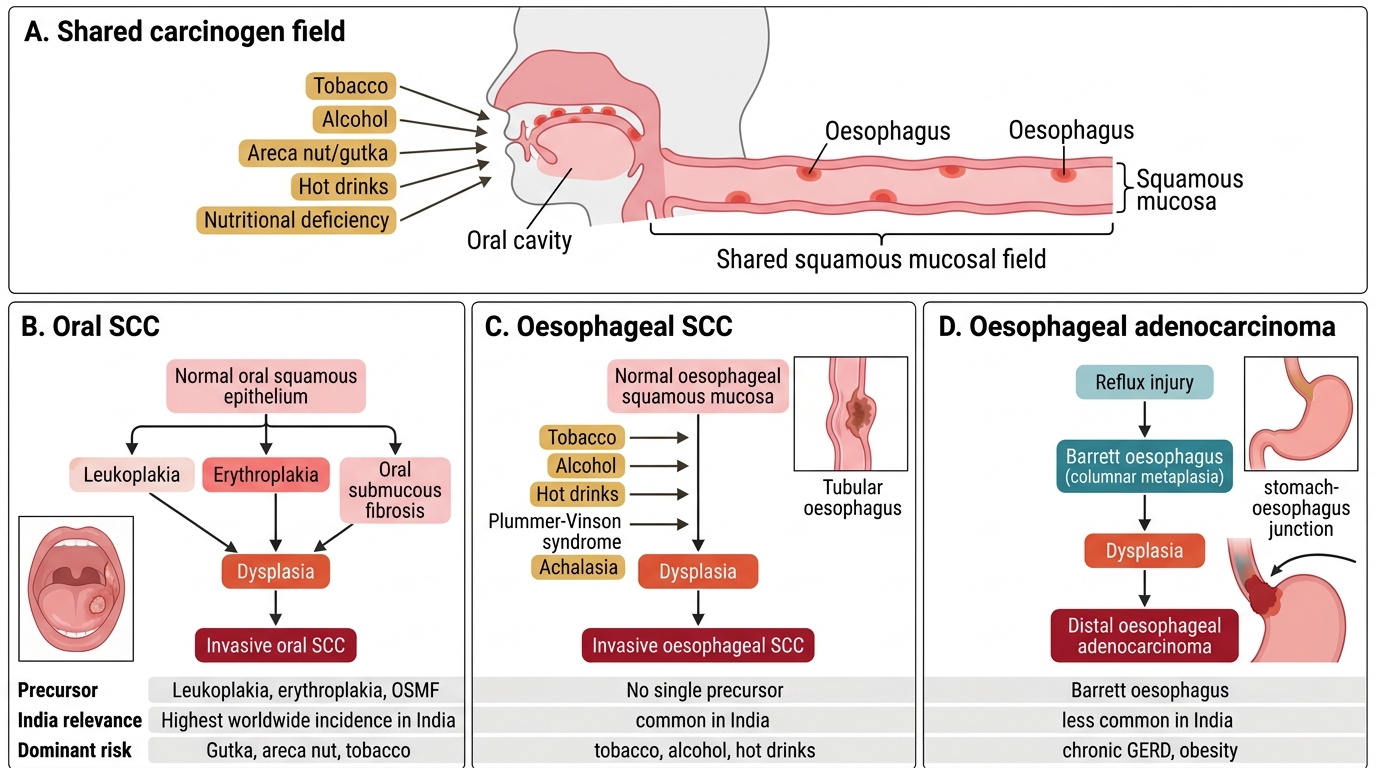
Oral and oesophageal SCC share a common carcinogen pathway — tobacco, alcohol, and nutritional deficiency — and this is not coincidental. Both arise in squamous-lined mucosa, both may be caused by the same field of carcinogenesis (hence patients with oral SCC have higher rates of oesophageal SCC and vice versa), and both have premalignant counterparts.
Key comparisons:
| Feature | Oral SCC | Oesophageal SCC | Oesophageal Adenocarcinoma |
|---|---|---|---|
| Precursor | Leukoplakia, erythroplakia, OSMF | No well-defined single precursor (Plummer-Vinson, achalasia) | Barrett oesophagus |
| India relevance | Highest worldwide incidence | Common | Less common |
| Dominant risk | Gutka, areca nut, tobacco | Tobacco, alcohol, hot drinks | GERD, obesity |
| Spread route | Cervical LN | Mediastinal LN; early intramural | Coeliac/gastric LN |
| Prognosis | Stage-dependent; early = good | Late presentation; ~15–20 % 5-yr | Better if caught at Barrett stage |
Field cancerisation links all aerodigestive SCC — a patient with oral SCC requires endoscopic surveillance of the oesophagus. Conversely, a patient with oesophageal SCC should have the oral cavity and larynx examined.