Page 7 of 28
PA23.3-4 | Peptic Ulcer Disease & Gastric Carcinoma — SDL Guide (Part 3)
Gastric Carcinoma — Epidemiology & Risk Factors
Gastric Carcinoma: Epidemiology and Risk Factors
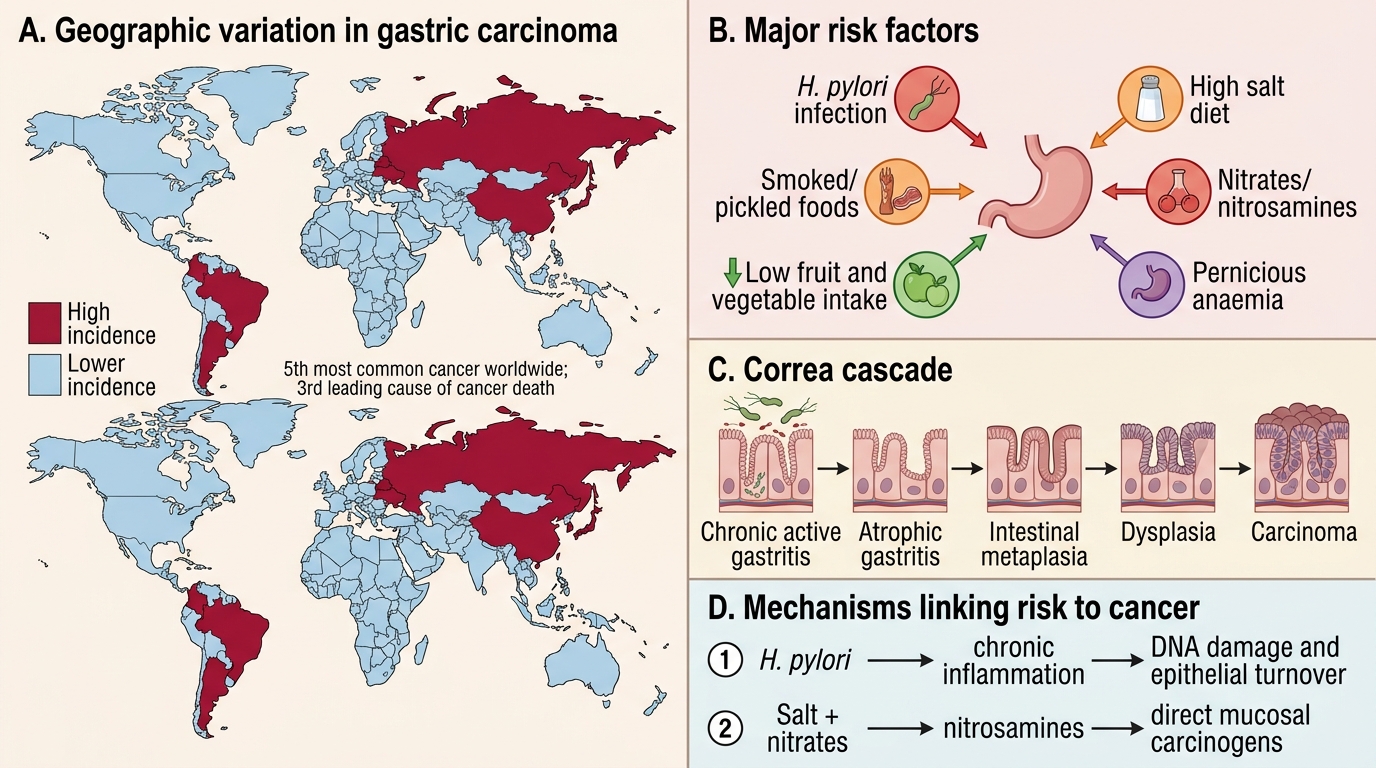
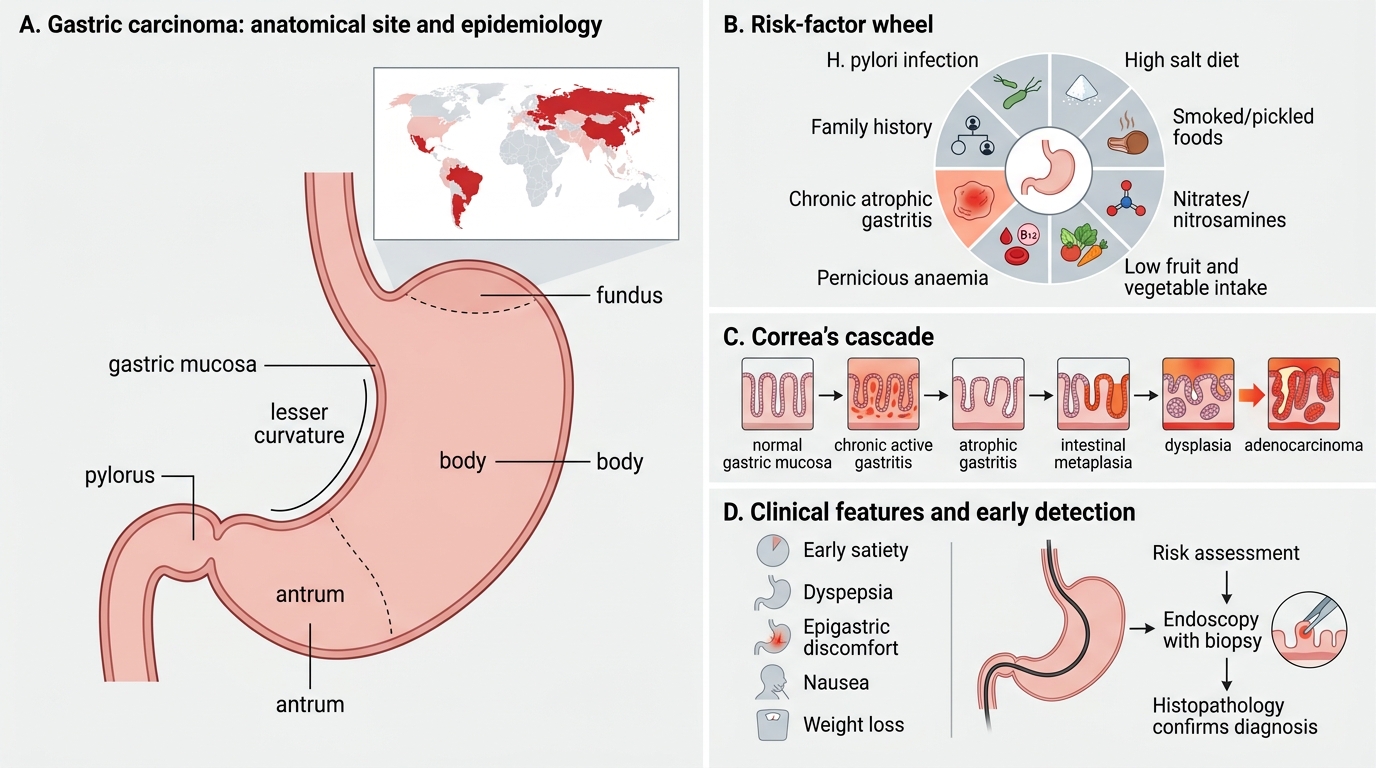
Gastric carcinoma is the fifth most common cancer worldwide and the third most common cause of cancer death. It has a striking geographic variation: highest incidence in East Asia (Japan, South Korea, China), Eastern Europe, and South America; lower in North America and Western Europe.
Risk factors (recall and link to pathogenesis):
- H. pylori infection — WHO Group 1 carcinogen. Present in 60-80% of gastric adenocarcinomas. Risk is 3-6× elevated. Mechanism: chronic active gastritis → atrophic gastritis → intestinal metaplasia → dysplasia → carcinoma (Correa's cascade).
- Diet: high salt, smoked/pickled foods, nitrates → nitrosamines (direct carcinogens); low fruit/vegetable intake (reduced antioxidants).
- Pernicious anaemia (autoimmune atrophic gastritis) — 2-3× increased risk; achlorhydria allows bacterial overgrowth → increased nitrite reduction.
- Previous gastric surgery — remnant gastritis, bile reflux.
- Smoking — independent risk factor.
- Family history / genetic factors: hereditary diffuse gastric cancer (CDH1 mutations, E-cadherin loss → diffuse type); first-degree relatives of affected individuals have 2-3× risk.
- Blood group A — classically associated (diffuse type), mechanism unclear.
Protective: Fresh fruit and vegetables, refrigeration (replaced salting/smoking), H. pylori eradication.
Lauren Classification — Intestinal vs Diffuse Type
⚑ AI image — pending faculty review (auto-QA score 8/10; best of 3 attempts)
Lauren Classification: Intestinal vs Diffuse Gastric Adenocarcinoma
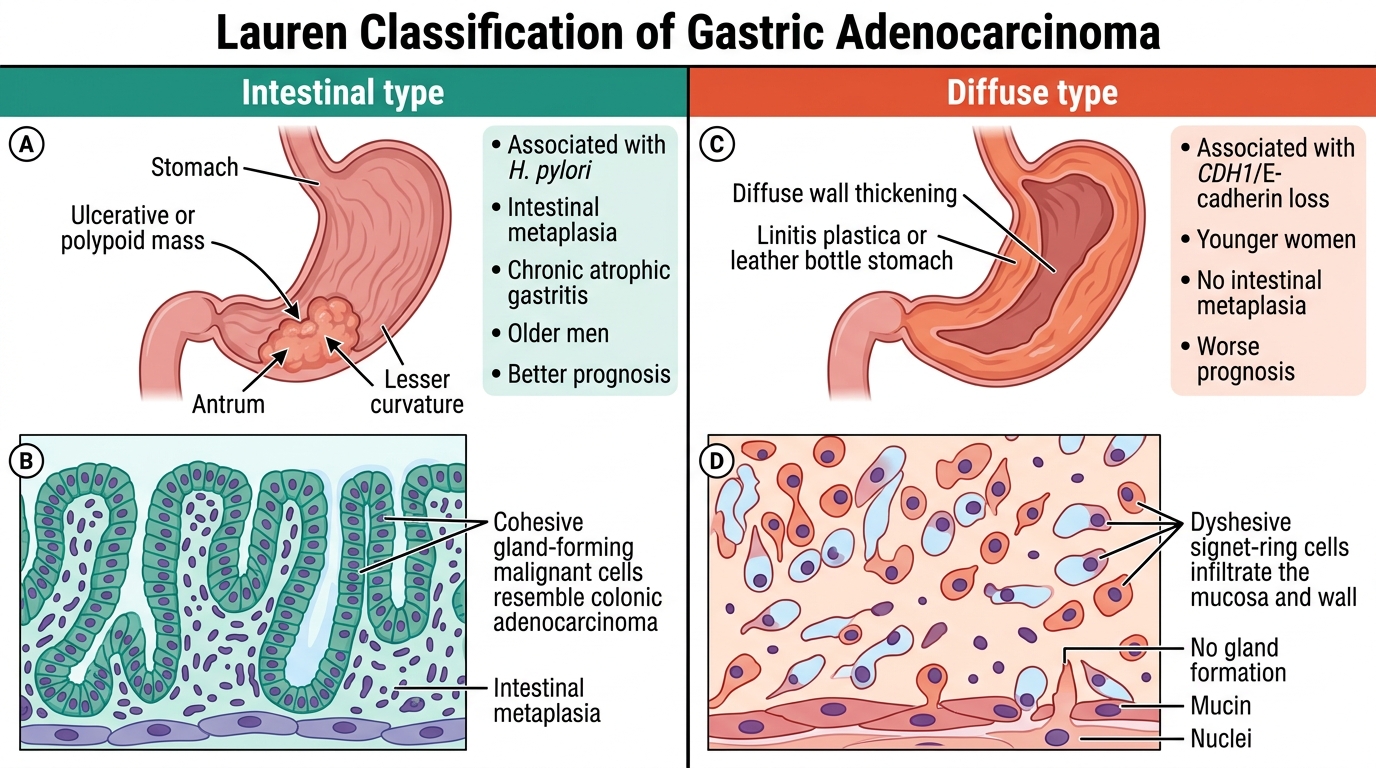
The Lauren classification (1965) divides gastric adenocarcinoma into two histogenetically and prognostically distinct types. This is the most important classification for both exam and clinical practice.
Intestinal type:
• Resembles intestinal/colonic adenocarcinoma — gland-forming, cohesive cells.
• Associated with H. pylori, intestinal metaplasia, dietary carcinogens, chronic atrophic gastritis.
• More common in high-incidence populations (Japan, Korea).
• Occurs in older patients (60-70s), slight male predominance.
• Better prognosis (more often localised, responds to surgery).
• Grossly: ulcerative or polypoid; located in antrum/lesser curvature.
Diffuse type:
• Individual tumour cells infiltrate the mucosa and wall diffusely — NO gland formation.
• Cells are dyshesive (loss of E-cadherin, encoded by CDH1) → cannot stick together.
• Signet-ring cells: tumour cells filled with intracytoplasmic mucin that displaces the nucleus to the periphery — pathognomonic on histology.
• When the entire stomach is infiltrated → linitis plastica ('leather bottle stomach'): a rigid, thickened, non-distensible stomach on gross exam and barium study.
• More common in younger patients, women, Western populations.
• NOT associated with intestinal metaplasia; not part of Correa's cascade.
• Worse prognosis — diffuse infiltration makes surgical margins difficult; often presents at advanced stage.
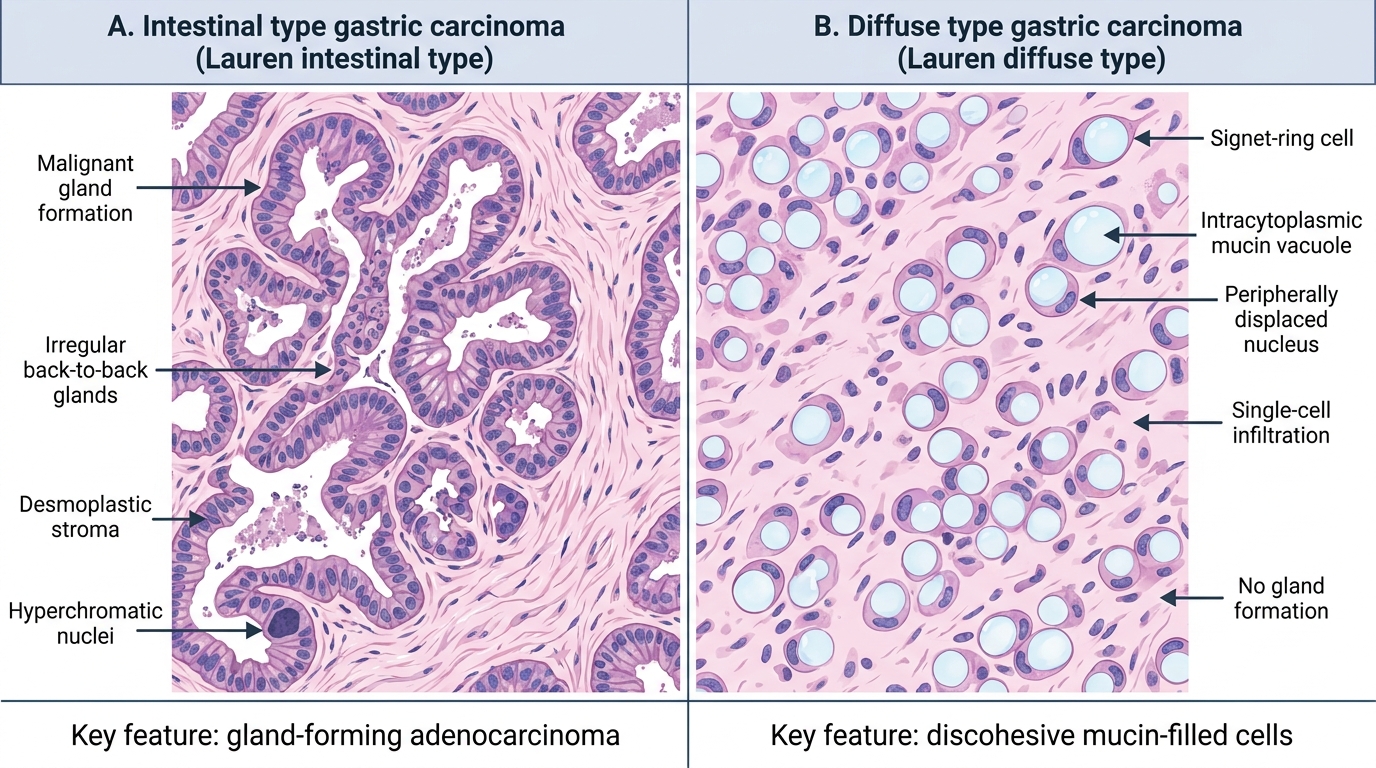
Lauren Types of Gastric Carcinoma: Histology Comparison
SELF-CHECK
A 38-year-old woman undergoes gastrectomy for gastric carcinoma. Histology shows individual tumour cells with large cytoplasmic mucin vacuoles compressing the nucleus to the periphery, diffusely infiltrating the entire gastric wall with no gland formation. The CORRECT characterisation of this tumour is:
A. Intestinal-type gastric adenocarcinoma arising on a background of intestinal metaplasia
B. Diffuse-type gastric adenocarcinoma with signet-ring cells — Lauren diffuse
C. Poorly differentiated squamous cell carcinoma of the stomach
D. Gastrointestinal stromal tumour (GIST) with epithelioid morphology
Reveal Answer
Answer: B. Diffuse-type gastric adenocarcinoma with signet-ring cells — Lauren diffuse
The description — individual non-gland-forming cells with intracytoplasmic mucin displacing the nucleus (signet-ring cells), diffuse wall infiltration — is classic Lauren diffuse-type gastric adenocarcinoma. When it involves the entire stomach, the gross picture is linitis plastica. It is NOT associated with intestinal metaplasia (unlike intestinal type). GIST does not show signet-ring mucin cells; squamous cell carcinoma is exceedingly rare in the stomach.
Gross Pathology & Spread of Gastric Carcinoma
Gross Pathology and Spread of Gastric Carcinoma
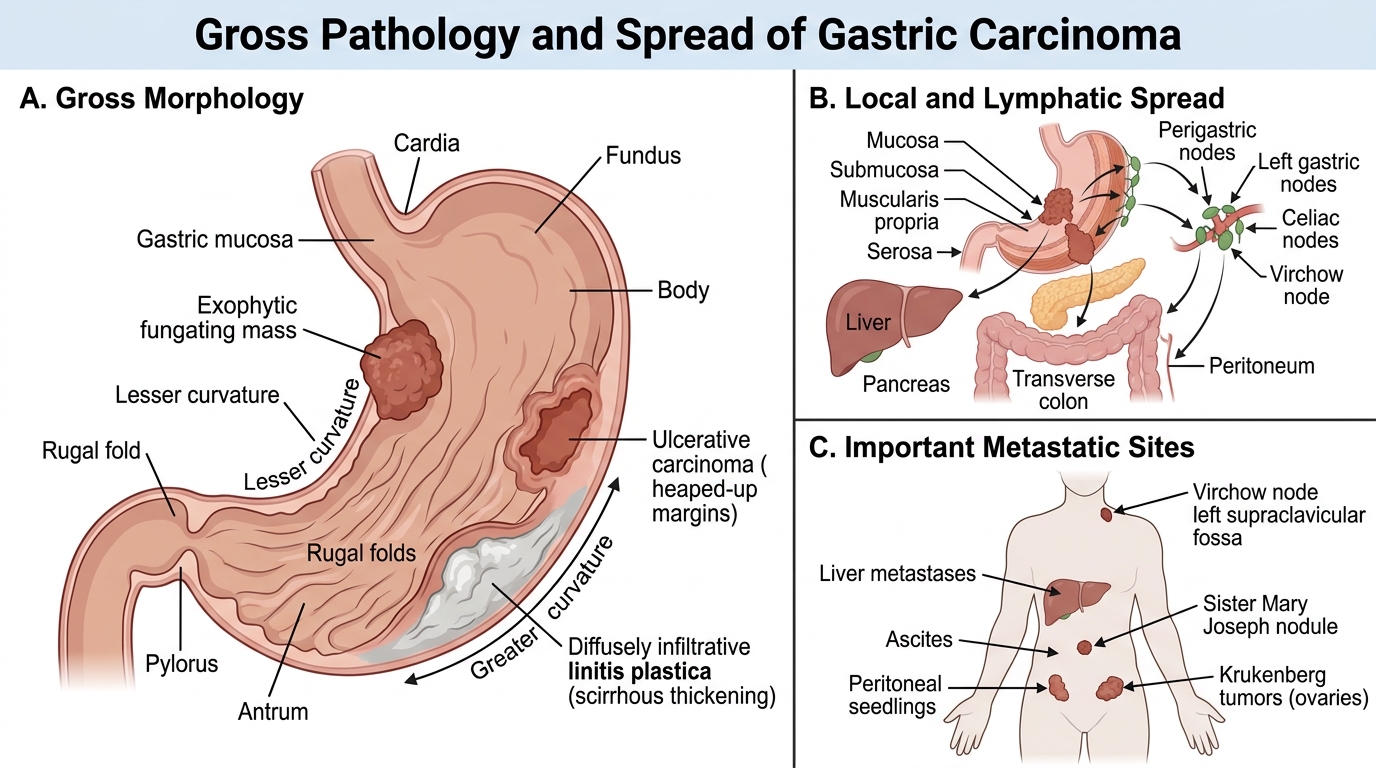
Gross patterns of gastric carcinoma (Borrmann classification):
• Fungating (exophytic/polypoid) — protrudes into lumen; better prognosis, often intestinal type.
• Ulcerative — irregular ulcer with heaped margins; must distinguish from benign ulcer (see earlier block).
• Infiltrative (diffuse/linitis plastica) — wall thickened, rigid, leather-bottle appearance; worst prognosis.
• Superficial spreading — early gastric cancer confined to mucosa/submucosa; excellent prognosis if resected.
Microscopy: Adenocarcinoma with variable differentiation. Intestinal type: tubular/papillary glands. Diffuse type: signet-ring cells, poorly cohesive. Both may have mucin pools (mucinous carcinoma).
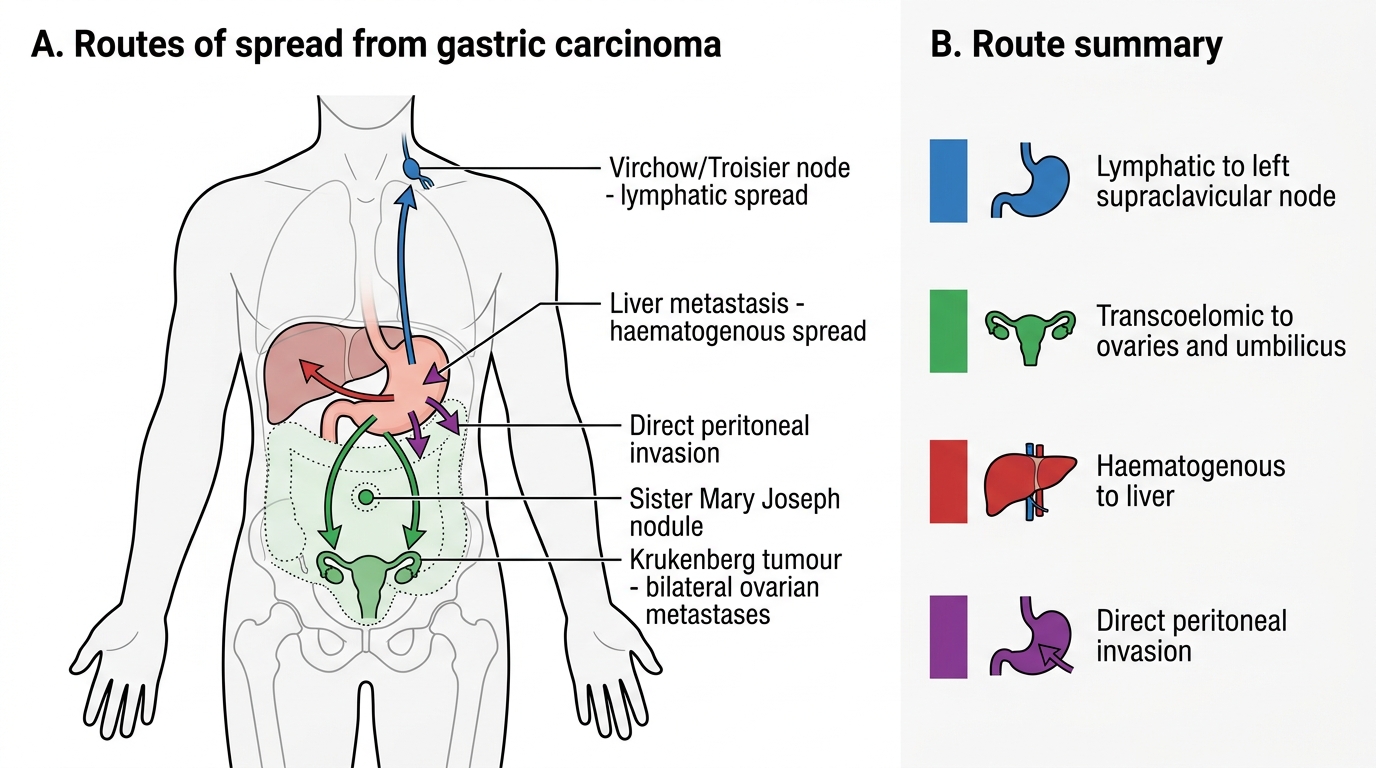
Routes of spread:
| Route | Site | Eponym |
|---|---|---|
| Lymphatic — left supraclavicular | Virchow node (sentinel node) | Troisier's sign |
| Transcoelemic — bilateral ovaries | Mucinous ovarian mets | Krukenberg tumour |
| Transcoelomic — umbilicus | Subcutaneous umbilical nodule | Sister Mary Joseph nodule |
| Direct — peritoneum | Malignant ascites, omental cake | — |
| Haematogenous | Liver (most common), lungs, bone | — |
Prognosis: Overall 5-year survival < 25% in most countries (late diagnosis). In Japan, mass screening detects early gastric cancer → 5-year survival > 90% for Stage I. India lacks screening → most present at Stage III-IV.
Routes of Spread of Gastric Carcinoma
SELF-CHECK
A patient with known advanced gastric carcinoma develops bilateral ovarian masses on ultrasound. Histology of the ovarian tumour shows sheets of signet-ring cells in an abundant fibrous stroma. This represents:
A. Primary mucinous ovarian carcinoma — an incidental finding
B. Krukenberg tumour — transcoelomic metastasis from gastric carcinoma
C. Direct extension of gastric carcinoma into the ovaries via the broad ligament
D. Haematogenous ovarian metastasis from gastric carcinoma
Reveal Answer
Answer: B. Krukenberg tumour — transcoelomic metastasis from gastric carcinoma
Krukenberg tumour refers to bilateral ovarian metastases — classically from gastric carcinoma (most common) but also from colorectal or breast cancers. The route is transcoelomic (peritoneal seeding), not direct extension. Histology shows signet-ring cells embedded in a cellular ovarian stroma (desmoplastic reaction). The bilateral nature and presence of a known gastric primary clinch the diagnosis. Primary mucinous ovarian carcinoma is typically unilateral and does not show signet-ring cells.
Clinical Features & Early Detection
Gastric Carcinoma: Risk Factors, Pathogenesis, and Early Detection
Peptic ulcer disease — clinical features:
• Duodenal ulcer: Epigastric pain 2-3 hours after meals, relieved by food/antacids; classic nocturnal awakening. Periodicity (weeks of pain, weeks of remission).
• Gastric ulcer: Pain precipitated by food (within 30-60 min); may cause food fear and weight loss.
• Investigations: H. pylori testing (CLO test, urea breath test, stool antigen, serology); endoscopy with biopsy (especially all gastric ulcers).
Gastric carcinoma — clinical features:
• Insidious onset — 'silent' until advanced; presenting symptoms include epigastric discomfort, weight loss, early satiety, dysphagia (cardia involvement), vomiting (pyloric obstruction).
• Alarm symptoms (mandate urgent endoscopy): unintentional weight loss, haematemesis/melaena, progressive dysphagia, epigastric mass, iron-deficiency anaemia.
• Signs of advanced disease: Virchow node (left supraclavicular lymphadenopathy), epigastric mass, ascites, hepatomegaly, Sister Mary Joseph nodule.
• Tumour markers: CEA and CA 19-9 are elevated in a minority; not diagnostic.
• Early gastric cancer (confined to mucosa/submucosa, regardless of lymph node status): excellent prognosis; detected only by endoscopic screening.