Page 6 of 28
PA23.3-4 | Peptic Ulcer Disease & Gastric Carcinoma — SDL Guide (Part 2)
Gross Morphology — Benign vs Malignant Gastric Ulcer
Benign vs Malignant Gastric Ulcer: Gross Morphology
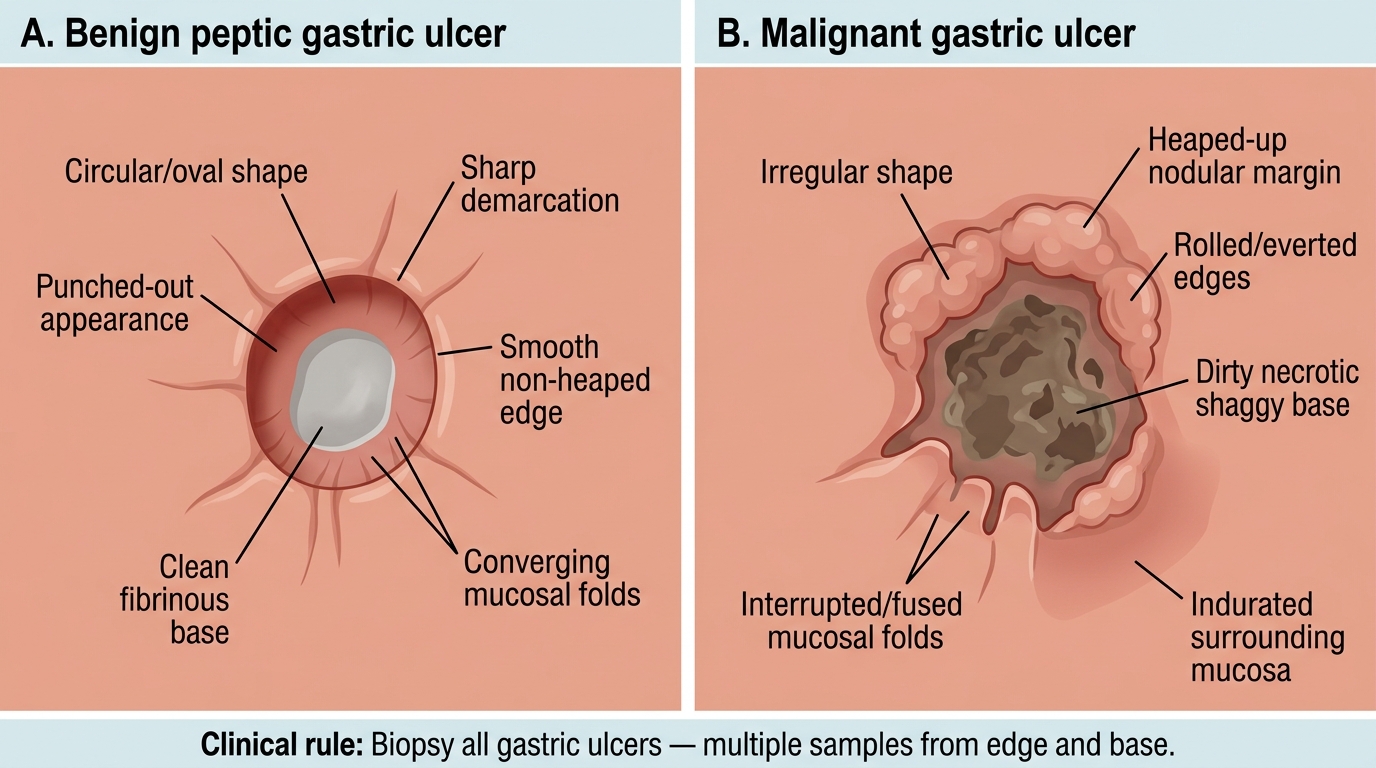
Distinguishing a benign peptic ulcer from a malignant (carcinomatous) ulcer on endoscopy and gross pathology is a high-yield clinical skill.
Benign peptic ulcer (classic features):
• Small, usually < 2 cm (duodenal nearly always < 1.5 cm).
• Punched-out appearance — circular or oval, with sharply demarcated perpendicular walls (like a cookie-cutter defect).
• Clean, flat base — often grey-white, covered by a thin fibrinous slough.
• Radiating mucosal folds converge toward the ulcer margin — a key sign of benign healing.
• Edges are smooth, not heaped; surrounding mucosa is pliable.
Malignant gastric ulcer (suspicious features — Mnemonic: MENACE):
• Often > 2-3 cm.
• Heaped-up, irregular, nodular margins — rolled, everted edges.
• Necrotic, shaggy, dirty base.
• Mucosal folds are interrupted or fused (do not converge cleanly).
• Surrounding mucosa is rigid, indurated.
• Location: body/fundus rather than antrum/lesser curvature raises suspicion.
> Clinical rule: ALL gastric ulcers require biopsy (multiple, from edges AND base). Duodenal ulcers are virtually never malignant and biopsy is not mandatory unless atypical.
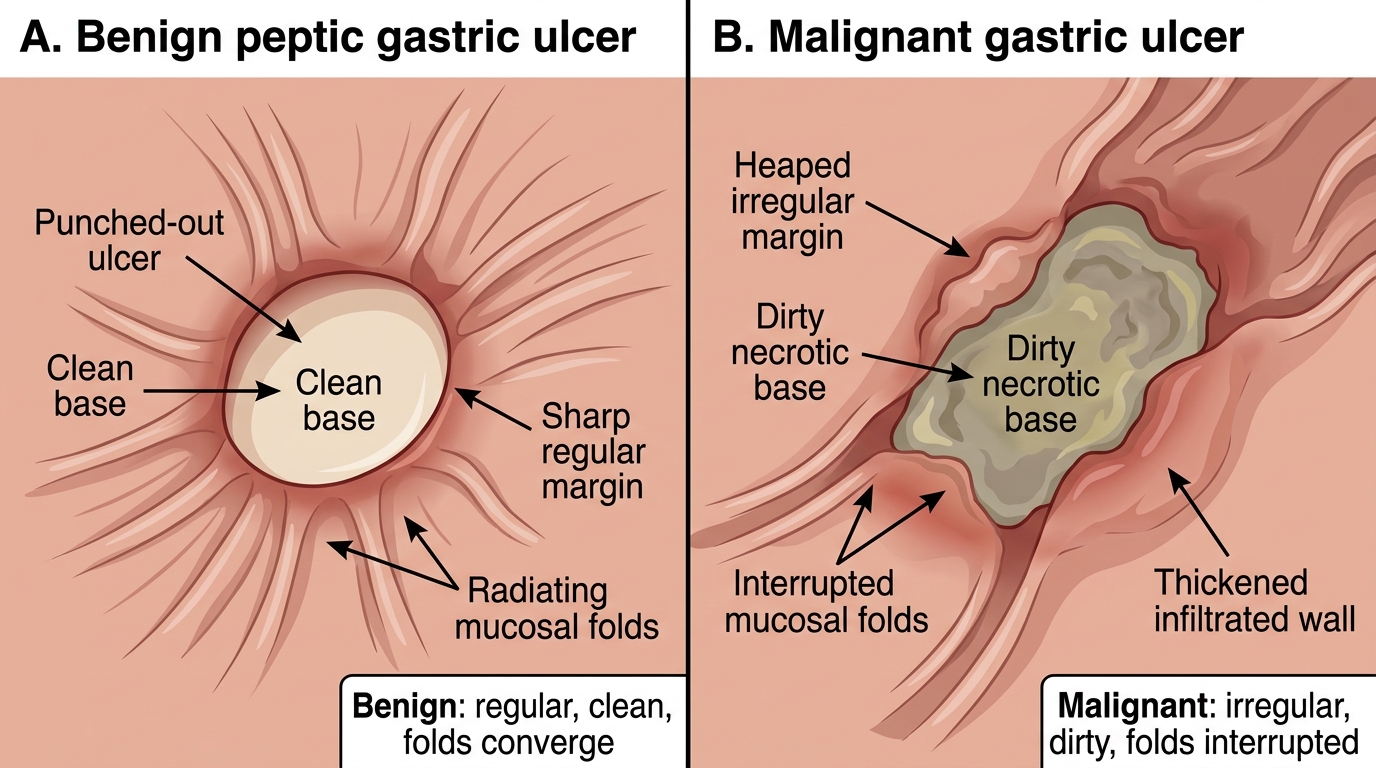
Gross Comparison of Benign and Malignant Gastric Ulcers
Microscopic Anatomy — The Four Zones of a Chronic Peptic Ulcer
Four Zones of a Chronic Peptic Ulcer
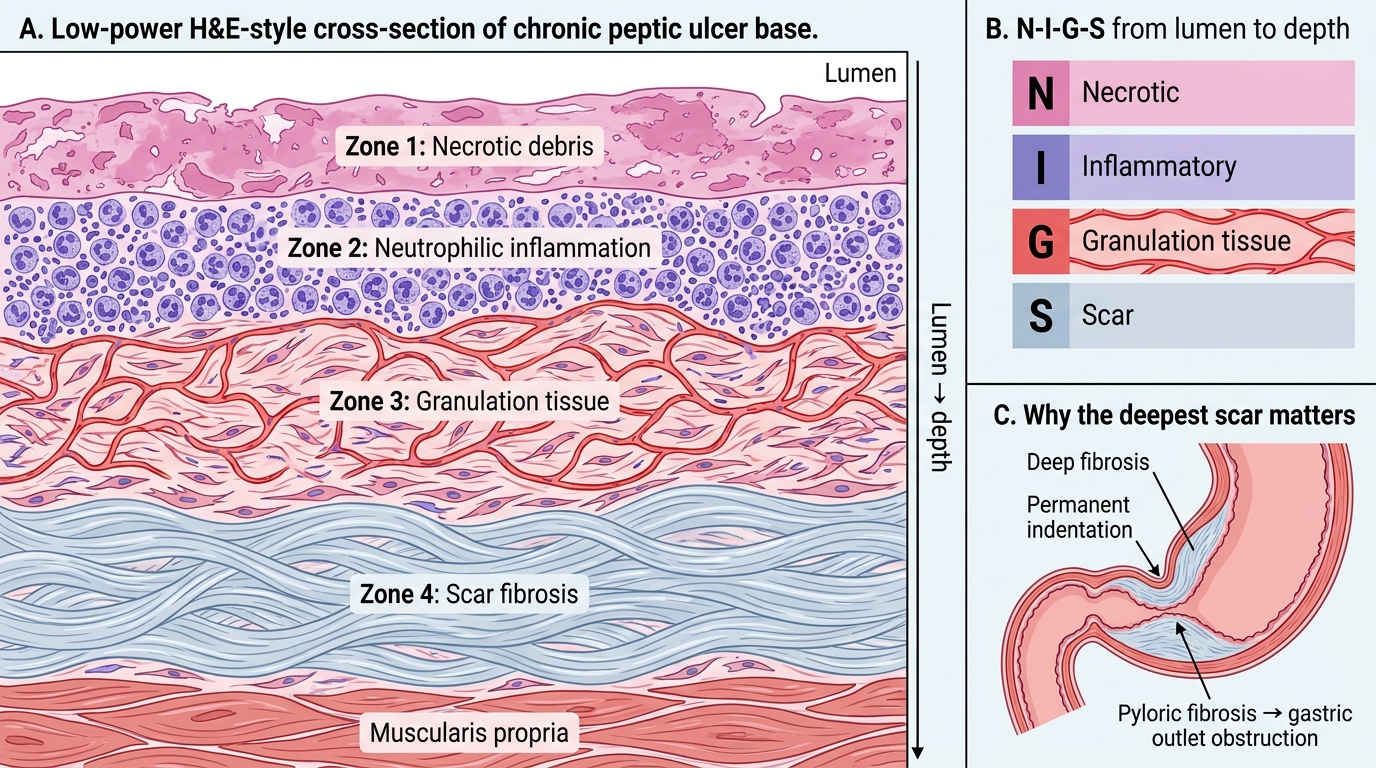
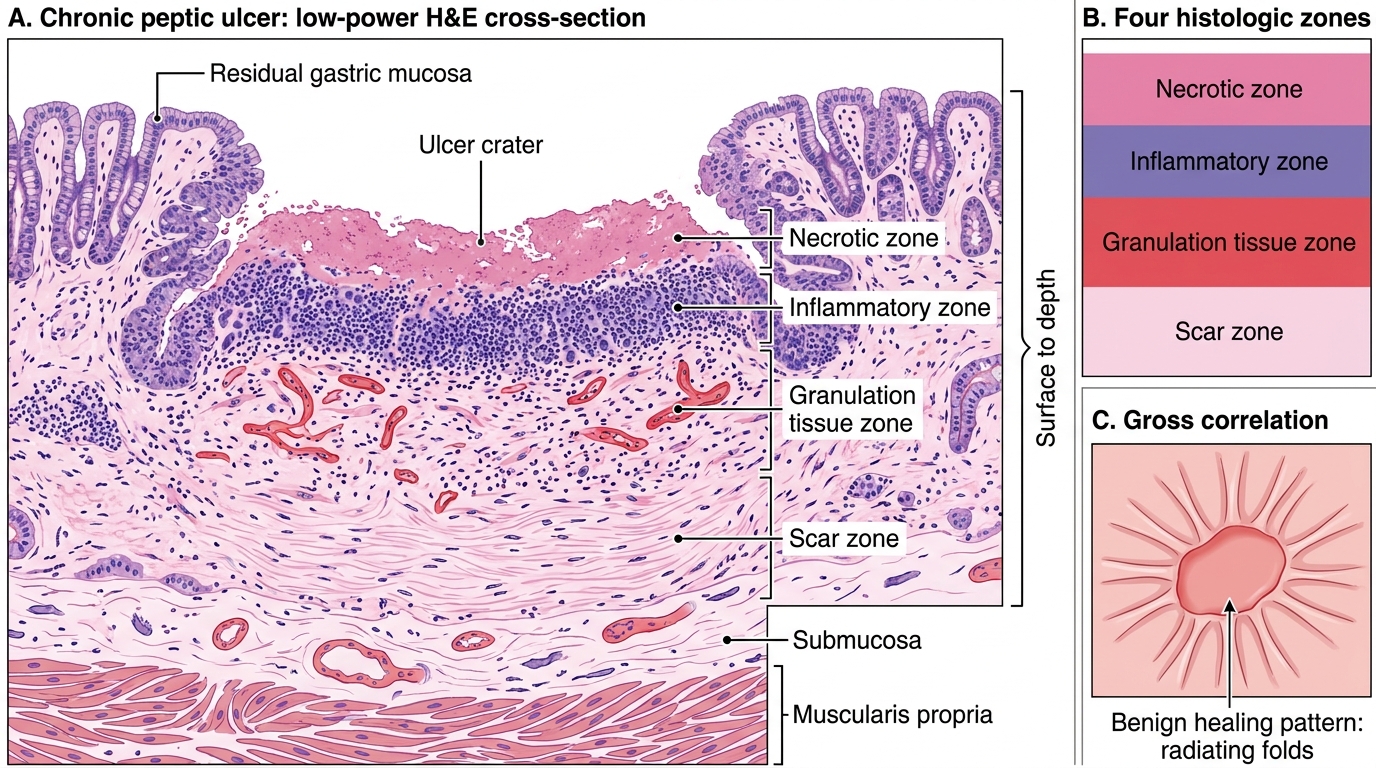
On histological section through the base of a chronic peptic ulcer, four concentric zones are seen from the luminal surface inward. This is a classical exam question.
Zone 1 — Necrotic (superficial)
Thin layer of eosinophilic necrotic debris, fibrin, and dead cells. This is the ulcer floor visible to the naked eye.
Zone 2 — Inflammatory (neutrophilic/exudative)
Dense neutrophilic infiltrate with fibrinous exudate. Active inflammation responsible for symptoms.
Zone 3 — Granulation tissue
Vascular loops, fibroblasts, and a mixed inflammatory infiltrate (lymphocytes, plasma cells, macrophages). This is the healing layer — what you want to see on follow-up biopsy.
Zone 4 — Scar (fibrosis)
Dense collagen replacing the muscularis propria. The deepest zone. Explains why healed ulcers may leave a permanent indentation and why obstructive complications occur (pyloric fibrosis → gastric outlet obstruction).
Remember: N-I-G-S (Necrotic → Inflammatory → Granulation → Scar), from lumen to depth.
Chronic Peptic Ulcer: Four Histologic Zones
SELF-CHECK
On histological examination of a gastric biopsy from a chronic peptic ulcer, the zone that lies DEEPEST (farthest from the lumen) and explains the complication of pyloric obstruction is:
A. Zone of active inflammation with dense neutrophil infiltration
B. Zone of granulation tissue with new capillary loops
C. Superficial zone of coagulative necrosis
D. Zone of dense fibrous scar replacing muscularis propria
Reveal Answer
Answer: D. Zone of dense fibrous scar replacing muscularis propria
The four zones from lumen inward are: (1) necrotic/fibrinous slough, (2) inflammatory (neutrophilic), (3) granulation tissue, and (4) dense fibrous scar. The scar zone replaces the muscularis propria and, when extensive in the pyloric region, causes fibrotic narrowing leading to gastric outlet obstruction — a well-recognised late complication of peptic ulcer disease.
Complications of Peptic Ulcer Disease
Complications of Peptic Ulcer Disease
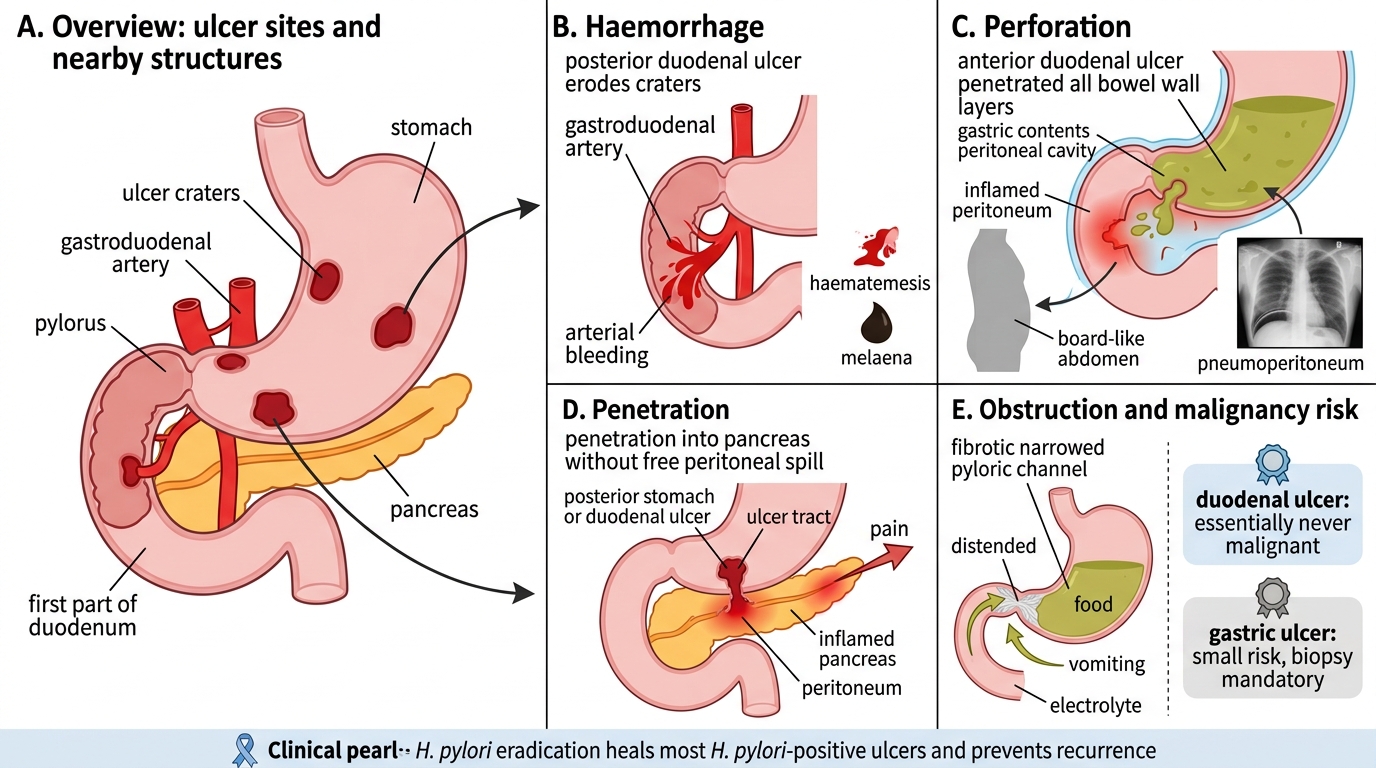
PUD complications are best learned systematically:
1. Haemorrhage (bleeding) — most common complication (~15-20% of patients). Posterior duodenal ulcers erode the gastroduodenal artery → major haemorrhage. Presents as haematemesis or melaena. Life-threatening: requires endoscopic haemostasis ± surgery.
2. Perforation — ulcer penetrates through all layers → gastric contents spill into peritoneal cavity → chemical peritonitis → bacterial peritonitis. Anterior duodenal ulcers perforate most often. Classic presentation: sudden, severe epigastric pain ('board-like abdomen'); erect CXR shows free air under diaphragm (pneumoperitoneum). Surgical emergency.
3. Penetration — ulcer erodes into an adjacent organ (without free perforation). Pancreatic penetration → pancreatitis; pain radiates to the back and is not relieved by antacids.
4. Pyloric/duodenal obstruction — fibrosis of the pyloric channel → gastric outlet obstruction. Presents with recurrent vomiting of undigested food, succussion splash, hypochloraemic hypokalaemic metabolic alkalosis. Endoscopic balloon dilatation or surgery.
5. Malignant transformation — duodenal ulcers essentially NEVER become malignant (a key distinguishing fact). Gastric ulcers have a small but real risk (<1%); this is why biopsy is mandatory.
> Clinical pearl: H. pylori eradication (triple/quadruple therapy) heals 90% of H. pylori-positive ulcers and prevents recurrence. Test-and-treat is now the standard of care.
CLINICAL PEARL
Zollinger-Ellison Syndrome (ZES): If a patient has multiple, recurrent, or atypically located peptic ulcers (distal duodenum, jejunum), resistant to standard therapy, think ZES. A gastrinoma (neuroendocrine tumour, usually in the 'gastrinoma triangle' — head of pancreas/duodenum) hypersecrets gastrin → massively elevated acid output → multiple ulcers + secretory diarrhoea. Part of MEN-1 syndrome in 25%. Diagnosis: fasting serum gastrin > 1000 pg/mL + secretin stimulation test. Treatment: high-dose PPI + tumour resection.
SELF-CHECK
A 45-year-old man has a posterior duodenal ulcer. He presents acutely with epigastric pain radiating to the back, and serum amylase is elevated. The MOST likely complication is:
A. Perforation into the peritoneal cavity with free air under the diaphragm
B. Penetration into the pancreas causing pancreatitis
C. Malignant transformation of the duodenal ulcer
D. Pyloric obstruction causing hypochloraemic alkalosis
Reveal Answer
Answer: B. Penetration into the pancreas causing pancreatitis
Posterior duodenal ulcers are classically associated with penetration into the pancreas (not free perforation, which is more characteristic of anterior ulcers). Pancreatic penetration causes pain that radiates to the back, is not relieved by antacids, and may elevate serum amylase/lipase. Malignant transformation of duodenal ulcers is extremely rare. Pyloric obstruction causes vomiting, not back pain or elevated amylase.