Page 14 of 25
PA20.2 | DIC & Vitamin K Deficiency — SDL Guide
Learning Objectives
- Define disseminated intravascular coagulation (DIC) and explain the paradox of simultaneous thrombosis and haemorrhage.
- List the major triggers of DIC and link each to the pathogenetic mechanism of tissue factor release.
- Interpret the classic DIC laboratory panel: thrombocytopenia, prolonged PT and aPTT, low fibrinogen, elevated D-dimer/FDPs, and schistocytes.
- Distinguish acute DIC from chronic (compensated) DIC using clinical and laboratory criteria.
- Explain the role of vitamin K in γ-carboxylation of coagulation factors II, VII, IX, and X.
- List causes of vitamin K deficiency and predict the laboratory pattern (PT-first prolongation, normal fibrinogen and platelets).
- Construct a three-way differential comparison table distinguishing DIC, liver disease, and vitamin K deficiency.
INSTRUCTIONS
Haemostasis is a tightly regulated balance. In DIC that balance catastrophically tips both ways at once — the body clots and bleeds simultaneously. Understanding why requires you to trace the sequence from trigger → thrombin burst → factor consumption → secondary fibrinolysis. Vitamin K deficiency offers a clean counterpoint: the coagulation defect is selective, platelets are unaffected, and correction is straightforward. Together these two conditions form the backbone of the PA20.2 competency and appear repeatedly in clinical pathology examinations and clinical practice.
References
- Robbins & Kumar: Basic Pathology, 11th ed., Ch 4 (Haemodynamic Disorders) (textbook)
- Bancroft & Lakin: Theory and Practice of Histological Techniques, 8th ed. (textbook)
- Hoffbrand & Steensma: Essential Haematology, 8th ed., Ch 28 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman is brought to the emergency department 6 hours after a car accident. She received 8 units of packed red cells. Now she is oozing from IV sites, her gums are bleeding, and her left calf is swollen and tender — a clot. Her platelet count is 38 × 10⁹/L, PT 28 s, aPTT 62 s, fibrinogen 0.6 g/L, D-dimer > 20 mg/L. She is clotting and bleeding at the same time. How is that possible?
WHY THIS MATTERS
Disseminated intravascular coagulation (DIC) and vitamin K deficiency are two of the most-tested coagulation disorders in the MBBS pathology curriculum. DIC is a life-threatening complication encountered in surgical ICUs, obstetric wards, oncology units, and general medicine. Vitamin K deficiency is a common correctable cause of bleeding in neonates, patients on broad-spectrum antibiotics, and those with malabsorption. Both disorders are distinguished partly by their lab panels — mastering those panels will directly improve your diagnostic accuracy in clinical postings.
RECALL
Before starting, revisit these concepts from earlier in the Haemostasis cluster:
- The coagulation cascade: intrinsic (contact) pathway → aPTT; extrinsic (tissue factor) pathway → PT. Both converge at factor X.
- Thrombin converts fibrinogen → fibrin and activates platelets, factors V and VIII (positive feedback).
- Fibrinolysis: plasmin degrades cross-linked fibrin → releases D-dimer (a fibrin-specific fragment).
- From H5 (MAHA and TTP/HUS): schistocytes are red cell fragments formed when erythrocytes are sheared by fibrin strands in small vessels — their presence confirms microangiopathic haemolytic anaemia (MAHA).
If any of these feel uncertain, take 3 minutes to re-read the H9 SDL summary before continuing.
What Is DIC? The Core Paradox
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
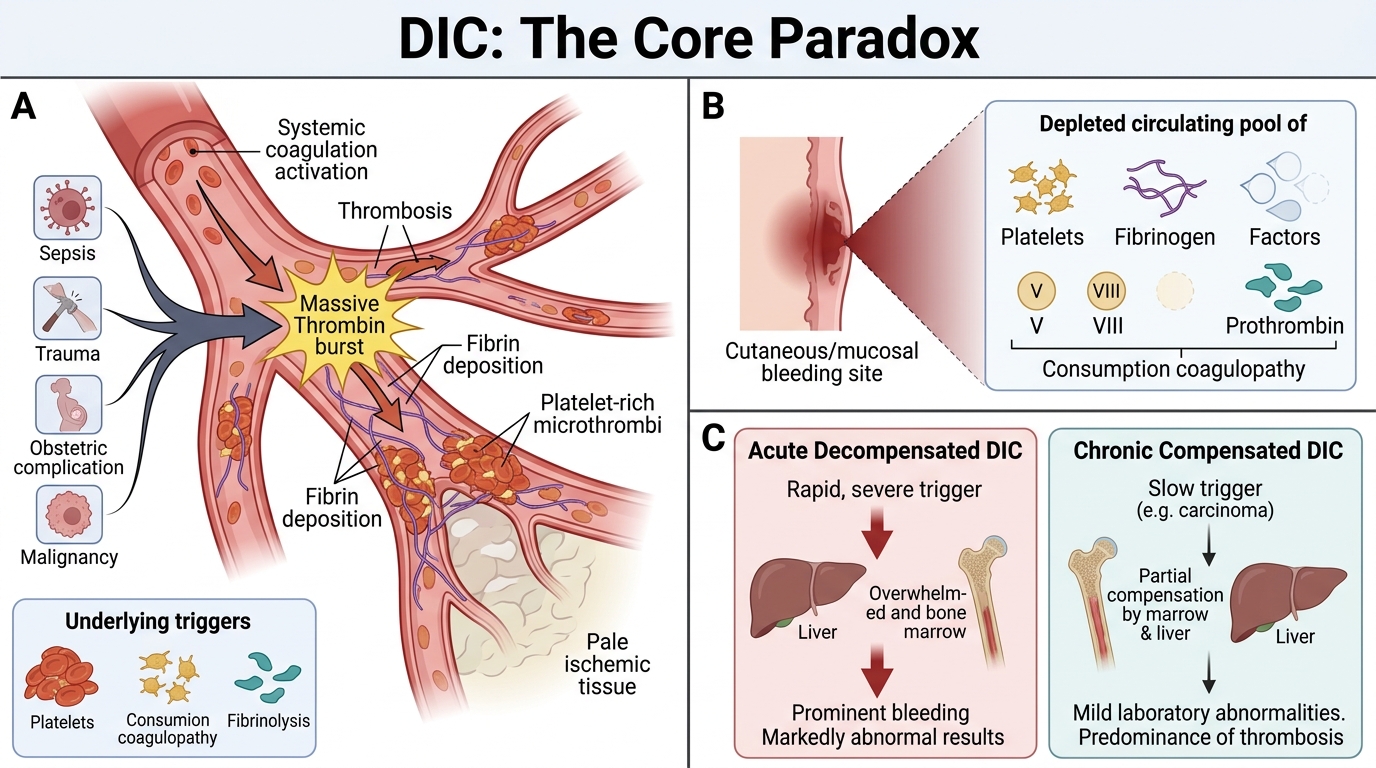
DIC: Clotting and Bleeding Paradox
Disseminated intravascular coagulation (DIC) is a pathological syndrome in which systemic, uncontrolled activation of the coagulation cascade leads to:
- Widespread formation of microthrombi in small vessels → organ ischaemia and failure.
- Consumption of platelets, fibrinogen, and clotting factors (factors V, VIII, prothrombin) → consumption coagulopathy.
- Secondary activation of fibrinolysis (because fibrin is being deposited) → secondary fibrinolysis → release of FDPs and D-dimer that further inhibit platelet function and fibrin polymerisation.
The paradox: the same patient clots (microthrombi) and bleeds (factor and platelet depletion). DIC is not a primary disease — it is always secondary to an underlying trigger.
DIC is classified as:
• Acute (decompensated) DIC: rapid trigger, bone marrow and liver cannot keep up → clinical bleeding dominates.
• Chronic (compensated) DIC: slow trigger (e.g., carcinoma), marrow partially compensates → thrombosis may dominate, lab values mildly abnormal.
Triggers of DIC

Major Triggers of Disseminated Intravascular Coagulation
Any condition that releases large amounts of tissue factor (TF) or activates the contact pathway systemically can trigger DIC. The most important categories are:
| Category | Examples | Mechanism |
|---|---|---|
| Sepsis | Gram-negative endotoxin (LPS), gram-positive exotoxins | LPS induces TF expression on monocytes and endothelial cells; cytokine storm (TNF, IL-1) amplifies |
| Obstetric | Placental abruption, amniotic fluid embolism, retained products of conception | Placental TF + amniotic fluid (rich in TF and phospholipids) enter maternal circulation |
| Trauma / Burns | Crush injury, massive burns | Widespread tissue destruction releases TF from exposed sub-endothelium and damaged cells |
| Malignancy | Acute promyelocytic leukaemia (APL), mucin-secreting adenocarcinoma | APL granules contain TF; mucin activates factor X directly |
| Others | Snakebite (venom activates factor X/prothrombin), ABO-incompatible transfusion | Direct activation of coagulation proteases or immune complex-mediated endothelial injury |
Clinical pearl: APL (AML-M3) is the single haematologic malignancy most strongly associated with DIC and is a therapeutic emergency — starting ATRA before chemotherapy reverses the DIC.
Pathogenesis of DIC — The Three-Step Cascade

DIC Pathogenesis: Three-Step Cascade
Understanding the mechanism as three linked steps prevents confusion:
Step 1 — Tissue factor release and thrombin burst
Massive TF expression (from damaged endothelium, activated monocytes, or circulating tumour products) drives extrinsic pathway activation → explosive thrombin generation. Thrombin converts fibrinogen to fibrin and activates platelets in bulk.
Step 2 — Microthrombi and consumption
Fibrin clots form throughout the microvasculature. This consumes:
• Platelets → thrombocytopenia
• Fibrinogen → hypofibrinogenaemia
• Factors V, VIII, II → prolonged PT and aPTT
Fibrin strands in capillaries shear red cells → schistocytes and microangiopathic haemolytic anaemia (MAHA).
Step 3 — Secondary fibrinolysis
Fibrin deposition triggers plasmin activation → fibrin degradation products (FDPs) and D-dimer released in large quantities. FDPs and D-dimer inhibit fibrin polymerisation and impair platelet aggregation → worsening haemorrhage.
The net result: clotting and bleeding occur simultaneously.

DIC Pathogenesis: Three-Stage Self-Amplifying Cycle
SELF-CHECK
In DIC, what is the PRIMARY mechanism by which most triggers initiate coagulation activation?
A. Massive tissue factor release driving the extrinsic coagulation pathway
B. Activation of the intrinsic (contact) pathway by collagen exposure
C. Direct platelet aggregation by bacterial toxins without thrombin generation
D. Inhibition of protein C leading to unopposed factor Va activity
Reveal Answer
Answer: A. Massive tissue factor release driving the extrinsic coagulation pathway
The vast majority of DIC triggers (gram-negative sepsis, obstetric catastrophes, solid tumours, APL) act by inducing tissue factor (TF) expression on monocytes, endothelial cells, or by releasing TF-rich material into the circulation. This drives the extrinsic pathway → explosive thrombin generation. While the contact pathway (option A) may contribute in some settings, TF-driven extrinsic activation is the dominant and therapeutically relevant mechanism.