Page 15 of 25
PA20.2 | DIC & Vitamin K Deficiency — SDL Guide (Part 2)
Clinical Features of DIC

Clinical Features of Disseminated Intravascular Coagulation
The clinical picture reflects the dual pathology of thrombosis and haemorrhage:
Haemorrhagic manifestations:
• Bleeding from multiple sites simultaneously — venepuncture sites, IV cannulas, surgical wounds, mucous membranes
• Ecchymoses and purpura
• Haematuria, haemoptysis, gastrointestinal bleeding in severe cases
Thrombotic manifestations (often subclinical):
• Microthrombi in kidneys → acute tubular necrosis, oliguria/anuria
• Microthrombi in lungs → ARDS
• Microthrombi in brain → encephalopathy, seizures
• Purpura fulminans: haemorrhagic necrosis of skin from dermal vessel thrombosis — a dramatic and grave sign
Key clinical rule: bleeding from at least three unrelated sites in a critically ill patient should prompt urgent DIC screen. The underlying trigger must be treated simultaneously — treating DIC without treating sepsis or delivering the placenta is futile.
Acute DIC presents with dramatic haemorrhage. Chronic DIC (e.g., from metastatic carcinoma or giant haemangioma — Kasabach-Merritt syndrome) may present insidiously with deep vein thrombosis and mild lab abnormalities.
Laboratory Findings in DIC — The Classic Panel

Classic Laboratory Panel in Acute DIC
The DIC laboratory panel is one of the most important diagnostic panels in clinical pathology. Learn it as a complete pattern:
| Test | Typical finding in acute DIC | Why |
|---|---|---|
| Platelet count | ↓ (< 100 × 10⁹/L) | Consumed in microthrombi |
| PT | ↑ (prolonged) | Factors II, V, VII, X consumed |
| aPTT | ↑ (prolonged) | Factors V, VIII, fibrinogen depleted |
| Fibrinogen | ↓↓ (< 1.0 g/L in severe DIC) | Consumed; fibrinogen is an acute-phase reactant so even a "normal" level may be low relative to expected baseline |
| D-dimer | ↑↑ (markedly elevated) | Secondary fibrinolysis of cross-linked fibrin |
| FDPs | ↑↑ | Fibrinolysis products; inhibit further fibrin polymerisation |
| Peripheral blood film | Schistocytes (fragmented RBCs) | MAHA from fibrin-strand shearing |
ISTH scoring system (simplified): Platelet count, PT prolongation, fibrinogen level, and D-dimer are scored 0-2 each. A score ≥ 5 is consistent with overt DIC. The score is also used to track treatment response.
Chronic DIC: D-dimer and FDPs are elevated, fibrinogen may be normal or high (compensated), platelets may be low-normal.

DIC Laboratory Panel: Key Tests and Pathophysiology
CLINICAL PEARL
D-dimer vs FDPs — know the difference: D-dimer is a fibrin-specific degradation product (from cross-linked fibrin) and is the more specific DIC marker. FDPs include both fibrinogen and fibrin breakdown products — they are sensitive but less specific. A very high D-dimer with elevated FDPs strongly supports secondary fibrinolysis in DIC. In primary fibrinolysis (rare, e.g., thrombolytic overdose), FDPs are elevated but D-dimer is low-to-normal because cross-linked fibrin is not the primary substrate. This distinction matters in examinations.
Schistocytes and MAHA in DIC
Schistocytes and MAHA in DIC
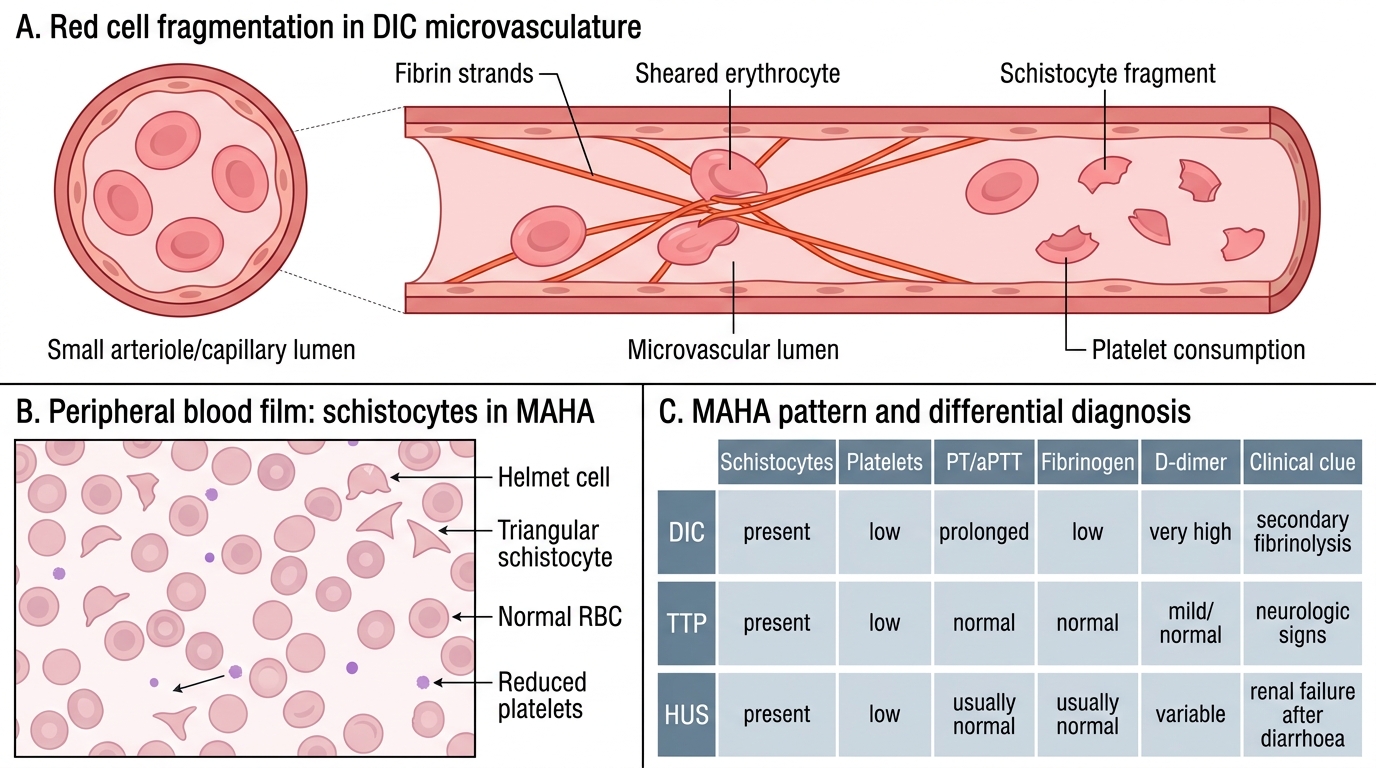
Red cell fragmentation occurs when erythrocytes are mechanically sheared by fibrin strands stretched across microvascular lumens. The resulting fragments — schistocytes (also called helmet cells or fragmented red cells) — are visible on the peripheral blood film as irregular, helmet-shaped, or triangular red cell remnants.
In DIC, the combination of:
• Schistocytes on film
• Thrombocytopenia
• Elevated LDH and falling haemoglobin
…constitutes microangiopathic haemolytic anaemia (MAHA). MAHA is not unique to DIC — recall from H5 that TTP and HUS also produce MAHA. The distinguishing features are:
• DIC: PT and aPTT both prolonged, fibrinogen ↓, D-dimer ↑↑
• TTP: coagulation tests NORMAL (schistocytes + thrombocytopenia without PT/aPTT prolongation)
• HUS: predominantly renal failure, often follows diarrhoeal illness

Schistocytes in DIC-Associated MAHA and Fibrinolysis Comparison
SELF-CHECK
A patient with DIC has a peripheral blood film showing fragmented red cells, a platelet count of 45 × 10⁹/L, and a markedly elevated D-dimer. Which finding most specifically confirms secondary fibrinolysis rather than primary fibrinolysis in this case?
A. Elevated FDPs
B. Prolonged aPTT
C. Markedly elevated D-dimer with low fibrinogen
D. Schistocytes on peripheral smear
Reveal Answer
Answer: C. Markedly elevated D-dimer with low fibrinogen
D-dimer is a fragment generated specifically from the plasmin degradation of cross-linked fibrin (i.e., fibrin that has already been incorporated into a clot and factor XIIIa-cross-linked). A markedly elevated D-dimer combined with low fibrinogen (consumed in clot formation) confirms that clotting occurred first (generating cross-linked fibrin) and fibrinolysis followed — this is secondary fibrinolysis as seen in DIC. In primary fibrinolysis (plasminogen activator excess), FDPs are high but D-dimer is NOT elevated because primary fibrinolysis degrades fibrinogen, not already cross-linked fibrin.