Page 2 of 13
PA17.1 | Aplastic Anaemia & Bone Marrow Examination — SDL Guide (Part 2)
Clinical Features

Clinical Features of Aplastic Anaemia
Onset is insidious over weeks to months, with features driven by the three-lineage failure:
| Lineage | Effect | Symptoms |
|---|---|---|
| Erythrocytes ↓ | Anaemia | Fatigue, pallor, dyspnoea on exertion |
| Neutrophils ↓ | Immunosuppression | Recurrent bacterial/fungal infections |
| Platelets ↓ | Thrombocytopenia | Petechiae, ecchymoses, mucosal bleeding |
Physical examination:
- Pallor, petechiae, purpura
- Signs of infection
- No hepatomegaly, no splenomegaly, no lymphadenopathy — the hallmark negative finding
Camitta Severity Criteria (used to guide treatment):
- Severe aplastic anaemia (SAA): hypocellular marrow (<25%) PLUS two of three: neutrophils <0.5×10⁹/L, platelets <20×10⁹/L, reticulocytes <20×10⁹/L
- Very severe (vSAA): SAA criteria with neutrophils <0.2×10⁹/L
- Non-severe/moderate: cytopenias not meeting the above thresholds
SAA/vSAA = stem cell transplant if donor available; otherwise immunosuppression.
Peripheral Blood Findings

Peripheral Blood Findings in Aplastic Anemia
The peripheral smear in aplastic anaemia is characteristically depleted but morphologically normal:
- Pancytopenia — low RBC count, leucocyte count, and platelet count
- Normocytic-normochromic anaemia — MCV and MCHC are normal; contrast with macrocytosis in megaloblastic anaemia
- Low or absent reticulocytes (reticulocytopenia) — confirms impaired erythropoiesis; a key finding distinguishing aplasia from haemolysis
- Leucocytes: reduced in total; the differential shows relative lymphocytosis (lymphocytes are spared because they are mature, not stem-cell–derived)
- Platelets: reduced in number; those present are normal in size
- No blasts, no hypersegmented neutrophils, no teardrop cells
The absence of abnormal cells on the smear is as important as the cytopenias.

Peripheral Blood Smear Findings in Aplastic Anemia
SELF-CHECK
A 22-year-old male has Hb 6.2 g/dL, TLC 1,600/µL, platelets 18,000/µL. Peripheral smear shows normocytic-normochromic RBCs, reduced platelets, no blasts, no hypersegmented neutrophils, relative lymphocytosis. Reticulocyte count is 0.1%. What is the MOST likely diagnosis?
A. Megaloblastic anaemia
B. Aplastic anaemia
C. Acute lymphoblastic leukaemia
D. Hypersplenism
Reveal Answer
Answer: B. Aplastic anaemia
Aplastic anaemia presents with pancytopenia, normocytic-normochromic RBCs, reticulocytopenia, and NO blasts or hypersegmented neutrophils. Megaloblastic anaemia causes macrocytosis and hypersegmented neutrophils. ALL would show blasts on the smear. Hypersplenism rarely causes this degree of anaemia and typically shows splenomegaly on examination.
Differential Diagnosis
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
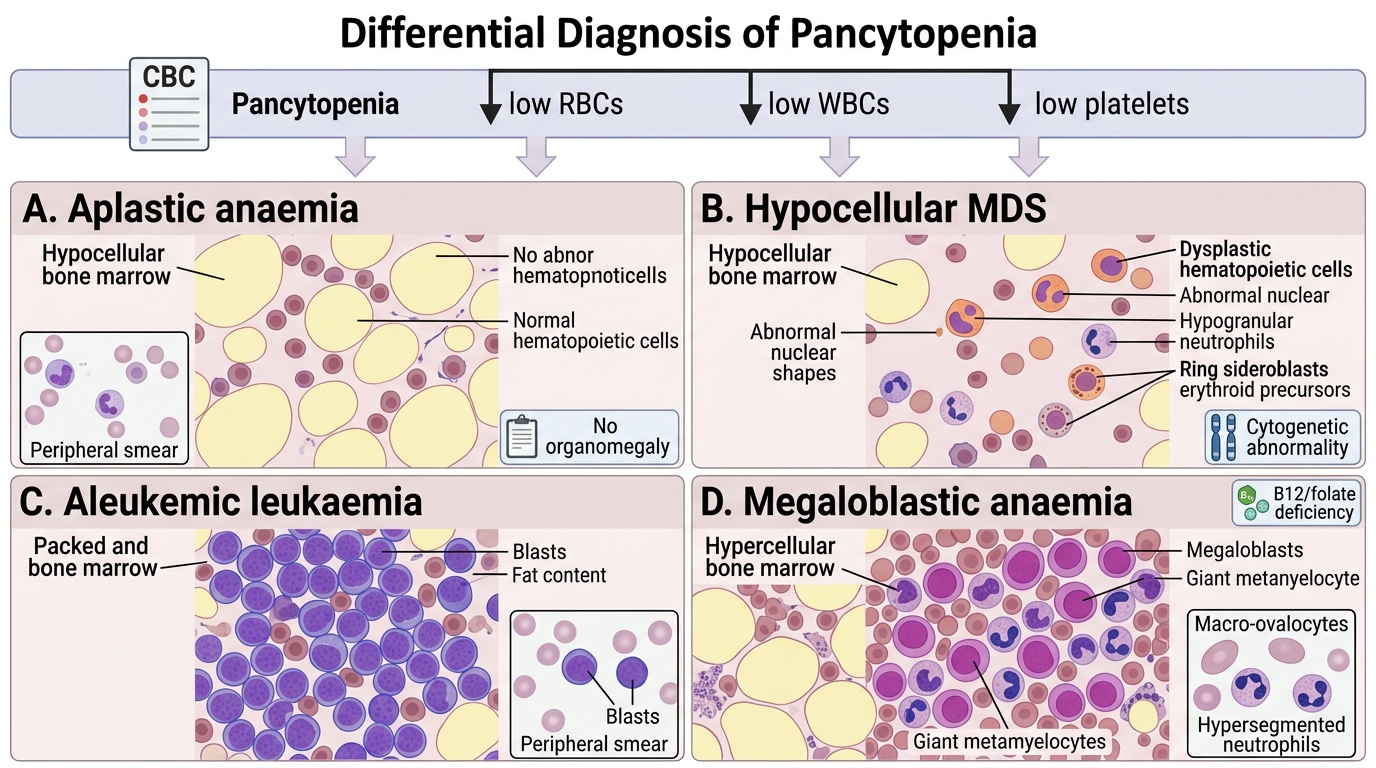
Differential Diagnosis of Pancytopenia
Pancytopenia is the common presentation; the bone marrow findings and clinical context separate the diagnoses:
| Condition | Marrow appearance | Key distinguishing features |
|---|---|---|
| Aplastic anaemia | Hypocellular, fat-replaced, no abnormal cells | No organomegaly; normal cell morphology on smear |
| Hypocellular MDS | Hypocellular but dysplastic cells present | Dysplastic neutrophils, ring sideroblasts, cytogenetic abnormalities |
| Aleukemic leukaemia | Packed with blasts; crowded | Blasts present (may be few on smear but numerous in marrow) |
| Megaloblastic anaemia | Hypercellular; megaloblasts, giant metamyelocytes | Macrocytosis, hypersegmented neutrophils; B12/folate deficiency |
| Myelofibrosis | Fibrosis on silver stain; dry tap | Tear-drop poikilocytes, splenomegaly |
Practical point: Hypocellular MDS and aplastic anaemia can be impossible to distinguish on marrow morphology alone; cytogenetics and flow cytometry are required in ambiguous cases.