Page 1 of 21
PA18.1 | Reactive Leucocytosis, Leucopenia & Lymphocytosis — SDL Guide
Learning Objectives
- State the normal ranges for total WBC count and the five-part differential.
- Enumerate the major causes of neutrophilia, neutropenia, lymphocytosis, eosinophilia, monocytosis, and basophilia.
- Describe the morphological changes of reactive neutrophilia — left shift, toxic granulation, Döhle bodies.
- Distinguish a leukaemoid reaction from chronic myeloid leukaemia using LAP score, basophilia, and clinical context.
- Recognise the atypical lymphocytes of infectious mononucleosis and distinguish reactive from neoplastic lymphocytosis.
- Apply the NAACP mnemonic to the causes of eosinophilia.
- Explain the concept of a leukoerythroblastic picture and its significance.
INSTRUCTIONS
Reactive changes in white-cell counts are the most common haematological finding in everyday clinical practice — virtually every ward patient will have a full blood count. This module equips you to read the differential count systematically, recognise the morphological clues of reaction versus malignancy, and avoid the trap of labelling a leukaemoid reaction as leukaemia. The analytical habits you build here are the scaffolding for SDL 2 and SDL 3, which take you into myeloid and lymphoid malignancies.
References
- Robbins & Kumar: Basic Pathology, 11th ed, Ch 11 (Red Cell and Bleeding Disorders) and Ch 12 (White Cell Disorders) (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed, Ch 12 (Disorders of WBCs) (textbook)
- Dacie & Lewis: Practical Haematology, 12th ed, Ch 5 (Blood Cell Morphology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old medical student presents to the college health centre with fever, sore throat, and marked fatigue for five days. Her CBC shows a WBC of 14 × 10⁹/L. The intern labels it 'leucocytosis — probably bacterial, start antibiotics.' The differential, however, shows 62% lymphocytes, many with irregular, lobulated nuclei. The senior resident stops the prescription and asks for a monospot test.
The total WBC count told one story; the differential count told another. Today you will learn to read both — and to tell reactive from malignant before a single drug is prescribed.
RECALL
Before we go further, activate what you already know:
- From Physiology (Year 1): What are the five types of white cells counted in a differential? What is the approximate normal percentage of each?
- From Biochemistry: What role do cytokines such as G-CSF and IL-6 play in haematopoiesis?
- From Anatomy: Where does granulopoiesis occur in an adult? What changes this in disease?
Jot your answers before reading on. Noticing gaps now will make the content stick better.
Normal WBC Count and the Differential
Normal WBC Count and Differential
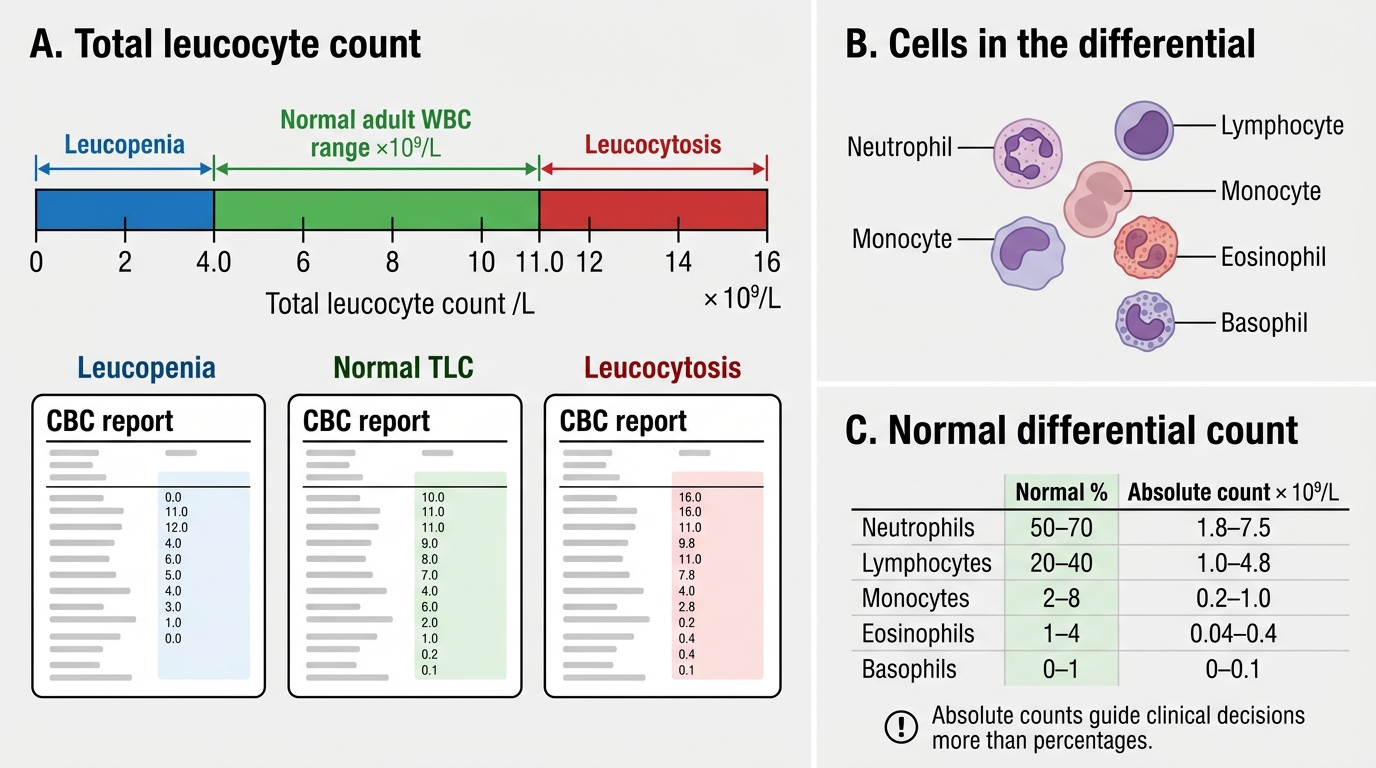
The total leucocyte count (TLC) in a healthy adult is 4.0–11.0 × 10⁹/L. Values above 11 × 10⁹/L are called leucocytosis; values below 4.0 × 10⁹/L are leucopenia.
The differential count expresses each cell type as a percentage and an absolute number. Absolute values matter more than percentages for clinical decisions.
| Cell type | Normal % | Absolute (× 10⁹/L) |
|---|---|---|
| Neutrophils | 50–70 % | 1.8–7.5 |
| Lymphocytes | 20–40 % | 1.0–4.8 |
| Monocytes | 2–8 % | 0.2–1.0 |
| Eosinophils | 1–4 % | 0.04–0.4 |
| Basophils | 0–1 % | 0–0.1 |
Relative leucocytosis — one cell type rises while others fall — can make the total count appear normal. Always assess absolute numbers.
Neutrophilia: Causes and Mechanism

Neutrophilia: Causes and Mechanisms
Neutrophilia is defined as an absolute neutrophil count > 7.5 × 10⁹/L.
Physiological causes include physical exercise, emotional stress, pregnancy (third trimester), and the neonatal period — all mediated by demargination (cells shifting from the marginating pool to circulating pool).
Pathological causes — the common clinical scenarios:
- Bacterial infections — gram-positive and gram-negative organisms trigger G-CSF and IL-8 release, accelerating marrow output and demargination. This is the most common cause worldwide.
- Inflammatory and tissue-necrotic conditions — myocardial infarction, burns, surgery, trauma, and connective tissue diseases. The same cytokine cascade drives marrow release.
- Steroid therapy and Cushing's syndrome — corticosteroids impair neutrophil margination and apoptosis, raising the circulating count without a true increase in marrow output.
- Metabolic disorders — diabetic ketoacidosis, uraemia, eclampsia, gout.
- Drugs — lithium, colony-stimulating factors (G-CSF used in chemotherapy protocols).
- Haematological — early myeloproliferative disease (CML — discussed below), polycythaemia vera.
Remember: neutrophilia is a response, not a diagnosis. The differential count morphology is your next clue.
Left Shift, Toxic Granulation, and Döhle Bodies

Left Shift and Toxic Neutrophil Changes
In severe bacterial infection or major tissue injury, the marrow releases immature granulocytes prematurely. This produces a left shift — the appearance of band neutrophils (non-segmented forms), and in more severe cases, metamyelocytes and myelocytes in the peripheral blood.
Two additional morphological markers of neutrophil stress are diagnostically important:
- Toxic granulation: enlarged, darkly staining primary (azurophil) granules in neutrophil cytoplasm. Caused by accelerated granulopoiesis with incomplete secondary granule synthesis. Seen in severe sepsis and major burns.
- Döhle bodies: pale blue-grey, round cytoplasmic inclusions composed of rough ER remnants. Accompany toxic granulation in severe infections, burns, and pregnancy. They are not Auer rods (which are malignant).
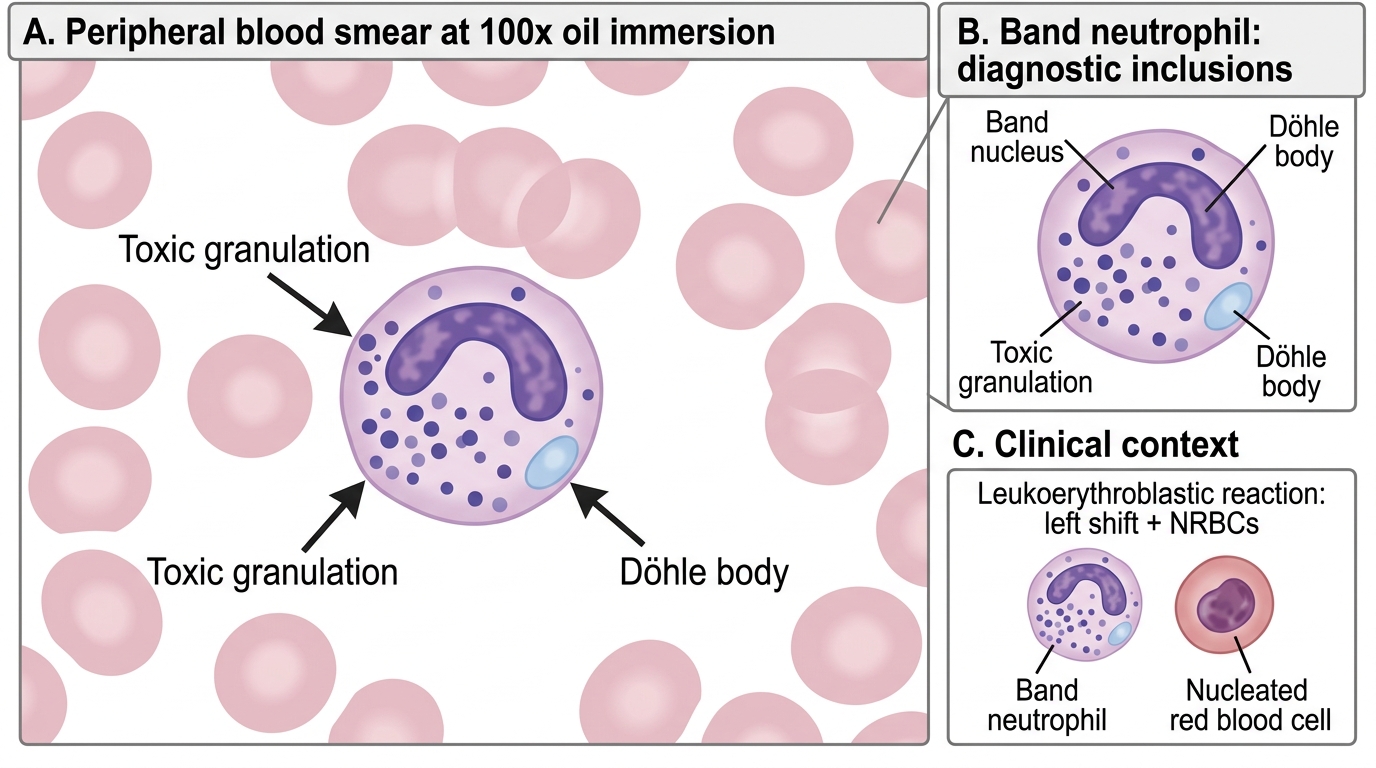
Toxic Changes in a Band Neutrophil
When left shift is accompanied by nucleated red blood cells (NRBCs) in the peripheral blood, the picture is called a leukoerythroblastic reaction — discussed separately below.