Page 2 of 21
PA18.1 | Reactive Leucocytosis, Leucopenia & Lymphocytosis — SDL Guide (Part 2)
Leukaemoid Reaction vs Chronic Myeloid Leukaemia
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
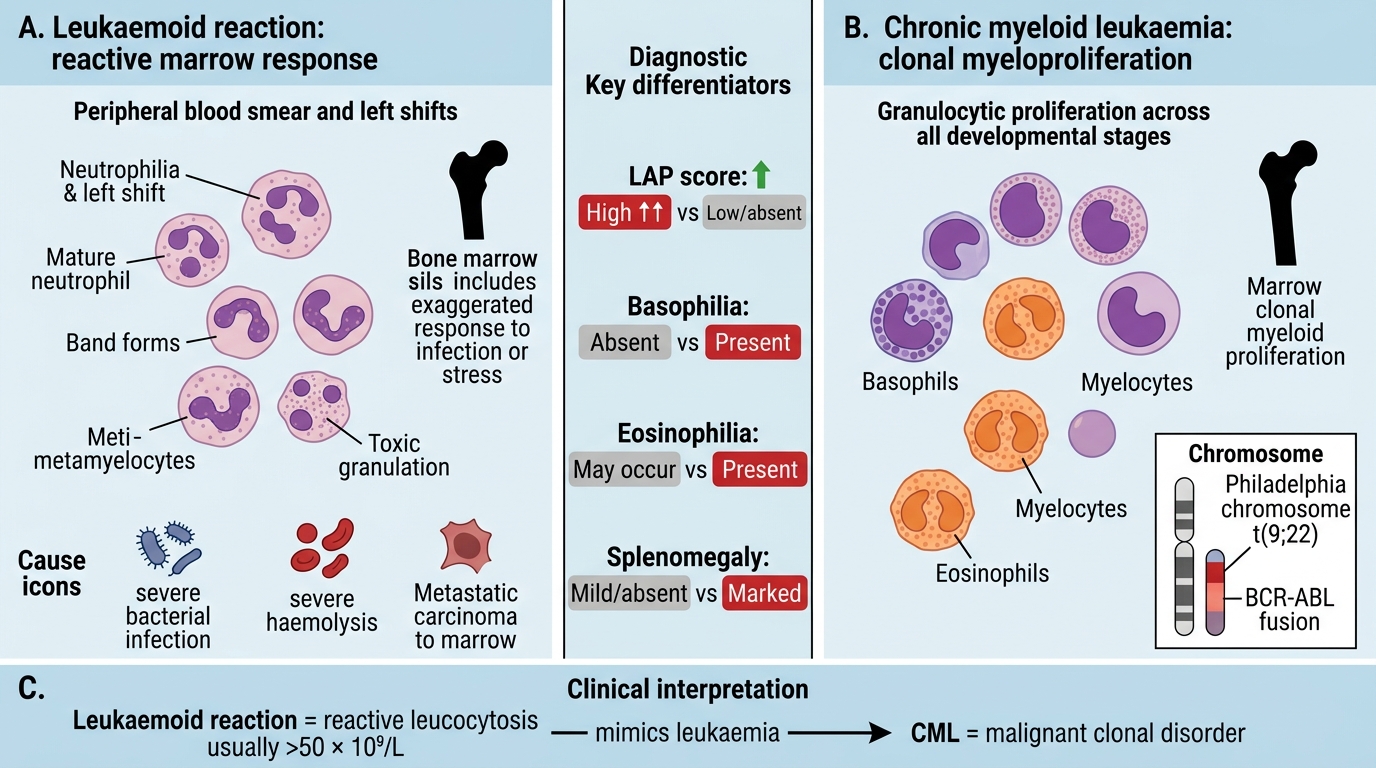
Leukaemoid Reaction vs Chronic Myeloid Leukaemia
A leukaemoid reaction is a reactive leucocytosis (usually > 50 × 10⁹/L) with a marked left shift that mimics the blood picture of leukaemia. It is not a disease itself — it is an exaggerated marrow response.
Causes: severe bacterial infections (e.g., miliary TB, severe pneumonia), severe haemolysis, metastatic carcinoma to the marrow.
Distinguishing a leukaemoid reaction from chronic myeloid leukaemia (CML) is one of the classic differential diagnoses in haematology and a favourite examination scenario:
| Feature | Leukaemoid reaction | CML |
|---|---|---|
| LAP score | High (↑↑) | Low or absent |
| Basophilia | Absent | Present (hallmark) |
| Eosinophilia | May be present | Present |
| Splenomegaly | Absent or mild | Prominent |
| Philadelphia chromosome (BCR-ABL) | Absent | Present |
| Cause | Identifiable trigger (infection, etc.) | Clonal myeloid neoplasm |
| Toxic granulation / Döhle bodies | Present | Usually absent |
The LAP (leucocyte alkaline phosphatase) score is determined by a cytochemical stain on a peripheral blood smear: 100 neutrophils are scored 0–4 based on granule staining intensity. Normal = 20–100. Leukaemoid reactions score > 100; CML scores near zero. In modern laboratories, BCR-ABL FISH or RT-PCR has replaced the LAP score, but understanding the concept remains a core competency.

Leukaemoid Reaction vs CML: Peripheral Blood Smear Comparison
SELF-CHECK
A 35-year-old woman with miliary tuberculosis has a WBC of 62 × 10⁹/L with a marked left shift. Which single investigation result best distinguishes this from CML?
A. Bone marrow biopsy showing hypercellularity
B. Peripheral blood showing basophilia > 2%
C. LAP score of 140
D. Serum LDH elevated
Reveal Answer
Answer: C. LAP score of 140
A high LAP score (> 100) is the classic marker of a leukaemoid reaction — reactive neutrophils retain their alkaline phosphatase. CML neutrophils are neoplastic clones with near-zero LAP. Basophilia in option B would actually support CML. Bone marrow hypercellularity is non-specific. LDH is non-specific.
Leukoerythroblastic Reaction

Leukoerythroblastic Reaction: A Marrow Red Flag
A leukoerythroblastic reaction (also written leukoerythroblastosis) describes the simultaneous appearance of immature white cells (myelocytes, metamyelocytes) and nucleated red blood cells (normoblasts) in the peripheral blood.
This combination signals marrow infiltration or displacement and should always prompt investigation for a serious underlying cause:
- Metastatic carcinoma to the marrow (breast, prostate, lung — the most common)
- Multiple myeloma or lymphoma with marrow involvement
- Severe haemolysis with marrow stress
- Myelofibrosis (the classic cause)
- Severe sepsis (occasionally)
Key teaching point: the leukoerythroblastic picture is not a diagnosis — it is a red flag that the bone marrow microenvironment is disrupted. A trephine biopsy is mandatory when this picture is found without an obvious cause.
Neutropenia and Agranulocytosis
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
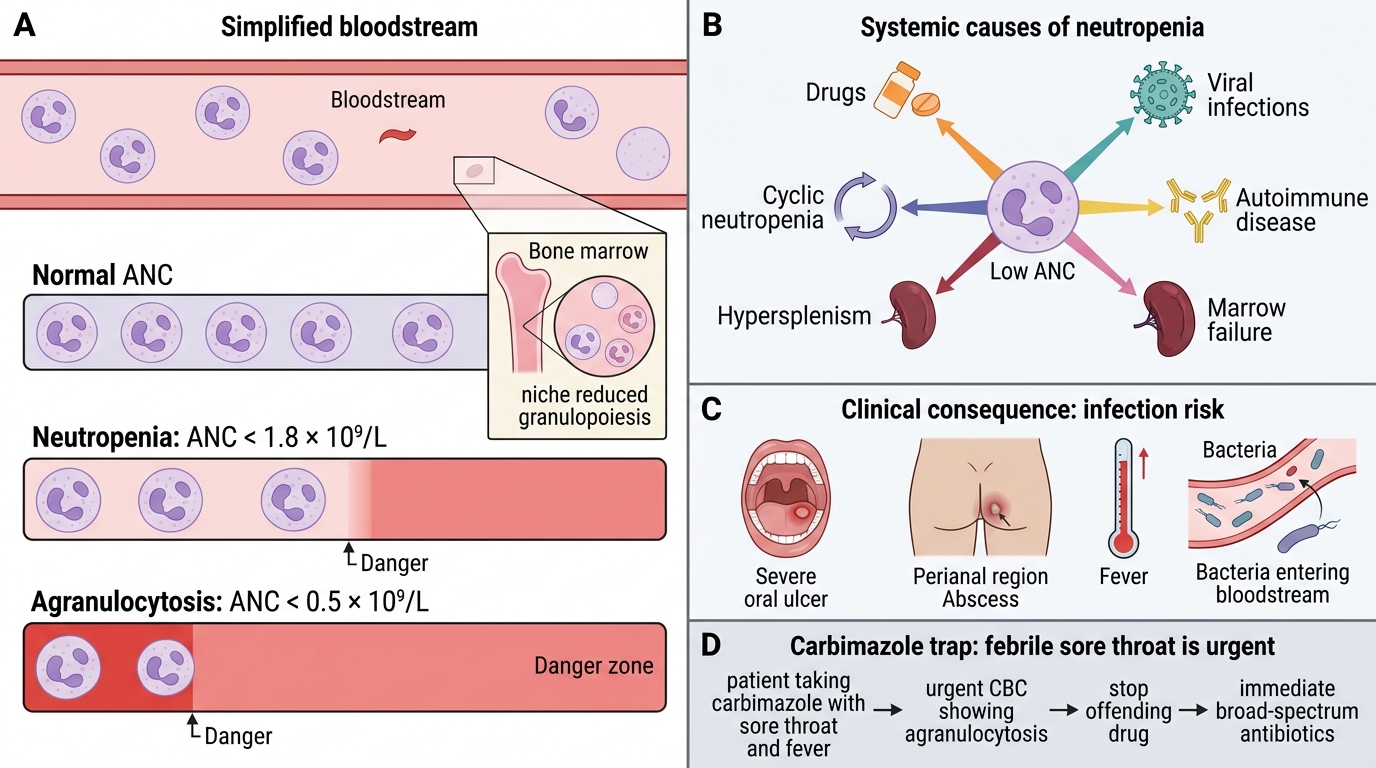
Neutropenia and Agranulocytosis: Causes and Clinical Risk
Neutropenia is an absolute neutrophil count < 1.8 × 10⁹/L. When counts fall below 0.5 × 10⁹/L the term agranulocytosis applies and life-threatening infection risk is extreme.
Causes — a systematic approach:
1. Drugs — the most important cause to recognise:
- Dose-related: cytotoxic chemotherapy (methotrexate, cyclophosphamide)
- Idiosyncratic (immune-mediated): clozapine, carbimazole, chlorpromazine, propylthiouracil, NSAIDs, co-trimoxazole
2. Viral infections — hepatitis B and C, HIV, EBV, CMV, influenza. Viruses suppress marrow progenitors and increase peripheral destruction.
3. Autoimmune — systemic lupus erythematosus, Felty syndrome (RA + splenomegaly + neutropenia). Antibodies target neutrophil surface antigens.
4. Marrow failure states — aplastic anaemia, B12/folate deficiency (maturation arrest), leukaemia replacing normal marrow.
5. Hypersplenism — spleen sequesters and destroys cells; any cause of massive splenomegaly (portal hypertension, storage diseases, lymphoma).
6. Cyclic neutropenia — rare genetic (ELANE mutations), ANC nadirs every ~21 days.
Clinical consequence: the first sign of agranulocytosis is often a severe oral ulcer or perianal abscess. Fever in a neutropenic patient is an oncological emergency requiring immediate broad-spectrum antibiotics.
CLINICAL PEARL
The carbimazole trap: a patient on carbimazole (for hyperthyroidism) presents with high fever and sore throat. The first instinct may be to attribute the fever to thyroid storm or infection. Always check the CBC first. Carbimazole-induced agranulocytosis is a serious, potentially fatal adverse effect — the WBC may be < 0.5 × 10⁹/L with no neutrophils. Stop the drug immediately, admit, and start G-CSF + antibiotics. In India, carbimazole is widely used and this complication is under-recognised.