Page 12 of 32
PA24.{2,4} | Alcoholic Liver Disease, Cirrhosis & Hepatic Failure — SDL Guide (Part 3)
Clinical Manifestations & Complications of Hepatic Failure
Clinical Manifestations & Complications of Hepatic Failure
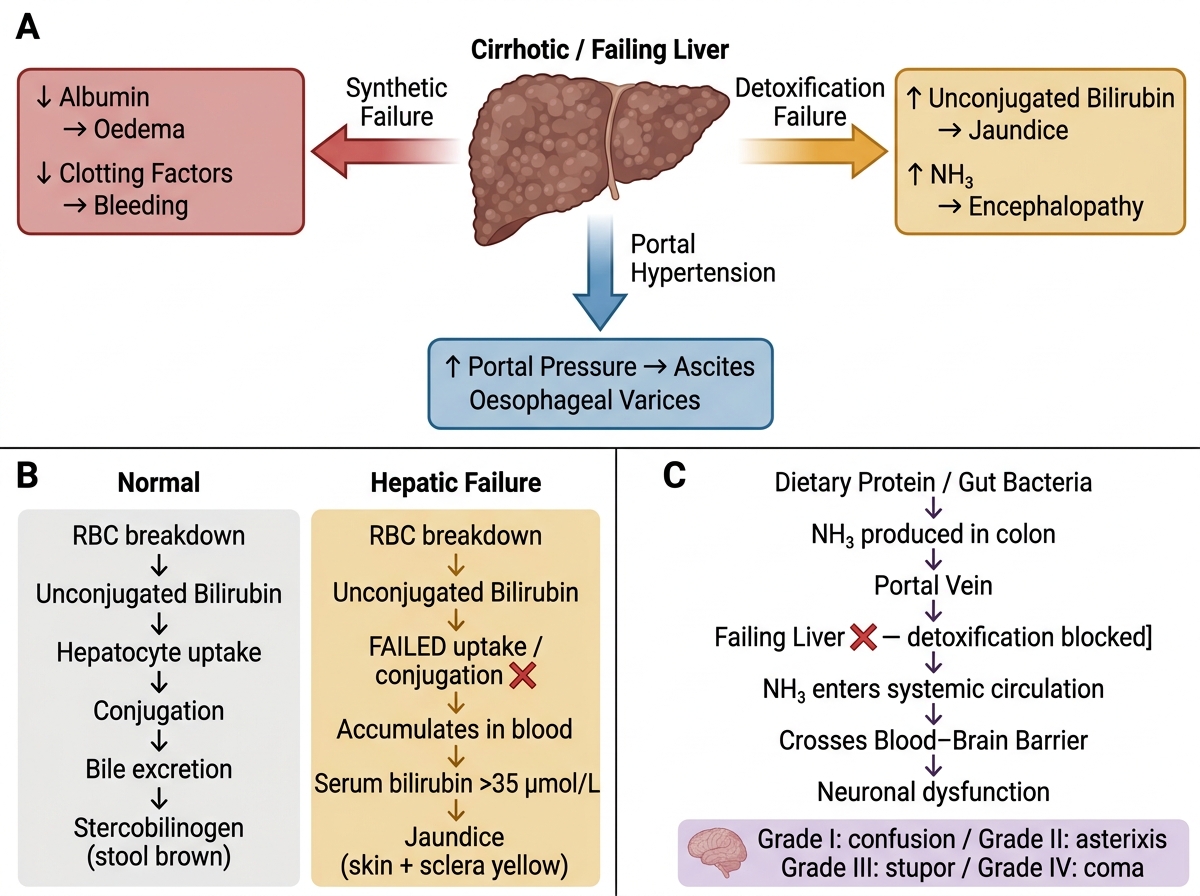
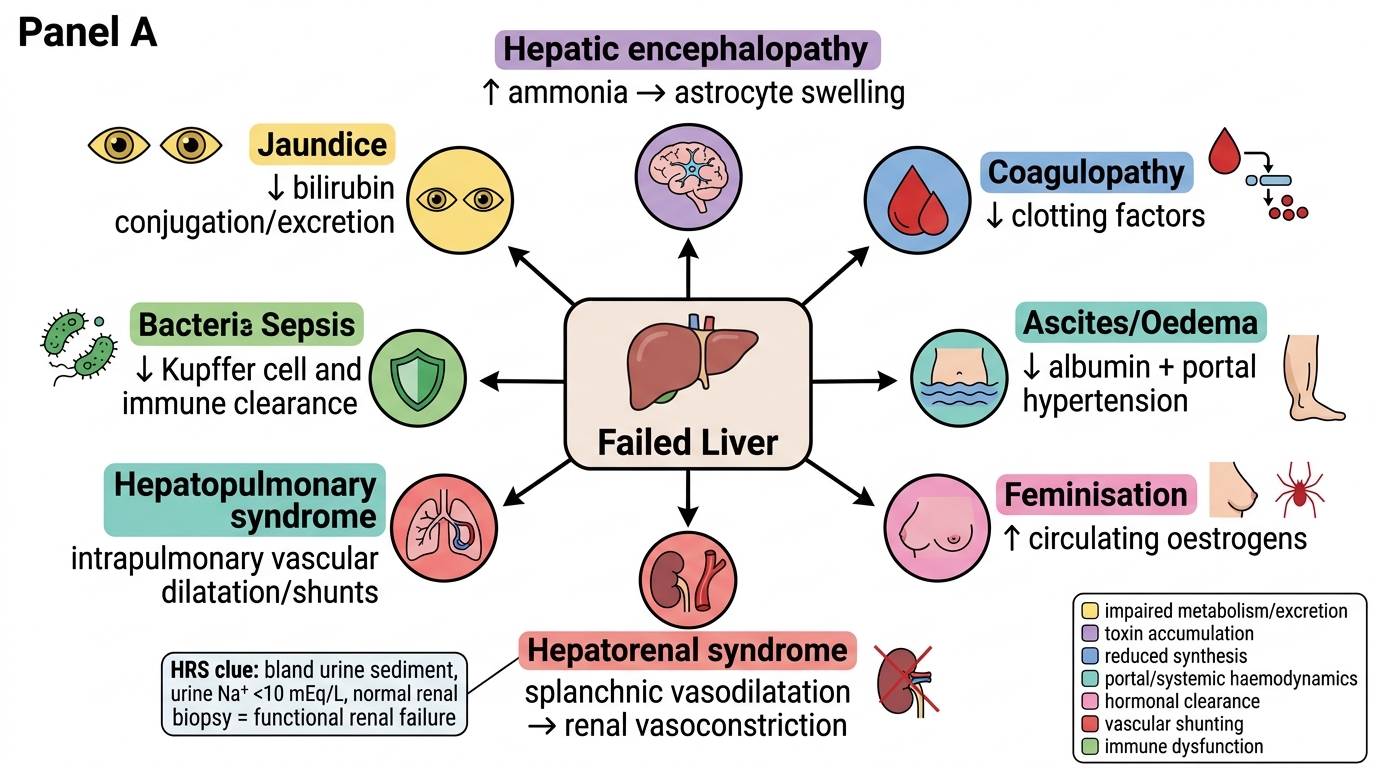
Each complication of hepatic failure has a direct mechanistic explanation:
1. Jaundice:
Failed hepatocyte uptake + conjugation of bilirubin → unconjugated hyperbilirubinaemia early; in cirrhosis, combined conjugated + unconjugated due to hepatocyte dysfunction and cholestasis. Clinically evident when serum bilirubin >35 µmol/L.
2. Hepatic Encephalopathy (HE):
Hepatic encephalopathy is a neuropsychiatric syndrome arising from accumulation of nitrogenous waste products, predominantly ammonia (NH₃), in the systemic circulation due to: (a) failed hepatic detoxification, and (b) porto-systemic shunting bypassing the liver. Ammonia crosses the blood-brain barrier → astrocyte swelling (Alzheimer type II astrocytes on histology) → cerebral oedema, altered neurotransmission. Clinical grades: Grade I (altered sleep, mild confusion) → Grade IV (coma). Asterixis (flapping tremor of outstretched hands) is the classical sign — due to involuntary lapses in sustained posture.
3. Coagulopathy:
The liver synthesises all coagulation factors except Factor VIII and vWF (endothelium-derived). In failure: ↓Factors I, II, V, VII, IX, X, XI → prolonged PT/INR, prolonged APTT → spontaneous bleeding, haematemesis from varices, petechiae. Factor VII has the shortest half-life (~6 hours) → PT/INR is the most sensitive and earliest synthetic marker of liver failure.
4. Hypoalbuminaemia → Oedema and Ascites:
Hypoalbuminaemia results from failed hepatic albumin synthesis → ↓plasma oncotic pressure → fluid transudation into interstitium → peripheral oedema and ascites. In cirrhosis, portal hypertension (↑hydrostatic pressure) acts synergistically with hypoalbuminaemia to produce massive ascites (see SDL 4 for portal hypertension mechanisms).
5. Feminisation and Spider Naevi:
The liver normally inactivates oestrogens. In hepatic failure → ↑circulating oestrogens → gynaecomastia, female hair distribution, spider naevi (dilated central arteriole with radiating vessels), palmar erythema, and testicular atrophy in males.
6. Hepatorenal Syndrome (HRS):
Hepatorenal syndrome is acute functional renal failure in a patient with severe hepatic failure or cirrhosis, in the absence of intrinsic renal disease. Mechanism: splanchnic vasodilatation (NO-mediated) → ↓effective arterial blood volume → reflex intense renal vasoconstriction → ↓GFR. Kidneys are structurally normal — they function normally if transplanted. Two types: HRS-1 (acute, rapidly progressive) and HRS-2 (chronic, slower).
7. Hepatopulmonary Syndrome:
Hepatopulmonary syndrome — intrapulmonary vascular dilatation → arteriovenous shunting → hypoxaemia. Clinically: platypnoea (dyspnoea worsened by standing) and orthodeoxia (desaturation on standing — opposite of orthopnoea). Seen in 5–30% of cirrhotic patients awaiting transplantation.
8. Sepsis and Immune Dysfunction:
The liver produces acute-phase proteins and clears portal-blood bacteria. In cirrhosis: ↓reticuloendothelial function + bacterial translocation from gut → spontaneous bacterial peritonitis (SBP) (most common in ascites), bacteraemia, fungaemia. SBP precipitates ACLF.
Complications of Hepatic Failure
SELF-CHECK
A patient with decompensated cirrhosis develops progressive renal failure. Urine sodium is <10 mEq/L, urine microscopy is bland, and renal biopsy shows no intrinsic disease. Which pathophysiological mechanism best explains this presentation?
A. IgA immune complex deposition in mesangial cells
B. Direct hepatitis C viral cytopathic effect on tubular cells
C. Splanchnic vasodilatation reducing effective arterial blood volume and triggering renal vasoconstriction
D. Aminoglycoside nephrotoxicity from empirical treatment of SBP
Reveal Answer
Answer: C. Splanchnic vasodilatation reducing effective arterial blood volume and triggering renal vasoconstriction
This is hepatorenal syndrome (HRS). Splanchnic vasodilatation (nitric oxide-mediated) in cirrhosis reduces effective arterial perfusion. Baroreceptor-driven activation of RAAS and sympathetic nervous system causes intense renal afferent arteriole vasoconstriction, reducing GFR. The key diagnostic point: blank urine sediment and normal renal biopsy confirm functional, not structural, renal failure. The kidneys will function normally if transplanted — a clinically important distinction.
Child-Pugh Score — Quantifying Hepatic Reserve
Child-Pugh Score for Hepatic Reserve
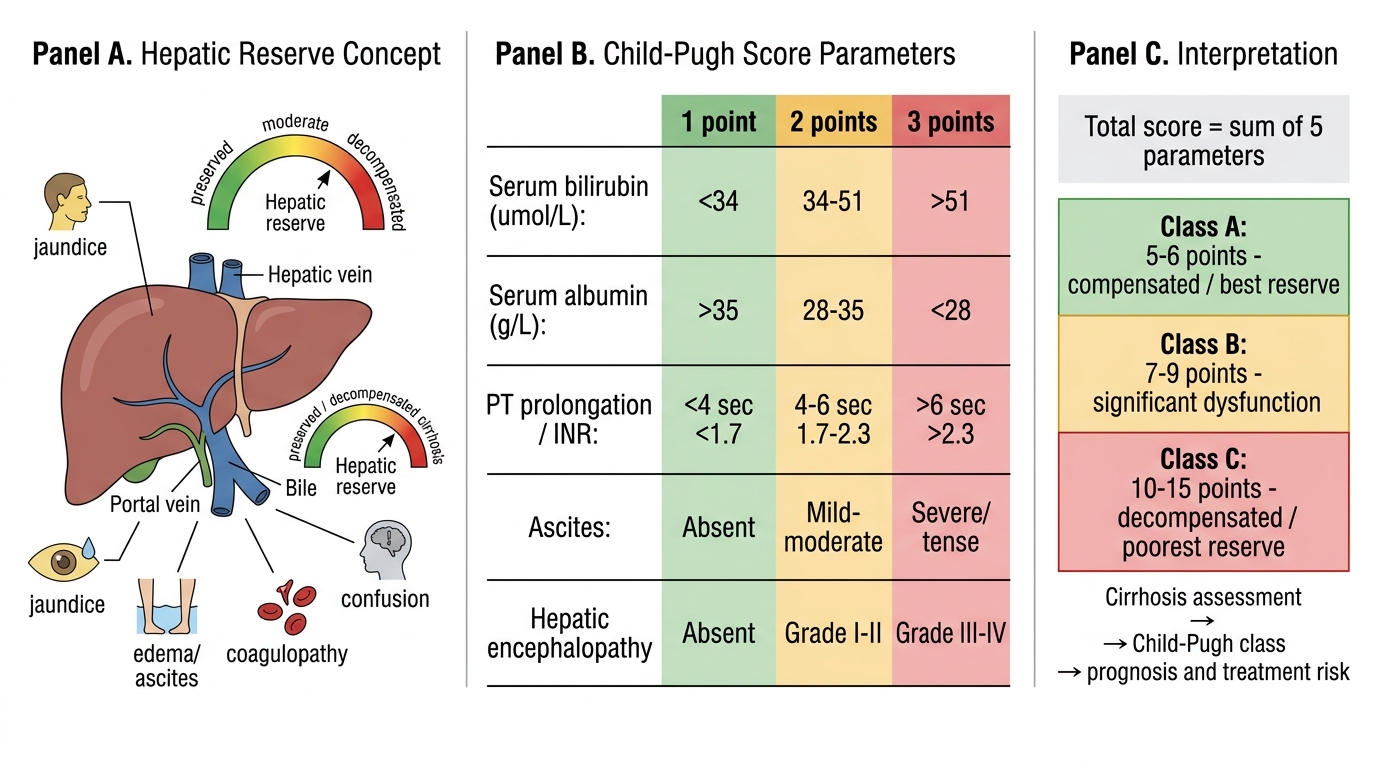
The Child-Pugh score (Child-Turcotte-Pugh) is a clinical-biochemical classification system that quantifies the severity of hepatic dysfunction and predicts short-term prognosis in cirrhosis.
Five parameters — each scored 1–3:
| Parameter | 1 point | 2 points | 3 points |
|---|---|---|---|
| Serum bilirubin (µmol/L) | <34 | 34–51 | >51 |
| Serum albumin (g/L) | >35 | 28–35 | <28 |
| PT prolongation (sec) or INR | <4 / <1.7 | 4–6 / 1.7–2.3 | >6 / >2.3 |
| Ascites | Absent | Mild–moderate | Severe/tense |
| Hepatic encephalopathy | Absent | Grade I–II | Grade III–IV |
Classification:
• Class A (5–6): Well-compensated; 1-year survival ~100%
• Class B (7–9): Significant functional compromise; 1-year survival ~80%
• Class C (10–15): Decompensated; 1-year survival ~45%
Note each parameter maps directly onto a mechanism of hepatic failure already discussed: bilirubin → conjugation failure; albumin → synthetic failure; PT → coagulation factor synthesis; ascites → portal hypertension + hypoalbuminaemia; encephalopathy → detoxification failure. The Child-Pugh score is thus a clinical application of the pathophysiology you have just learned.
SELF-CHECK
In a patient with hepatic failure, which coagulation factor is synthesised OUTSIDE the liver and would therefore be NORMAL even in severe hepatocellular disease?
A. Factor X
B. Factor II (Prothrombin)
C. Factor VII
D. Factor VIII
Reveal Answer
Answer: D. Factor VIII
Factor VIII is synthesised predominantly by vascular endothelium (and to a lesser extent by other cells including hepatic sinusoidal endothelium), not by hepatocytes. In contrast, Factors I, II, V, VII, IX, X, XI are hepatocyte-synthesised and fall in hepatic failure. Factor VII has the shortest half-life (~6 hours) and is the earliest to fall, making PT/INR the most sensitive real-time marker of hepatocellular synthetic function. The Factor VIII distinction is also clinically relevant: it helps differentiate haemophilia A from Vitamin K deficiency or hepatic disease.
CLINICAL PEARL
Asterixis is not specific to hepatic failure. While it is the classical sign of hepatic encephalopathy ("liver flap"), asterixis occurs in any metabolic encephalopathy involving elevated neurotoxins — including uraemia (renal failure), CO₂ narcosis (respiratory failure), and hypoglycaemia. The common mechanism is impaired sustained neurological inhibition of motor circuits, not ammonia specifically. In clinical practice, if you find asterixis, check liver and renal function, blood gases, and glucose — do not reflexively diagnose hepatic encephalopathy without ruling out other metabolic causes.
SELF-CHECK
A 52-year-old man has chronic alcoholic cirrhosis. His serum bilirubin is 45 µmol/L, albumin 30 g/L, INR 1.9, with mild ascites and no encephalopathy. What is his Child-Pugh class?
A. Class A (score 6)
B. Class B (score 8)
C. Class C (score 11)
D. Class B (score 7)
Reveal Answer
Answer: B. Class B (score 8)
Scoring: Bilirubin 45 µmol/L (34–51 range) = 2 pts; Albumin 30 g/L (28–35 range) = 2 pts; INR 1.9 (1.7–2.3 range) = 2 pts; Ascites mild = 2 pts; No encephalopathy = 1 pt. Total = 9 points → Child-Pugh Class B. Class A is 5–6, Class B is 7–9, Class C is 10–15. This patient has significant hepatic compromise but is not yet fully decompensated.