Page 11 of 32
PA24.{2,4} | Alcoholic Liver Disease, Cirrhosis & Hepatic Failure — SDL Guide (Part 2)
Stage 3: Alcoholic Cirrhosis
Alcoholic Cirrhosis: Fibrosis, Nodules, and Histology
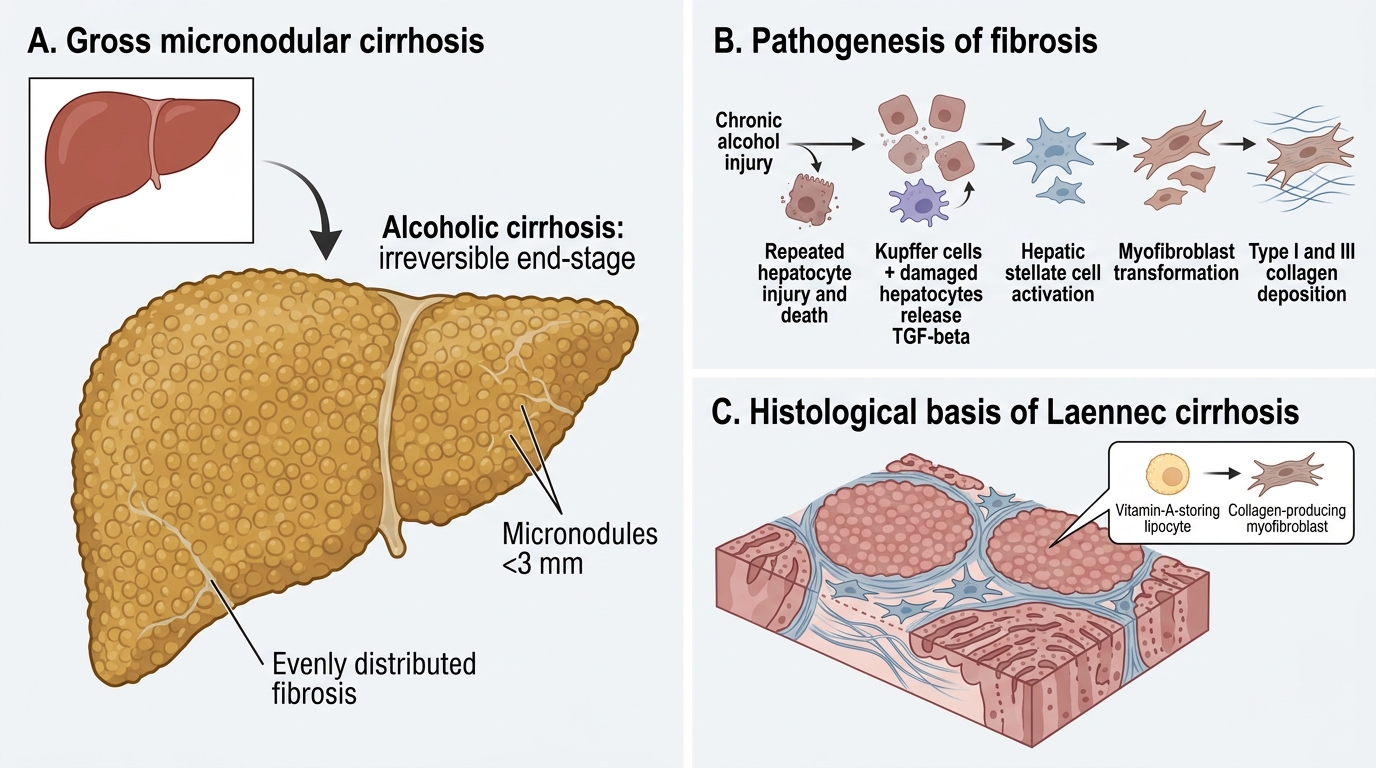
Alcoholic cirrhosis is the irreversible end-stage of alcoholic liver disease, developing in approximately 10–20% of chronic heavy drinkers after 10–20 years.
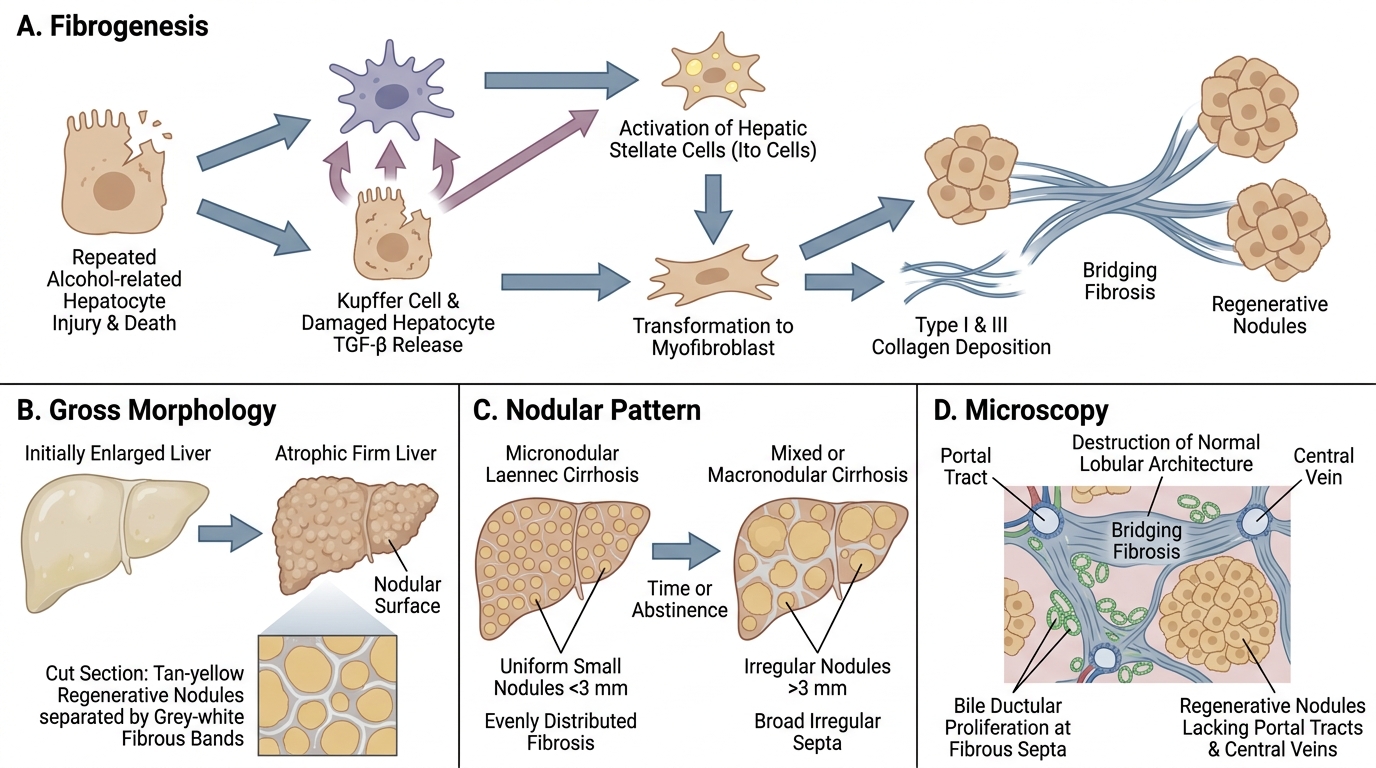
Pathogenesis of fibrosis: Repeated hepatocyte injury and death → activation of hepatic stellate cells (Ito cells) by TGF-β (released from Kupffer cells and damaged hepatocytes) → stellate cells transform from vitamin-A-storing lipocytes into myofibroblasts → synthesise type I and III collagen → progressive fibrosis.
Pattern: Alcoholic cirrhosis initially produces micronodular cirrhosis (Laennec's cirrhosis):
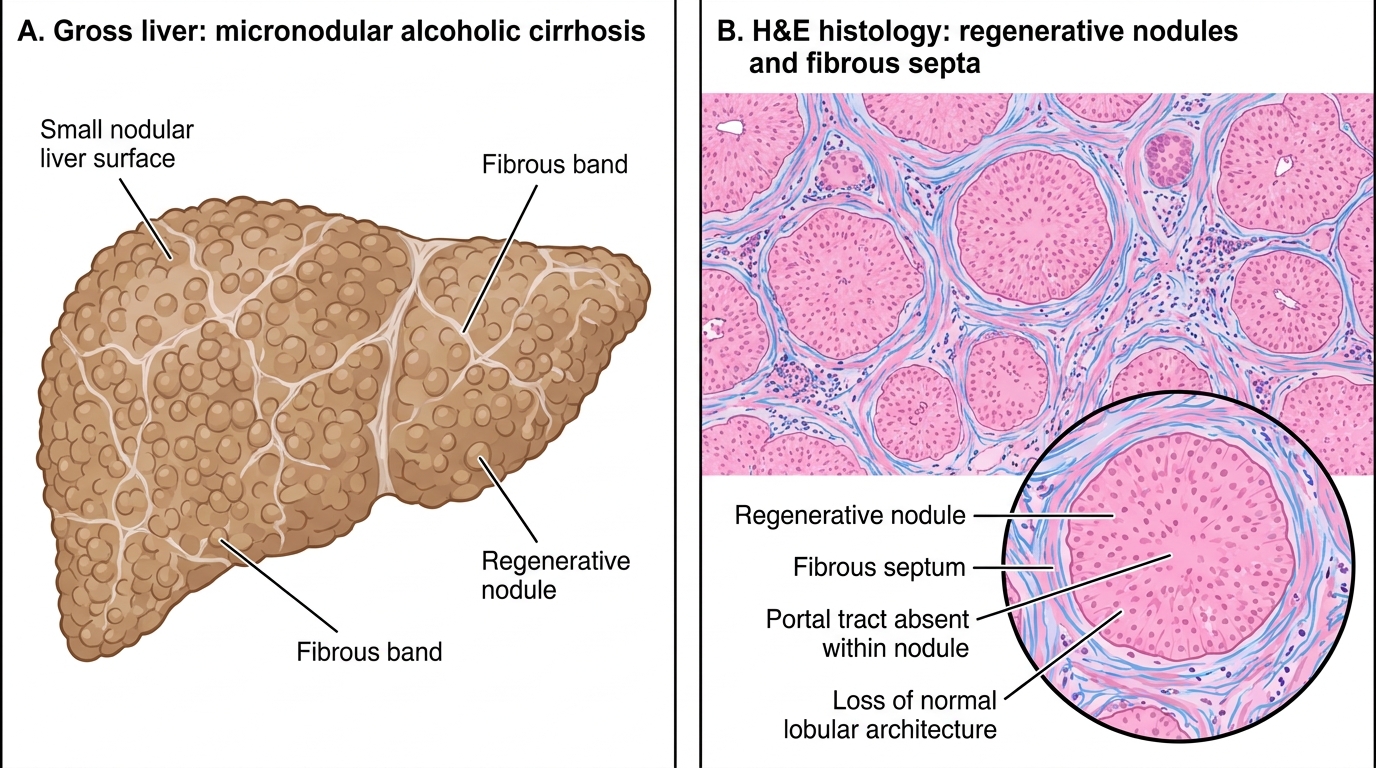
• Regenerative nodules are small, uniform, <3 mm
• Fibrosis is evenly distributed throughout the parenchyma
• Reflects uniform zonal injury from alcohol
With time or after abstinence, micronodular cirrhosis may convert to a mixed or macronodular pattern (nodules >3 mm, irregular sizes).
Gross morphology: Liver is initially enlarged, then atrophic; firm, nodular surface; cut section shows tan-yellow nodules separated by grey-white fibrous bands.
Microscopy:
• Bands of fibrous tissue (bridging fibrosis) linking portal tracts to central veins and portal tract to portal tract
• Regenerative nodules (parenchyma without portal tracts or central veins)
• Destruction of normal lobular architecture — this is the defining histological criterion of cirrhosis
• Bile ductular proliferation at fibrous septa
Irreversibility: Once bridging fibrosis with regenerative nodules is established, normal architecture cannot be restored. This is in contrast to steatosis and alcoholic hepatitis, which can regress with abstinence.
Alcoholic Cirrhosis: Gross and H&E Features
Cirrhosis: General Definition, Aetiology & Classification
Alcoholic Cirrhosis: Pathogenesis and Micronodular Pattern
Cirrhosis is defined as diffuse hepatic fibrosis with regenerative nodule formation, resulting in complete distortion of the normal lobular and vascular architecture. It is the final common pathway of many forms of chronic liver disease.
Causes — in approximate frequency in India:
| Aetiology | Notes |
|---|---|
| Alcohol (most common in urban centres) | Micronodular early |
| Chronic hepatitis B/C | Macronodular; B is dominant in India |
| Non-alcoholic steatohepatitis (NASH) | Metabolic syndrome; rising rapidly |
| Biliary cirrhosis | Primary (PBC, PSC) or secondary (biliary obstruction) |
| Haemochromatosis | Hereditary iron overload; brownish liver |
| Wilson disease | Copper accumulation; younger patients |
| Autoimmune hepatitis | Young women; ANA/SMA positive |
| Cryptogenic | ~10%; possibly NASH |
Micronodular vs Macronodular:
• Micronodular (<3 mm, uniform): alcohol, haemochromatosis, primary biliary cirrhosis, cardiac cirrhosis
• Macronodular (>3 mm, irregular): chronic viral hepatitis, Wilson disease, alpha-1-antitrypsin deficiency; higher risk of hepatocellular carcinoma
• Mixed pattern: seen in advanced or treated disease
Regardless of aetiology, once established, cirrhosis leads to the same downstream consequences: portal hypertension, hepatocellular failure, and increased risk of hepatocellular carcinoma.
CLINICAL PEARL
AST:ALT > 2:1 in alcoholic liver disease — a teachable ratio: Alcohol suppresses hepatic pyridoxal phosphate (vitamin B6), which is a cofactor required by ALT (but not AST) for synthesis. The result is disproportionately low ALT relative to AST. A ratio >2 strongly suggests alcoholic aetiology; a ratio >3 is almost diagnostic. In viral hepatitis, both enzymes rise proportionately (ratio <1). In NASH, the ratio is usually <1. This single ratio helps differentiate three of the most common causes of elevated transaminases at the bedside.
Hepatic Failure: Acute vs Chronic
Hepatic Failure: Acute vs Chronic
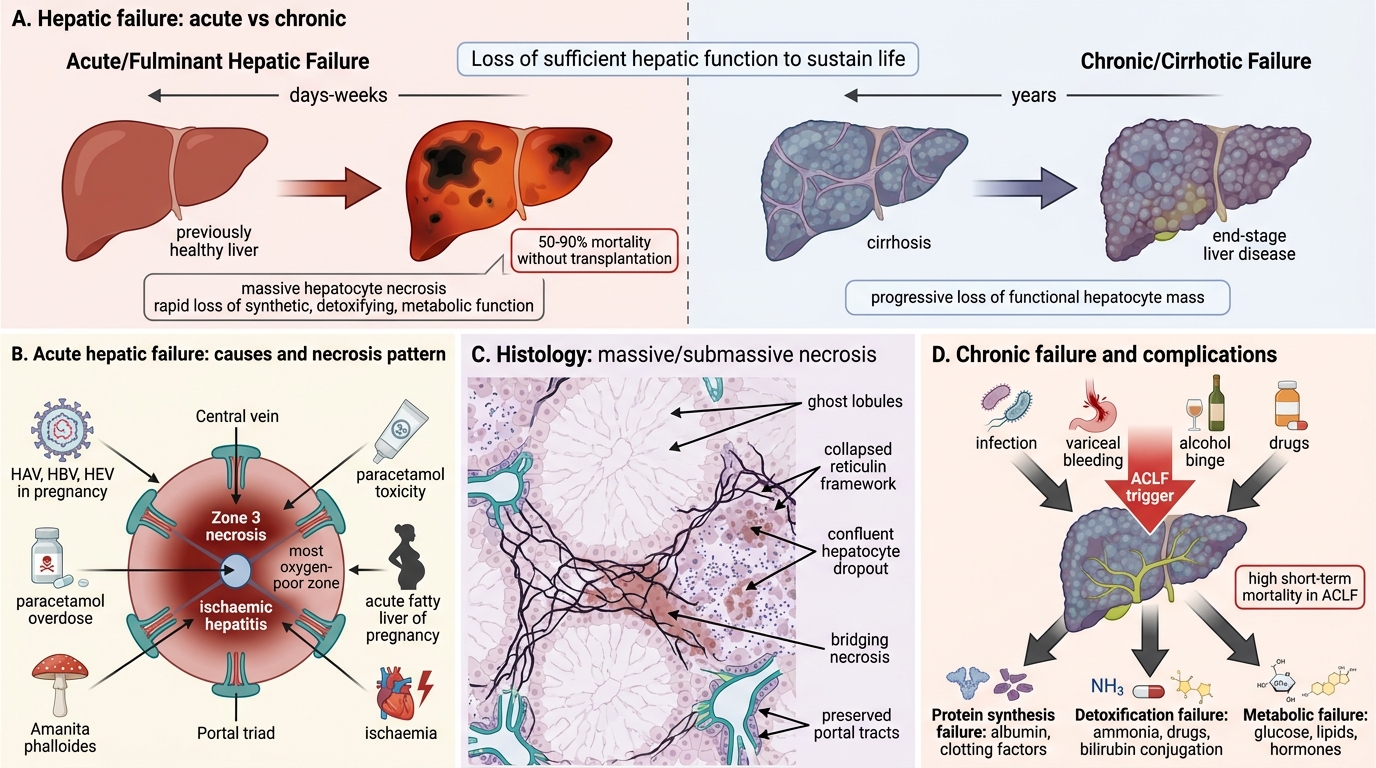
Hepatic failure is defined as loss of sufficient hepatic function — synthetic, detoxifying, metabolic — to sustain life. It presents in two distinct clinical patterns.
Acute (Fulminant) Hepatic Failure:
• Massive hepatocyte necrosis over days–weeks in a previously healthy liver
• Causes: acute viral hepatitis (HAV, HBV, HEV in pregnancy), paracetamol overdose, Amanita phalloides mushroom poisoning, acute fatty liver of pregnancy, ischaemic hepatitis
• Zone 3 necrosis (centrilobular): seen in paracetamol toxicity and ischaemia (most oxygen-poor zone)
• Massive/submassive necrosis: entire lobule or bridging necrosis across multiple lobules
• Histology: confluent hepatocyte dropout with collapsed reticulin framework, preserved portal tracts ("ghost" lobules)
• Prognosis: 50–90% mortality without liver transplantation
Chronic Hepatic Failure (Cirrhotic Failure):
• Insidious loss of function over years as functional hepatocyte mass decreases
• End-stage complication of cirrhosis from any cause
• Acute-on-chronic hepatic failure (ACLF): acute deterioration of stable cirrhosis, triggered by infection, variceal bleeding, drugs, or alcohol binge; high short-term mortality
Why so many complications? The liver performs >500 distinct functions. Its failure simultaneously disrupts:
• Protein synthesis (albumin, clotting factors)
• Detoxification (ammonia, drugs, bilirubin conjugation)
• Metabolism (glucose homeostasis, lipid metabolism, hormone inactivation)
• Haemodynamics (altered sinusoidal and splanchnic pressures)