Page 1 of 32
PA24.{1,6} | Bilirubin Metabolism, Jaundice & LFT Interpretation — SDL Guide
Learning Objectives
- Trace the complete pathway of bilirubin from haemoglobin breakdown to faecal excretion, naming the key biochemical steps and transporters at each stage.
- Classify jaundice into prehepatic, hepatic, and posthepatic types and explain the underlying mechanism for each.
- Distinguish conjugated from unconjugated hyperbilirubinaemia using clinical features, urine findings, and LFT patterns.
- Identify the four hereditary hyperbilirubinaemia syndromes (Gilbert, Crigler-Najjar, Dubin-Johnson, Rotor) and assign each to conjugated or unconjugated category.
- Interpret a liver function test panel by recognising hepatocellular, cholestatic, and prehepatic patterns.
- Interpret hepatitis B serology (HBsAg, anti-HBs, anti-HBc IgM/IgG, HBeAg) to determine acute infection, chronic infection, resolved infection, or vaccination status.
- Explain the pathophysiology of neonatal jaundice and the risk of kernicterus in preterm infants.
INSTRUCTIONS
Jaundice is one of the most common presentations in clinical medicine, and interpreting a liver function test is a core skill you will use daily in wards, OPD, and emergencies. This module builds a mechanistic map: from the molecular steps that process bilirubin, through the three sites where that processing can fail, to the pattern-recognition framework that turns a set of LFT numbers into a differential diagnosis. Hepatitis serology interpretation is woven in because viral hepatitis is the leading cause of hepatocellular jaundice in India. Everything here links to your Physiology base (bilirubin conjugation, enterohepatic circulation) and prepares you for the clinical reasoning you will need in Surgery and Medicine postings.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 18 (Liver) (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 20 (textbook)
- Chatterjea & Shinde Manual of Practical Medical Biochemistry, 12th ed. (Liver function tests) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old man presents with yellow eyes, dark urine, and pale stools for five days. His LFT shows: total bilirubin 9.2 mg/dL, direct 7.8 mg/dL, AST 68 U/L, ALT 72 U/L, ALP 480 U/L, GGT 310 U/L. His urine dipstick is positive for bilirubin, negative for urobilinogen. Before you order an ultrasound, a single question separates hepatitis from a stone in the common bile duct — and the LFT has already answered it. By the end of this module you will read that answer instantly.
WHY THIS MATTERS
Jaundice is visible at bilirubin levels above 2.5 mg/dL (scleral icterus earlier). In India, viral hepatitis and biliary obstruction from cholelithiasis together account for over 80% of jaundice cases in adults. Neonatal jaundice affects 60% of term newborns and nearly all preterms — and mismanaging it causes permanent brain damage. The LFT and viral serology panels you order in Year 2 clinics are the same panels used in ICUs and hepatology units. Getting the pattern-recognition right now makes every clinical posting faster.
RECALL
Before proceeding, confirm you can answer these from Year-1 Biochemistry and Physiology:
- What is the normal serum bilirubin range, and at what level does jaundice become clinically visible?
- Which enzyme catalyses bilirubin conjugation in hepatocytes?
- What is the enterohepatic circulation of bile?
- Name two causes of haemolytic anaemia you have already studied.
If any of these feel uncertain, spend five minutes revisiting Chatterjea & Shinde Ch 12 before continuing — the next block builds directly on this foundation.
Bilirubin Production: From Haem to Unconjugated Bilirubin
Bilirubin Production from Haem
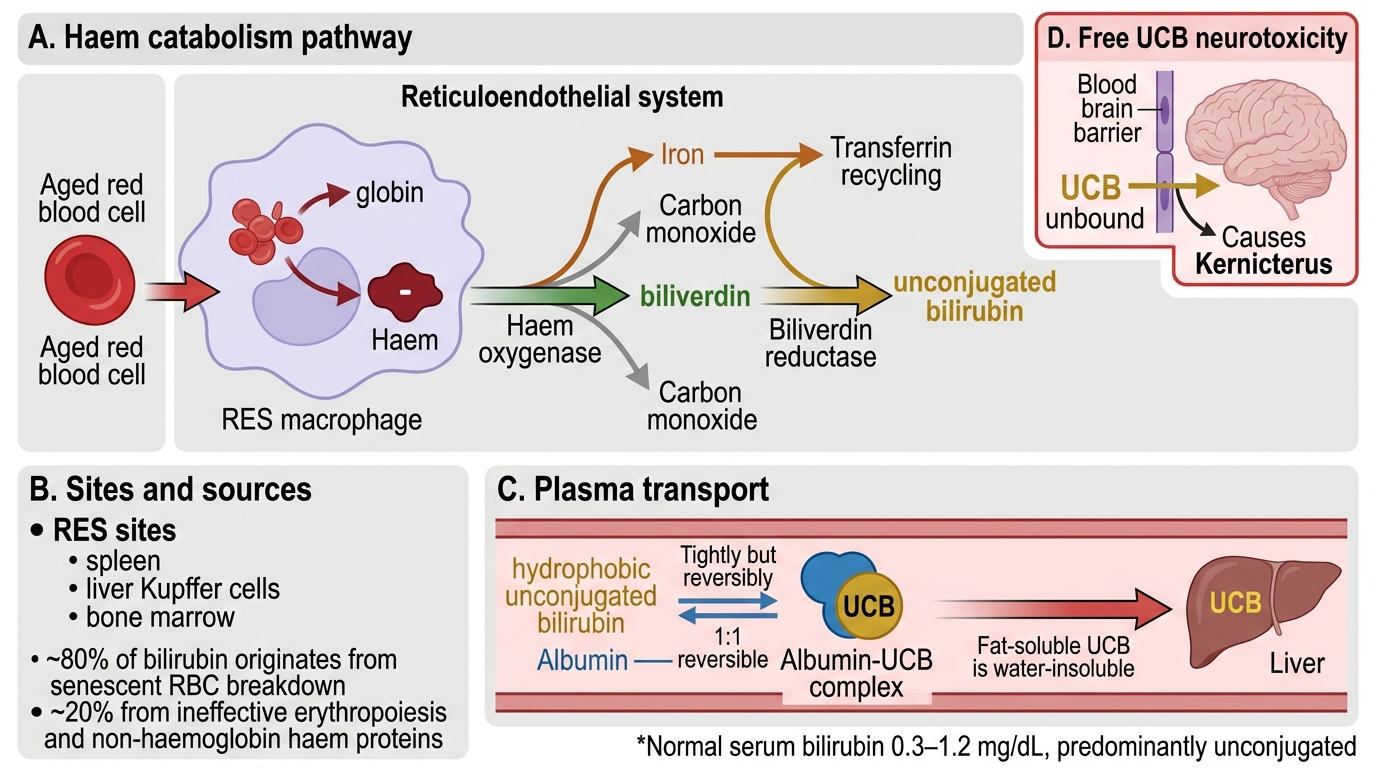
Bilirubin is the end-product of haem catabolism. Approximately 80% derives from the breakdown of senescent red blood cells (RBC lifespan ≈ 120 days) in the reticuloendothelial system (RES) — principally the spleen, liver Kupffer cells, and bone marrow. The remaining 20% comes from premature destruction of defective erythroblasts (ineffective erythropoiesis) and from turnover of non-haemoglobin haem proteins (myoglobin, cytochrome P450).
The pathway has two enzymatic steps:
1. Haem oxygenase (in RES macrophages) opens the porphyrin ring, releasing iron (recycled via transferrin) and producing biliverdin + carbon monoxide.
2. Biliverdin reductase immediately reduces biliverdin to unconjugated bilirubin (UCB), also called indirect bilirubin.
UCB is non-polar and hydrophobic (fat-soluble). It is insoluble in water and cannot be excreted in bile or urine in this form. To travel in plasma, UCB binds tightly (but reversibly) to albumin — typically as a 1:1 complex. Free (unbound) UCB is neurotoxic: it crosses the blood-brain barrier and causes kernicterus.
Normal serum bilirubin: 0.3–1.2 mg/dL, predominantly unconjugated.
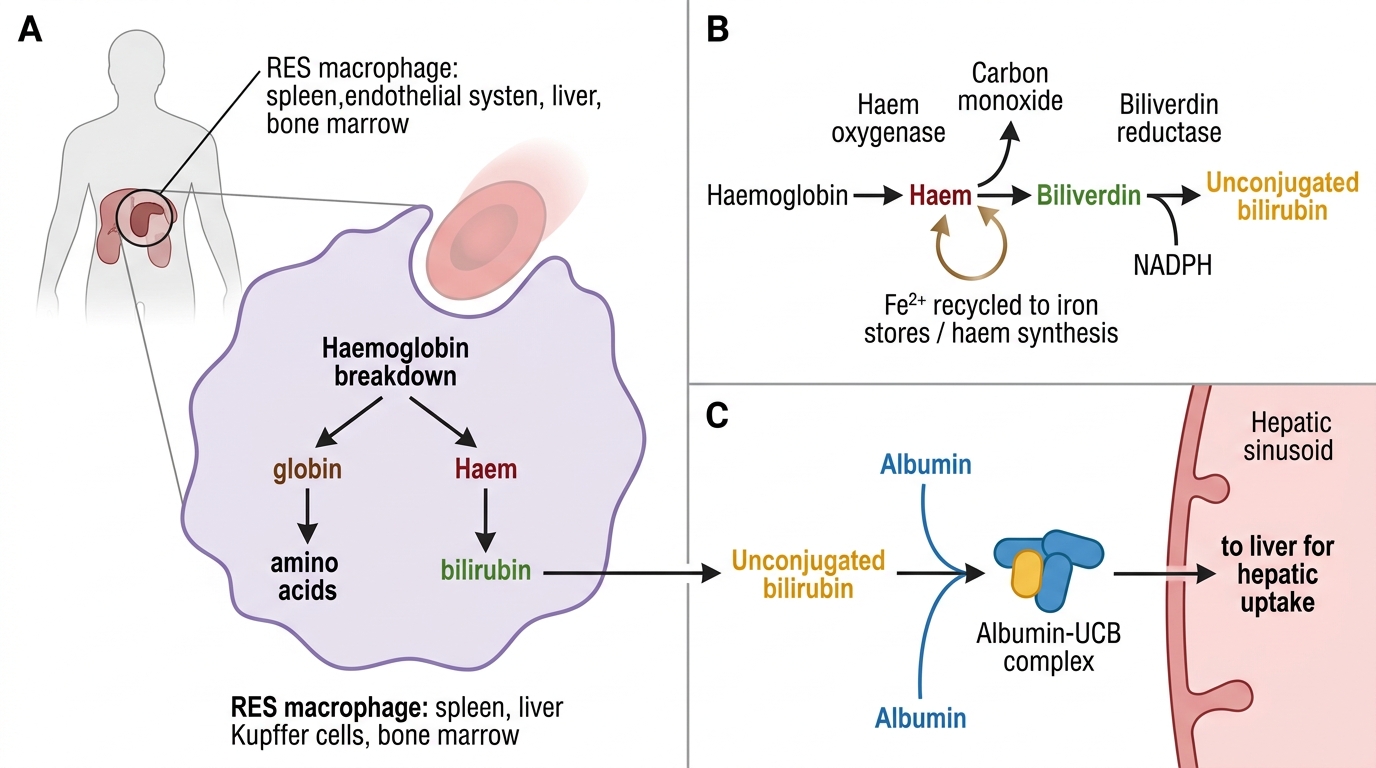
Bilirubin Production from Haemoglobin
Hepatic Uptake, Conjugation, and Excretion
Hepatic Bilirubin Uptake, Conjugation, and Excretion with Enterohepatic Circulation
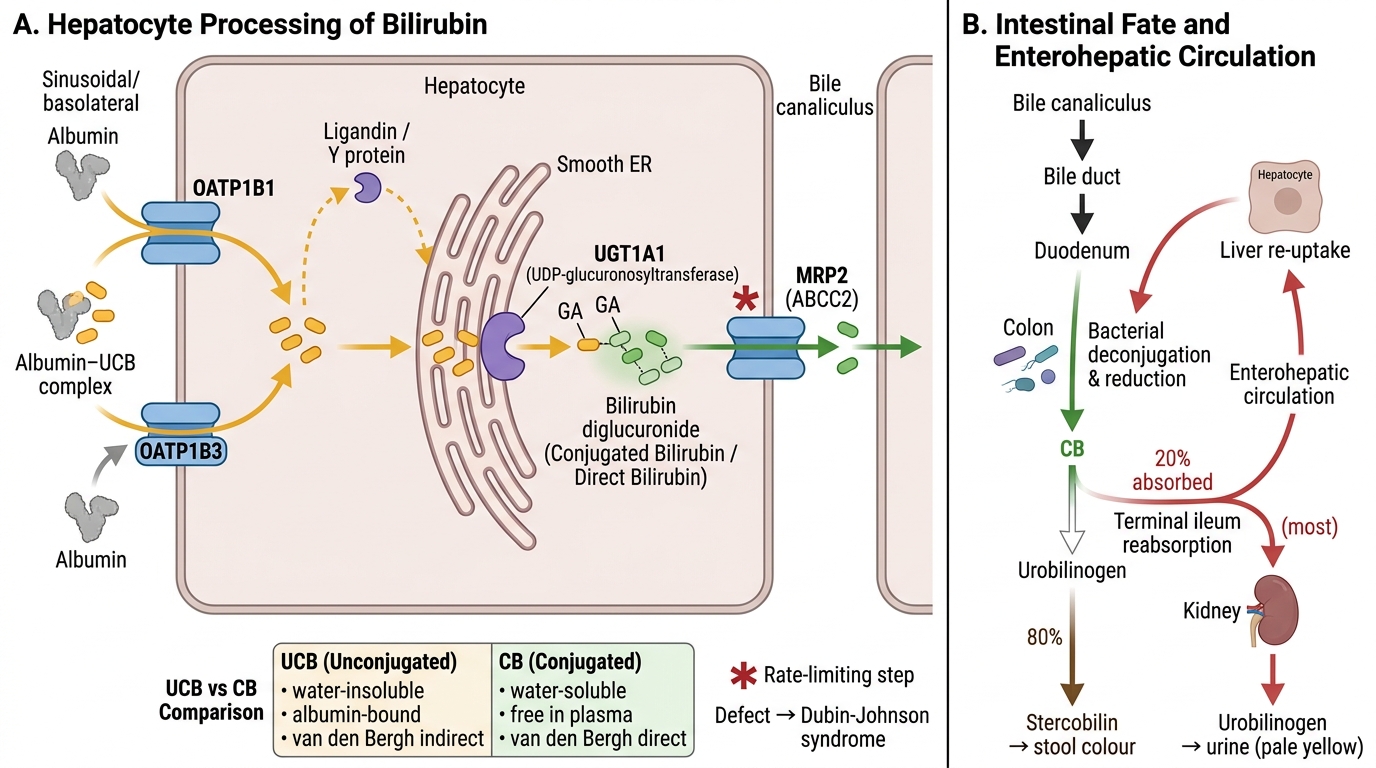
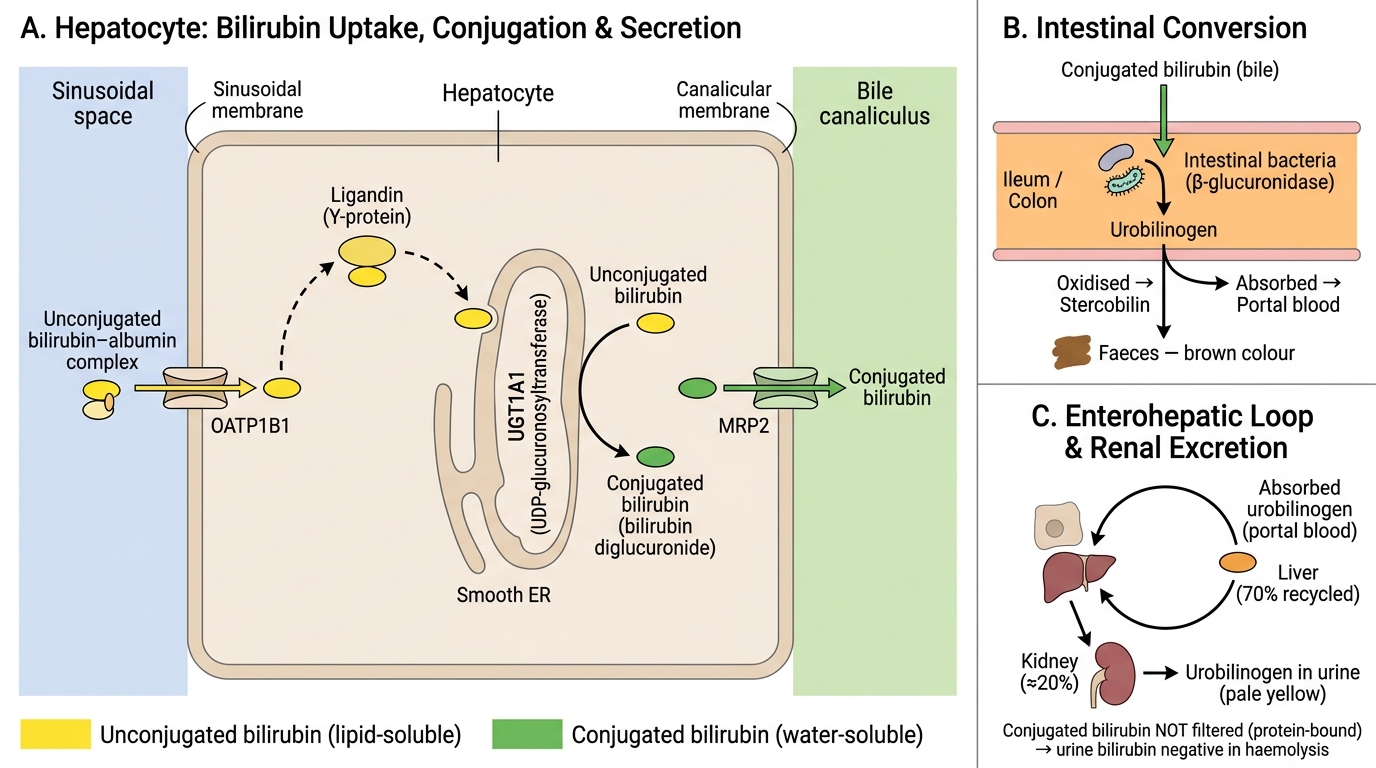
Once the albumin-UCB complex reaches the hepatic sinusoid, the bilirubin is removed from albumin and taken up by hepatocytes via OATP1B1/1B3 transporters (organic anion transporting polypeptides) on the basolateral membrane. Inside the hepatocyte, UCB is bound to intracellular carrier proteins (ligandin/Y protein) and transported to the endoplasmic reticulum.
Conjugation occurs in the smooth ER, catalysed by UDP-glucuronosyltransferase (UGT1A1). Two molecules of glucuronic acid are added to bilirubin, producing bilirubin diglucuronide — also called conjugated bilirubin or direct bilirubin. Conjugated bilirubin (CB) is:
- Water-soluble → can be excreted in bile and filtered into urine
- No longer albumin-bound → faster clearance from plasma
- Detected by the van den Bergh direct reaction (reacts without methanol)
Biliary excretion: CB is actively transported across the canalicular membrane into bile by MRP2 (multidrug resistance protein 2, also called ABCC2). This is the rate-limiting step in bilirubin clearance and the most common site of inherited transport defects (Dubin-Johnson syndrome).
In the bile duct and intestine, CB passes to the colon where colonic bacteria deconjugate and reduce it sequentially to urobilinogen (colourless) → stercobilin (brown — normal stool colour).
Enterohepatic circulation: ~20% of urobilinogen is reabsorbed from the terminal ileum and colon into portal blood. The liver re-excretes most of it into bile; a small fraction (~1%) escapes into systemic circulation and is excreted by the kidneys as urinary urobilinogen (normal: trace amounts detectable).
Hepatic Bilirubin Metabolism: Molecular Transporters, Conjugation, and Enterohepatic Circulation
SELF-CHECK
A 22-year-old medical student notices mild yellow tinge in her sclera after fasting for 24 hours during examination week. Her bilirubin is 2.8 mg/dL, predominantly unconjugated. LFTs are otherwise normal. Urine bilirubin: negative. Urine urobilinogen: normal. Which enzyme is most likely functionally reduced in this patient?
A. Haem oxygenase
B. Biliverdin reductase
C. UDP-glucuronosyltransferase (UGT1A1)
D. MRP2 canalicular transporter
Reveal Answer
Answer: C. UDP-glucuronosyltransferase (UGT1A1)
This is Gilbert syndrome — a benign, common (5–8% population) variant with reduced UGT1A1 activity (≈30% of normal). Fasting, stress, and intercurrent illness precipitate mild unconjugated hyperbilirubinaemia. Because conjugation is reduced but not absent, and because MRP2 is intact, conjugated bilirubin does not accumulate — so urine bilirubin is negative. Haem oxygenase and biliverdin reductase are upstream of the defect and are normal in Gilbert syndrome.
Jaundice: Definition, Detection, and Classification
Jaundice: Detection and Mechanistic Classification
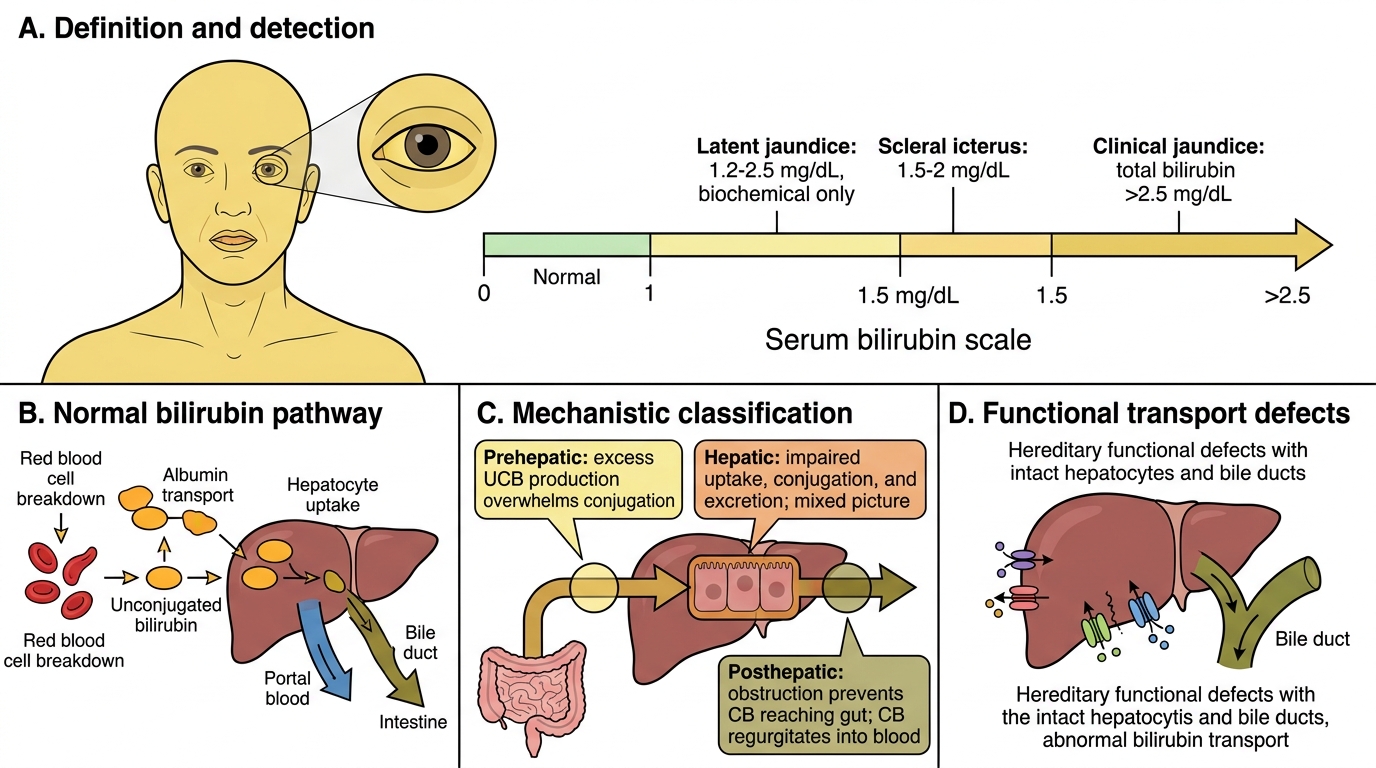
Jaundice (icterus) is the yellow discolouration of skin, sclerae, and mucous membranes due to elevated serum bilirubin. It becomes clinically detectable when total bilirubin exceeds 2.5 mg/dL (scleral icterus at 1.5–2 mg/dL, as the sclera has high elastin with strong bilirubin affinity).
Latent jaundice: 1.2–2.5 mg/dL — biochemical, no visible staining.
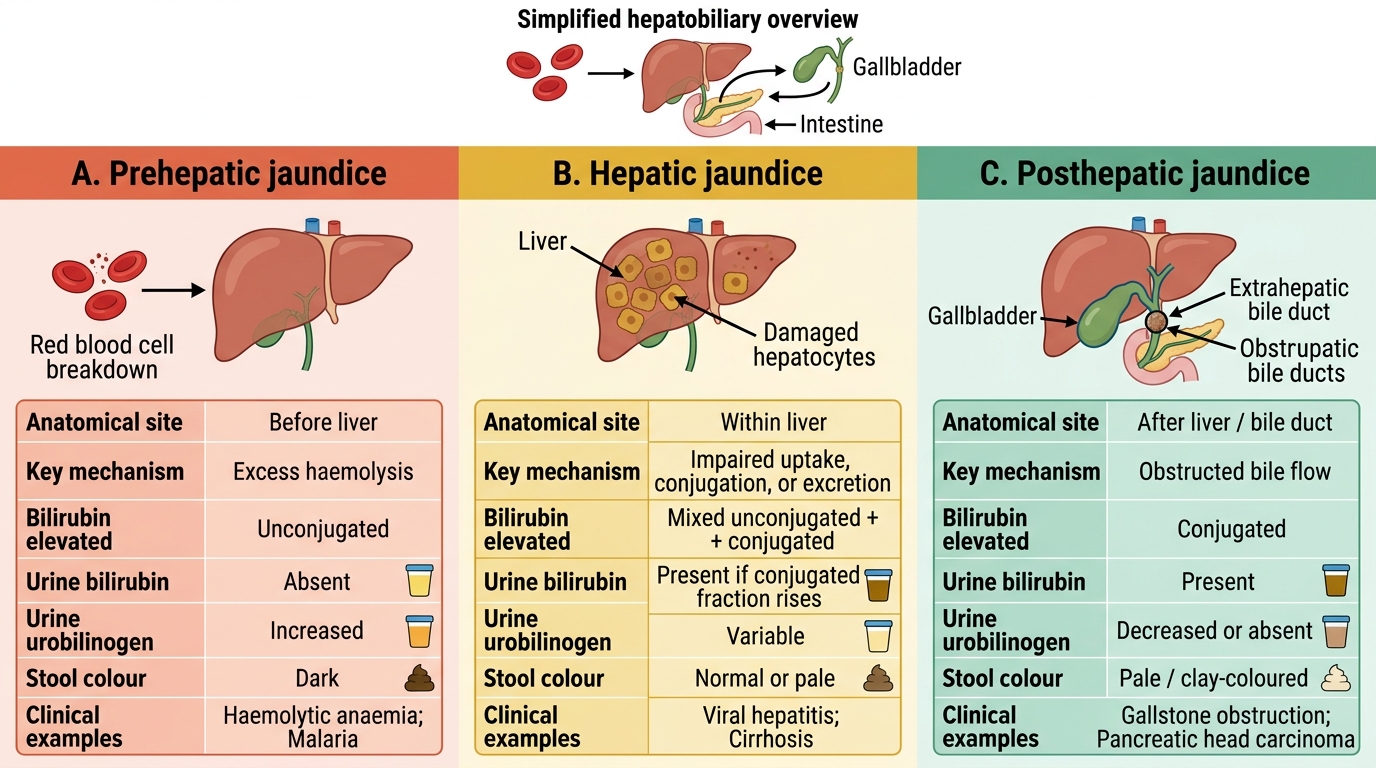
Mechanistic classification (the framework used in clinical reasoning):
| Type | Site of problem | Mechanism |
|---|---|---|
| Prehepatic | Before liver | Excess UCB production (haemolysis, ineffective erythropoiesis) overwhelms hepatic conjugation capacity |
| Hepatic | In liver cells | Hepatocellular damage impairs uptake, conjugation, AND excretion → mixed picture |
| Posthepatic | Bile ducts (extra- or intrahepatic) | Obstruction prevents CB from reaching gut → CB regurgitates into blood |
A fourth mechanistic category — functional/transport defects — covers hereditary syndromes where the bile ducts and hepatocytes are structurally intact but specific transporters or enzymes are deficient.
Classification of Jaundice