Page 2 of 32
PA24.{1,6} | Bilirubin Metabolism, Jaundice & LFT Interpretation — SDL Guide (Part 2)
Prehepatic Jaundice: Haemolytic Mechanisms
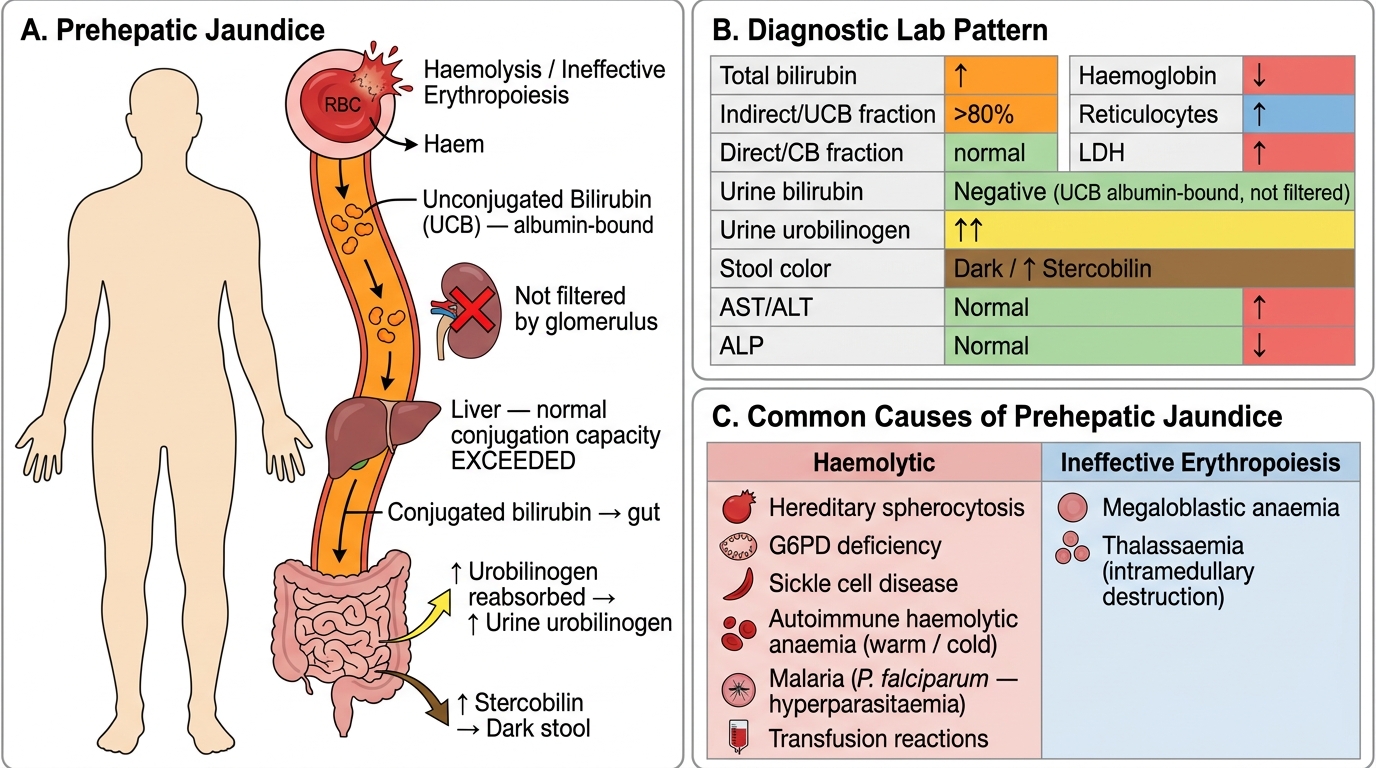
Prehepatic Jaundice: Mechanism, Lab Pattern, and Causes
When RBC destruction accelerates (haemolysis) or erythropoiesis is ineffective, bilirubin production exceeds the conjugation and secretory capacity of normal hepatocytes. The excess remains as unconjugated bilirubin.
Key features of prehepatic jaundice:
- ↑ Total bilirubin, predominantly unconjugated (indirect fraction >80%)
- Urine bilirubin: negative (UCB is albumin-bound; not filtered by the glomerulus)
- Urine urobilinogen: ↑↑ (more CB reaches gut → more urobilinogen formed → more absorbed → more excreted in urine)
- Stool: dark (↑ stercobilin)
- LFT: transaminases normal (no hepatocyte damage), ALP normal
- Blood: ↑ reticulocytes, ↓ haemoglobin, ↑ LDH, ↓ haptoglobin, +/− anaemia
Common causes:
- Hereditary spherocytosis, G6PD deficiency, sickle cell disease
- Autoimmune haemolytic anaemia (warm/cold antibody)
- Malaria (Plasmodium falciparum — hyperparasitaemia → massive haemolysis)
- Transfusion reactions
- Ineffective erythropoiesis: megaloblastic anaemia, thalassaemia (intramedullary destruction)
Hepatic Jaundice: Hepatocellular Injury
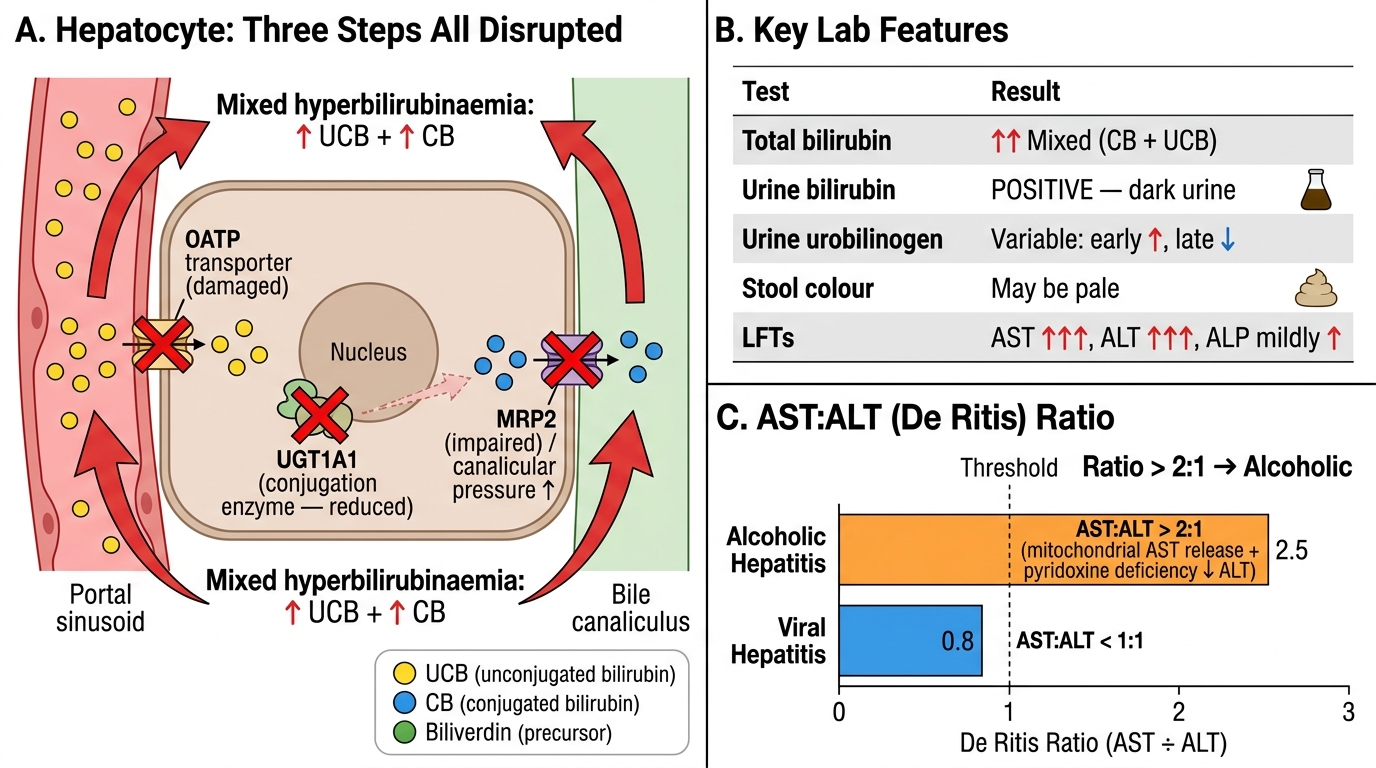
Hepatic (Hepatocellular) Jaundice: Pathophysiology, Lab Pattern, and Clinical Discriminators
Hepatocellular damage disrupts all three hepatic bilirubin-handling steps simultaneously: uptake (damaged OATP transporters), conjugation (UGT1A1 reduced), and canalicular excretion (MRP2 impaired or canalicular pressure raised by hepatocyte swelling). The result is a mixed hyperbilirubinaemia — both conjugated and unconjugated fractions rise.
Key features of hepatic (hepatocellular) jaundice:
- ↑ Total bilirubin, mixed (both fractions elevated; CB may dominate in severe disease)
- Urine bilirubin: positive (CB is water-soluble and filtered by glomerulus → dark urine)
- Urine urobilinogen: variable (early ↑, late ↓ as liver fails to extract reabsorbed urobilinogen)
- Stool: may be pale (if canalicular excretion severely impaired)
- LFT: markedly ↑ AST and ALT (hepatocyte necrosis → cytosolic enzyme release), ALP mildly to moderately raised
- Synthetic markers: ↓ albumin (chronic), ↑ PT/INR (acute or chronic)
Common causes:
- Viral hepatitis (A, B, C, D, E)
- Alcoholic hepatitis
- Drug-induced liver injury (DILI): paracetamol, anti-TB drugs (isoniazid, rifampicin, pyrazinamide)
- Leptospirosis (Weil disease)
- Autoimmune hepatitis
- Wilson disease (in young patients)
CLINICAL PEARL
The AST:ALT ratio (De Ritis ratio) is a quick discriminator: ratio >2:1 strongly suggests alcoholic hepatitis (mitochondrial AST release + relative pyridoxine deficiency lowering ALT synthesis). Viral hepatitis typically gives AST:ALT ≈1:1 or ALT > AST. However, in advanced cirrhosis of any cause, the ratio may rise as functional hepatocyte mass falls — so interpret in context, not in isolation.
Posthepatic (Obstructive) Jaundice
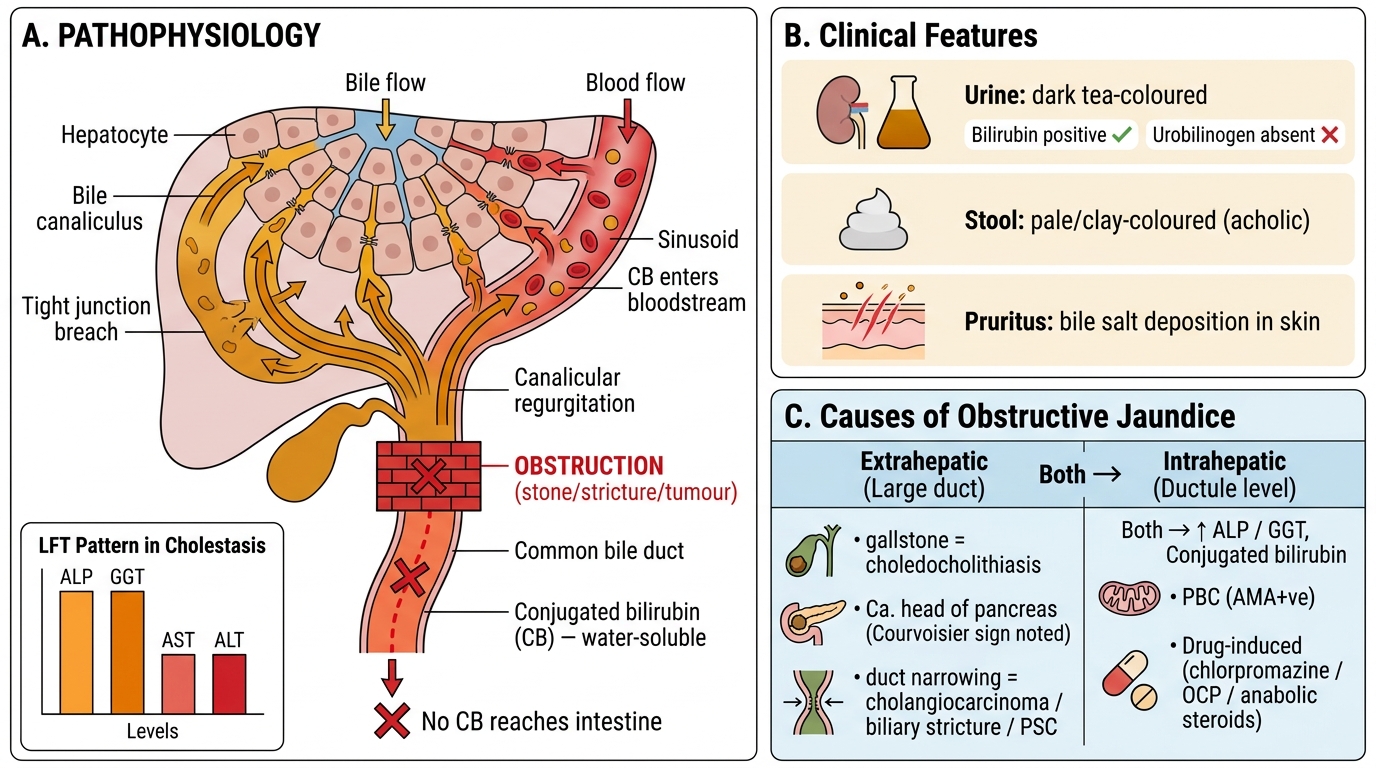
Posthepatic (Obstructive) Jaundice — Pathophysiology, Clinical Features, and Causes
When bile flow is obstructed — whether in the large extrahepatic ducts or in intrahepatic ductules — conjugated bilirubin cannot reach the intestine. It backs up into hepatocyte canaliculi, crosses the tight junctions, and regurgitates into the sinusoidal blood. Because CB is water-soluble, it freely passes into urine.
Key features of posthepatic (obstructive/cholestatic) jaundice:
- ↑ Total bilirubin, predominantly conjugated (direct fraction >50%, often >80%)
- Urine bilirubin: strongly positive → dark 'tea-coloured' urine
- Urine urobilinogen: absent or very low (no CB reaches gut, so no urobilinogen forms)
- Stool: pale/clay-coloured (acholic stools — stercobilin absent)
- Pruritus (bile salt deposition in skin — a key clinical pointer)
- LFT: markedly ↑ ALP and GGT (synthesised by biliary epithelium and released in response to pressure), transaminases mildly to moderately elevated (secondary hepatocyte injury)
Extrahepatic obstruction (large duct):
- Choledocholithiasis (most common in adults — fluctuating jaundice, colicky pain)
- Carcinoma head of pancreas (painless progressive jaundice — Courvoisier sign)
- Cholangiocarcinoma
- Biliary stricture post-surgery or primary sclerosing cholangitis (PSC)
Intrahepatic cholestasis (bile ductule level):
- Primary biliary cholangitis (PBC — AMA positive, middle-aged women)
- Drug-induced cholestasis: chlorpromazine, oral contraceptives, anabolic steroids
- Intrahepatic cholestasis of pregnancy
SELF-CHECK
A 55-year-old woman presents with progressive jaundice for three weeks, pale stools, dark urine, and pruritus. She has no fever, no pain. On examination a non-tender palpable gallbladder is felt (Courvoisier sign). LFT shows total bilirubin 14 mg/dL (direct 12), ALP 620 U/L, GGT 480 U/L, AST 88 U/L, ALT 76 U/L. Which urine finding is most consistent?
A. Urine bilirubin negative, urobilinogen strongly positive
B. Urine bilirubin positive, urobilinogen absent
C. Urine bilirubin negative, urobilinogen absent
D. Urine bilirubin positive, urobilinogen strongly positive
Reveal Answer
Answer: B. Urine bilirubin positive, urobilinogen absent
This is classic posthepatic/obstructive jaundice (carcinoma head of pancreas). Conjugated bilirubin is water-soluble and freely filtered → urine bilirubin is strongly positive (dark urine). Because no CB reaches the intestine, no urobilinogen is formed by colonic bacteria → urobilinogen is absent (not elevated). Option A describes prehepatic jaundice. Option C would require both a non-conjugating liver AND no obstruction — does not match. Option D (both positive) would be seen in severe hepatocellular disease with partial obstruction.