Page 4 of 32
PA24.{1,6} | Bilirubin Metabolism, Jaundice & LFT Interpretation — SDL Guide (Part 4)
Viral Hepatitis Serology: Hepatitis B Window Periods
Hepatitis B Serology: Markers, Window Period, and Clinical Interpretation
Hepatitis B serology interpretation is a high-yield clinical skill with direct implications for diagnosis, treatment decisions, and post-exposure management. The key markers are:
| Marker | What it is | What elevation means |
|---|---|---|
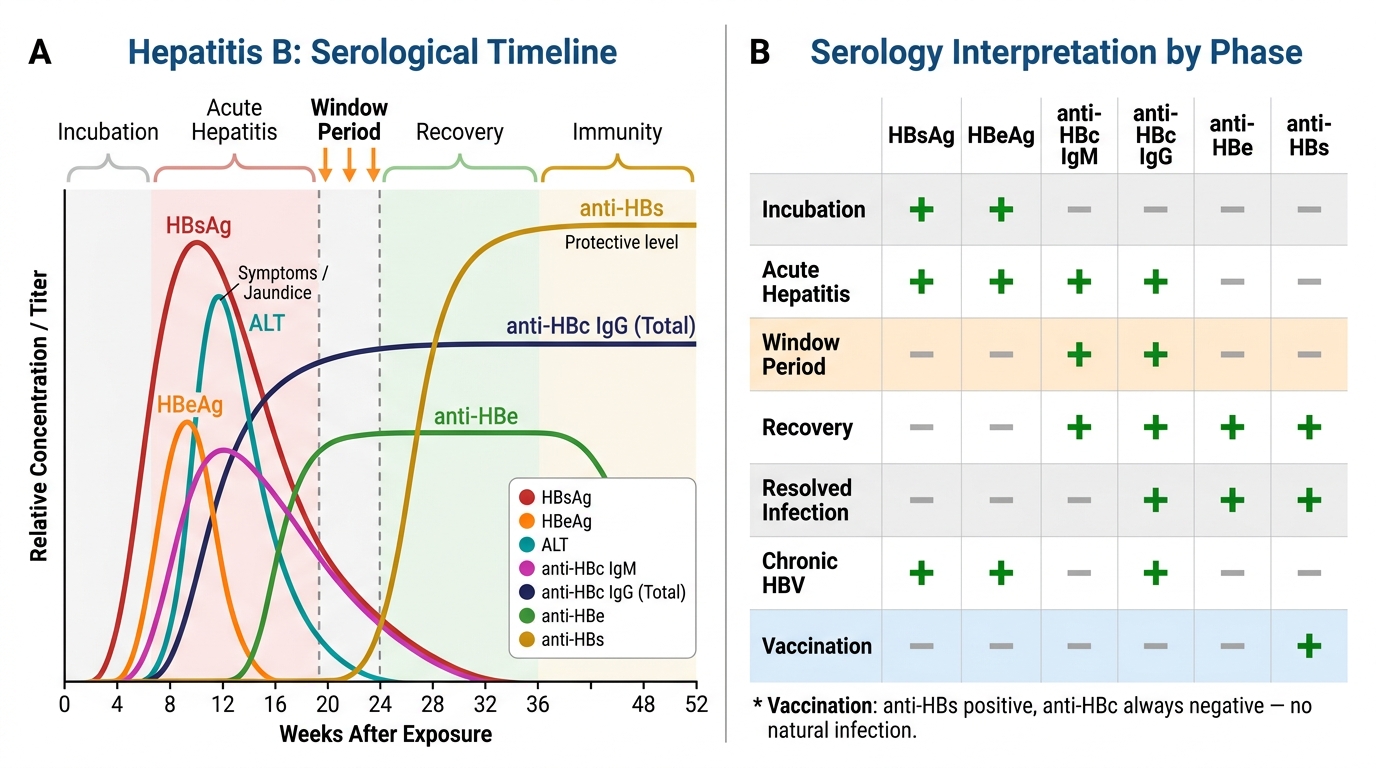
| HBsAg | Surface antigen (envelope protein) | Active infection (acute or chronic) — appears 1–10 wks after exposure, before symptoms |
| Anti-HBs (HBsAb) | Antibody to surface antigen | Recovery/immunity — appears after HBsAg clears; also positive after vaccination |
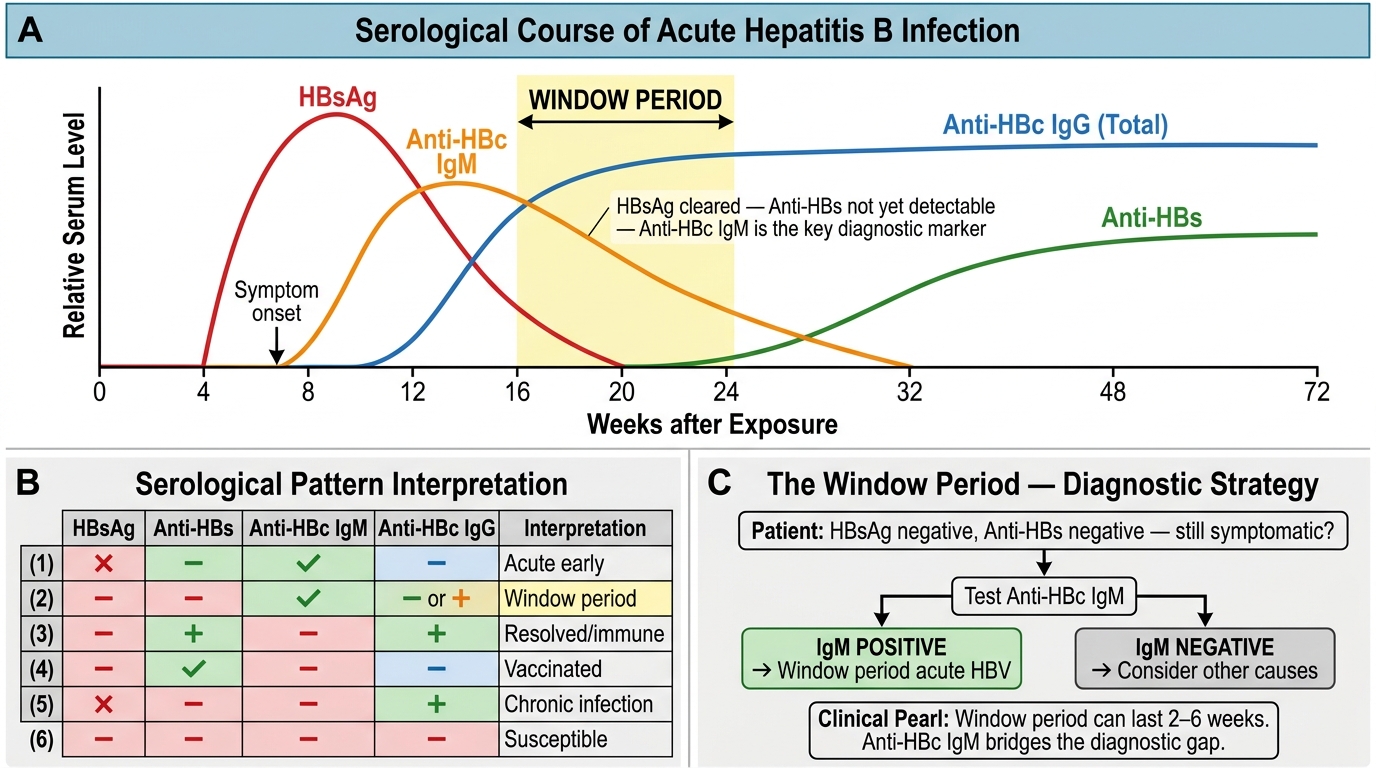
| Anti-HBc IgM | IgM antibody to core antigen | Acute infection (window period marker — positive when HBsAg has cleared but anti-HBs not yet appeared) |
| Anti-HBc IgG (total anti-HBc) | IgG antibody to core antigen | Past exposure (recovered or chronic); NOT induced by vaccine |
| HBeAg | e-antigen (secreted core protein) | High viral replication, high infectivity |
| Anti-HBe | Antibody to e-antigen | Declining replication — seroconversion is a treatment goal in HBeAg-positive chronic hepatitis B |
Interpretation patterns:
| Pattern | HBsAg | Anti-HBs | Anti-HBc IgM | Anti-HBc IgG | HBeAg | Interpretation |
|---|---|---|---|---|---|---|
| Acute hepatitis B | + | − | + | − | +/− | Active acute infection |
| Window period | − | − | + | +/− | − | HBsAg cleared, anti-HBs not yet; anti-HBc IgM is the only positive marker |
| Resolved infection | − | + | − | + | − | Recovered; immune via natural infection |
| Vaccinated | − | + | − | − | − | Immune via vaccine (no core antibody — vaccine contains only HBsAg) |
| Chronic HBV (active) | + | − | − | + | + | >6 months HBsAg positive; high replication |
| Chronic HBV (inactive) | + | − | − | + | − | Carrier state; lower replication |
Hepatitis C serology:
- Anti-HCV (ELISA): screener — positive in active and resolved infection. Cannot distinguish.
- HCV RNA (PCR): confirms active replication; positive within days of infection (before antibody). A positive anti-HCV + undetectable HCV RNA = resolved infection.
Hepatitis B Serology Timeline and Interpretation Reference
SELF-CHECK
A 28-year-old healthcare worker has a needlestick injury. Baseline serology: HBsAg negative, anti-HBs 150 mIU/mL, anti-HBc IgM negative, anti-HBc IgG negative. What is the correct interpretation?
A. Chronic hepatitis B carrier state
B. Window period of acute hepatitis B infection
C. Resolved natural hepatitis B infection
D. Protective immunity from prior vaccination
Reveal Answer
Answer: D. Protective immunity from prior vaccination
Anti-HBs positive (>10 mIU/mL is protective), HBsAg negative, and — crucially — anti-HBc IgG negative. Anti-HBc is generated only by natural infection, not by vaccination (the vaccine contains only HBsAg). Therefore a pattern of anti-HBs positive + anti-HBc negative = vaccination-induced immunity. Resolved natural infection would show anti-HBs + anti-HBc IgG both positive. Window period shows anti-HBc IgM positive. Chronic HBV shows HBsAg positive.
Clinical Integration: Putting It All Together
Three-Step LFT Framework: Clinical Integration
The three-step LFT framework in practice:
Step 1 — Dominant pattern?
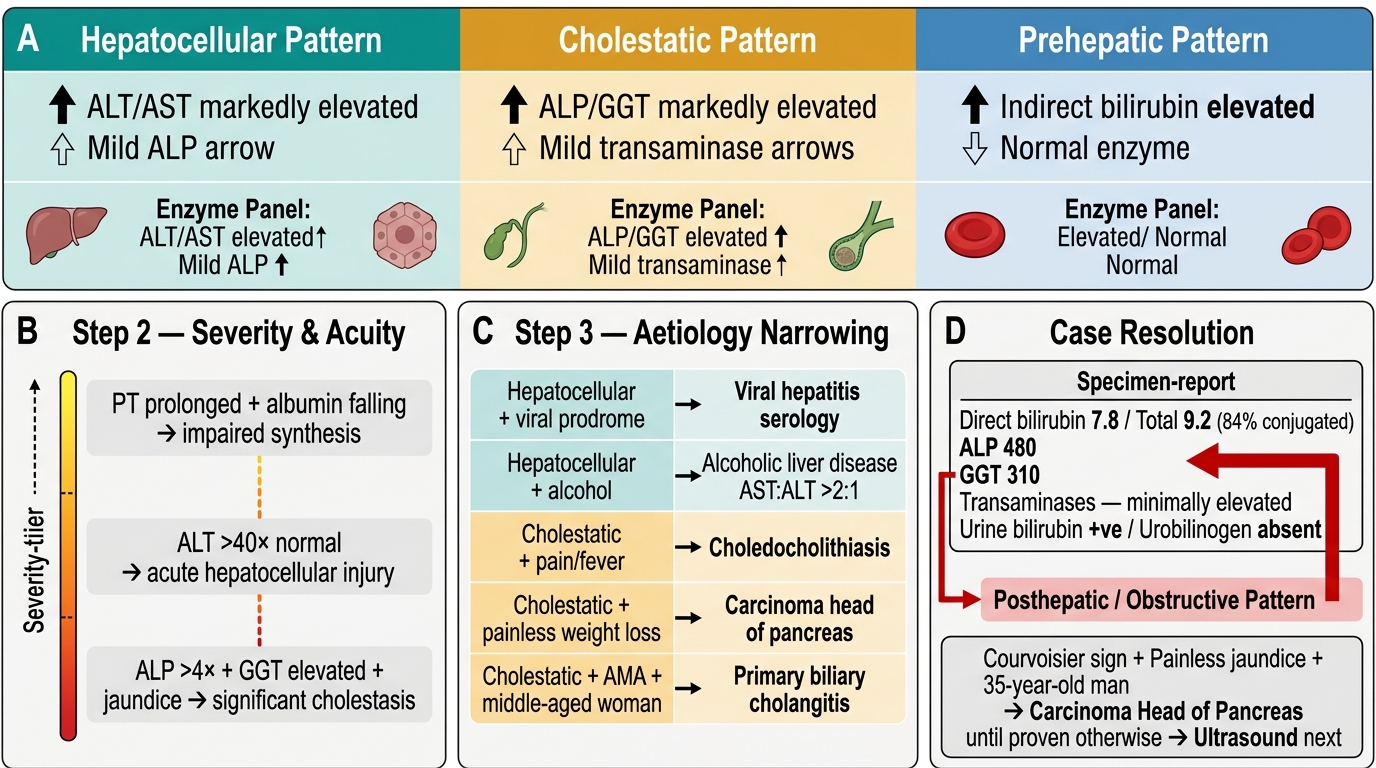
- Transaminases (ALT/AST) markedly elevated, ALP mildly elevated → Hepatocellular
- ALP/GGT markedly elevated, transaminases mildly elevated → Cholestatic
- Bilirubin predominantly indirect, transaminases/ALP normal → Prehepatic
Step 2 — Severity and acuity?
- PT prolonged + albumin falling → impaired synthesis → severity marker (indicates significant parenchymal reserve loss)
- ALT >40× normal → acute/severe hepatocellular injury (paracetamol, ischaemia, fulminant viral)
- ALP >4× + GGT elevated + jaundice → significant cholestasis
Step 3 — Aetiology narrowing:
- Hepatocellular + viral prodrome → hepatitis serology (HBsAg, anti-HBc IgM, anti-HCV)
- Hepatocellular + history of alcohol → AST:ALT >2:1, ↑GGT, ↓MCV
- Cholestatic + pain + fever → choledocholithiasis (ultrasound)
- Cholestatic + painless + weight loss → carcinoma head of pancreas (CECT)
- Cholestatic + AMA positive + middle-aged woman → Primary biliary cholangitis
Return to the opening case: Direct bilirubin 7.8/total 9.2 (84% conjugated), ALP 480, GGT 310, transaminases minimally elevated, urine bilirubin positive, urobilinogen absent → Posthepatic/obstructive pattern. Courvoisier sign in a 35-year-old man with painless progressive jaundice → carcinoma head of pancreas until proven otherwise. Ultrasound next.