Page 19 of 32
PA24.8 | Cholelithiasis & Cholecystitis — SDL Guide
Learning Objectives
- Classify gallstone types and explain the pathogenesis of cholesterol, black pigment, and brown pigment stones
- Describe the pathological sequence in acute calculous and acalculous cholecystitis
- Identify the gross and microscopic features of acute and chronic cholecystitis
- Enumerate complications of cholelithiasis and cholecystitis and explain their mechanisms
- Correlate porcelain gallbladder, gallstone ileus, and ascending cholangitis with their underlying pathology
- Recognise the risk factors for gallbladder carcinoma and its association with chronic gallbladder disease
INSTRUCTIONS
Gallstones are among the most common surgical conditions in South Asia, and gallbladder carcinoma carries one of the highest incidences in India. This module traces the pathogenesis of stone formation from bile chemistry through to the complications that make cholelithiasis a systemic disease — equipping you to reason through any patient who presents with right upper quadrant pain or obstructive jaundice.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 16 (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 20 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 42-year-old woman — overweight, has had two pregnancies, and is a non-vegetarian — presents with colicky right upper quadrant pain radiating to the right shoulder after a fatty meal. Ultrasound shows echogenic foci with posterior acoustic shadowing in the gallbladder. She asks: "Doctor, how did these stones form?" By the end of this module, you will not only answer that question but also predict every complication she risks if they are left untreated.
WHY THIS MATTERS
Cholelithiasis affects approximately 10–15% of adults worldwide, with India recording some of the highest gallbladder carcinoma rates globally — particularly in the Gangetic belt. For a Year-2 student, understanding stone pathogenesis and the cholecystitis cascade is essential because:
- It integrates bile biochemistry (PY), hepatic anatomy (AN), and clinical medicine
- Complications — empyema, perforation, ascending cholangitis, pancreatitis — span multiple organ systems
- Chronic cholecystitis → porcelain gallbladder → carcinoma is a testable, high-yield progression
- Cross-reference SDL 1 (obstructive jaundice) applies whenever choledocholithiasis is discussed
RECALL
Before proceeding, refresh the following from Year 1:
- Bile composition: bile salts, lecithin (phospholipid), cholesterol, bilirubin, water — the balance between these determines lithogenicity
- Enterohepatic circulation: bile salt recycling via ileal reabsorption; disruption by ileal disease (e.g., Crohn's) increases cholesterol stone risk
- Haemolysis and bilirubin metabolism: unconjugated → conjugated bilirubin in hepatocytes; excess unconjugated load leads to pigment stone formation
- Murphy's sign: arrest of inspiration on deep palpation in the right hypochondrium — indicates acute cholecystitis
Classification of Gallstones
Classification of Gallstones
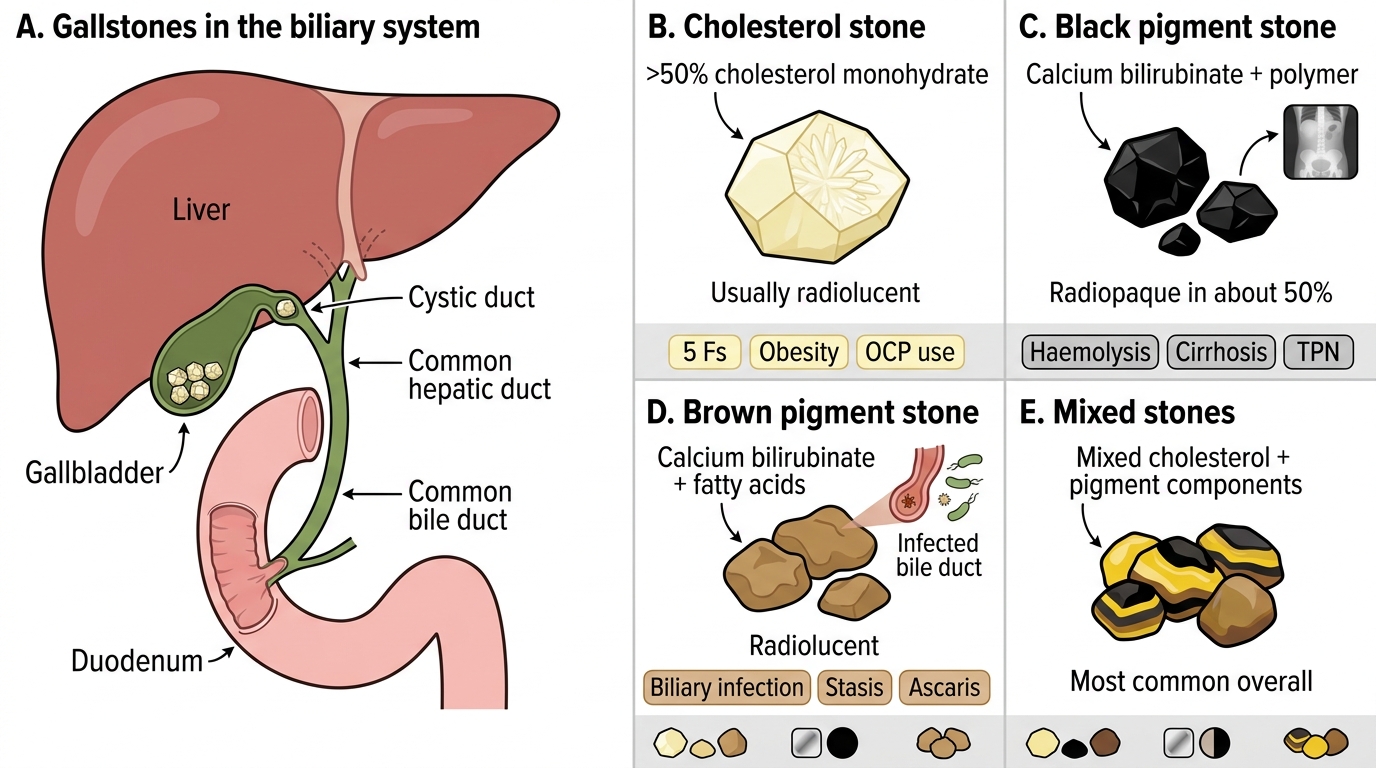
Gallstones (cholelithiasis) are crystalline concretions that form within the biliary system. Three major types are recognised:
| Type | Composition | Colour | Radiopaque? | Key associations |
|---|---|---|---|---|
| Cholesterol stones | >50% cholesterol monohydrate | Pale yellow–white | No (10%) | 5 Fs, obesity, OCP |
| Black pigment stones | Calcium bilirubinate + polymer | Jet black | Yes (50%) | Haemolysis, cirrhosis, TPN |
| Brown pigment stones | Calcium bilirubinate + fatty acids | Brown–tan | No | Biliary infection, stasis, Ascaris |
Mixed stones (most common overall) are cholesterol-predominant with pigment layers, often multiple and faceted from mutual compression.
IMPORTANT NOTE: Cholesterol stones account for ~80% of gallstones in Western populations; pigment stones predominate in haemolytic disorders and in parts of Asia with high biliary infection burden.
Pathogenesis of Cholesterol Stones — The Three Pillars
Pathogenesis of Cholesterol Gallstones: The Three Pillars
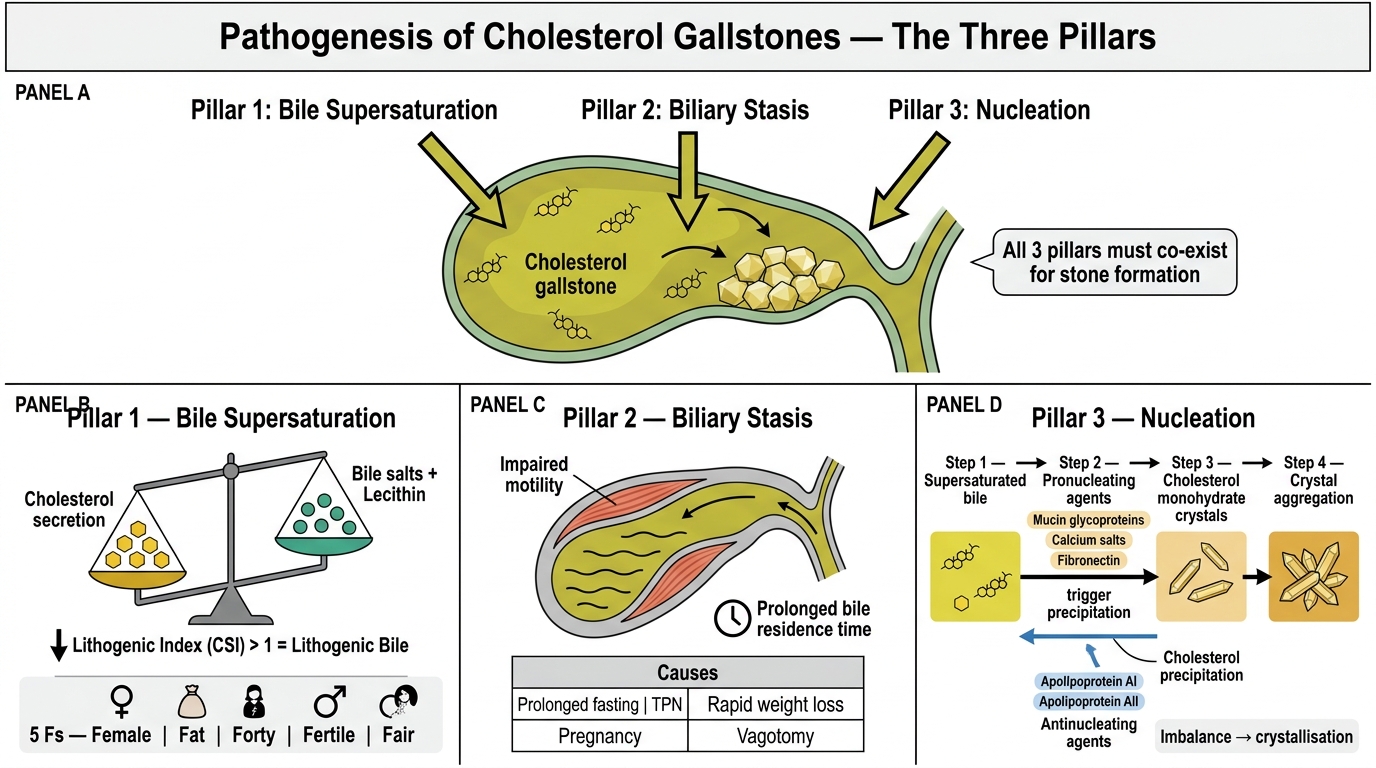
Cholesterol is insoluble in water and is held in aqueous bile as mixed micelles (with bile salts) and vesicles (with lecithin). Three conditions must co-exist for cholesterol stone formation:
1. Bile supersaturation with cholesterol
Occurs when cholesterol secretion exceeds the solubilising capacity of bile salts and lecithin. The lithogenic index (or cholesterol saturation index) >1 indicates supersaturated bile. Risk factors follow the mnemonic 5 Fs:
• Female (oestrogen ↑ cholesterol secretion, ↓ bile salt pool)
• Fat (obesity → ↑ hepatic cholesterol synthesis)
• Forty (prevalence rises steeply after age 40)
• Fertile (multiparity; pregnancy hormones → biliary stasis)
• Fair (Northern European and Native American genetic predisposition — ABCG5/ABCG8 polymorphisms)
Oral contraceptive pills and fibrate drugs also raise lithogenicity.
2. Biliary stasis
Impaired gallbladder motility allows prolonged bile residence, promoting crystal growth. Causes: prolonged fasting, TPN, pregnancy, rapid weight loss, vagotomy.
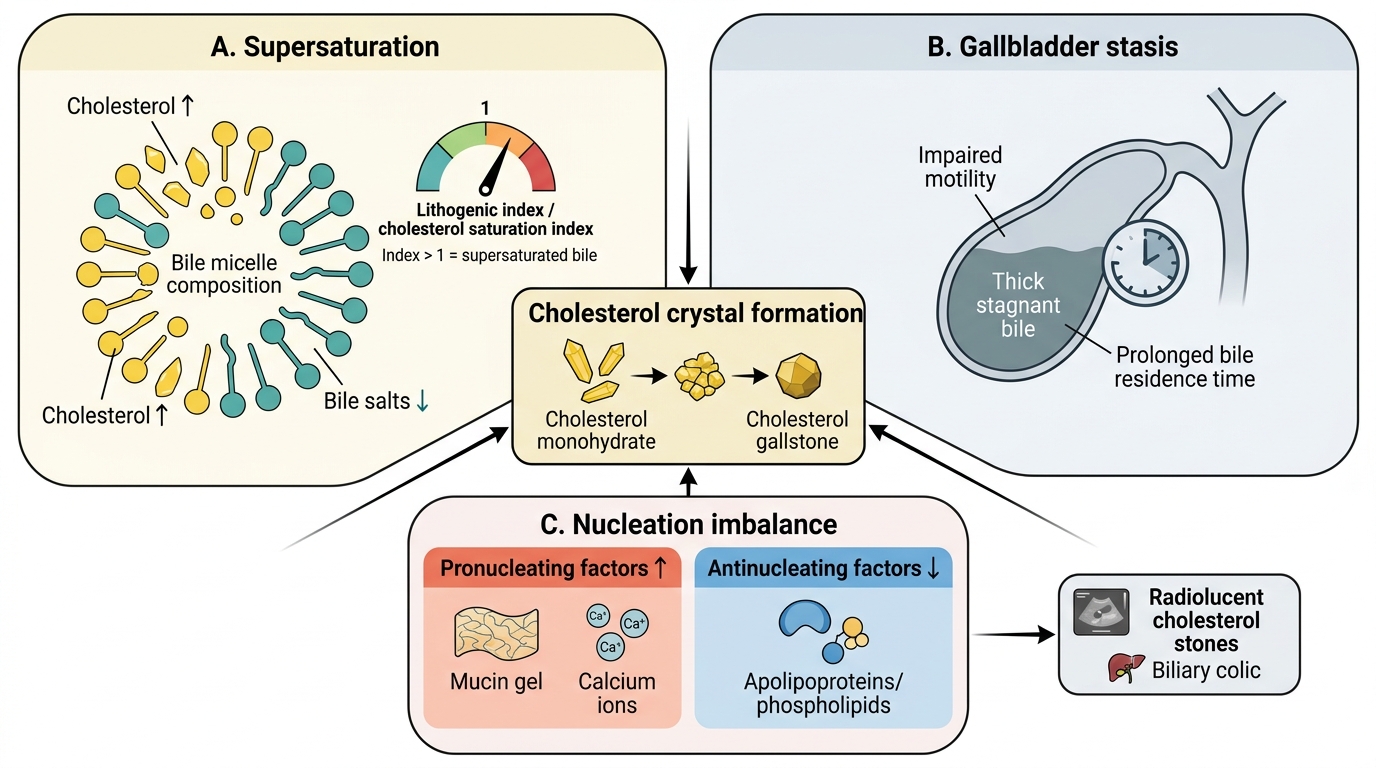
3. Nucleation
Precipitation of cholesterol monohydrate crystals from supersaturated bile. Pronucleating agents (mucin glycoproteins, calcium salts, fibronectin) accelerate this; antinucleating agents (apolipoproteins AI/AII) oppose it. An imbalance tips the equilibrium toward crystallisation.
Once crystals nucleate, they aggregate and are trapped by mucin gel secreted by the gallbladder epithelium — forming the nidus of the macroscopic stone.
Three-Pillar Pathogenesis of Cholesterol Gallstones
SELF-CHECK
A 48-year-old woman on long-term fibrate therapy for hypertriglyceridaemia develops biliary colic. Ultrasound confirms radiolucent gallstones. Which mechanism best explains her stone formation?
A. Fibrate-induced increase in biliary cholesterol secretion causing supersaturation
B. Increased unconjugated bilirubin load precipitating calcium bilirubinate
C. Biliary infection by Escherichia coli hydrolysing conjugated bilirubin
D. Haemolysis reducing the bile salt pool
Reveal Answer
Answer: A. Fibrate-induced increase in biliary cholesterol secretion causing supersaturation
Fibrates increase biliary cholesterol secretion (via ABCG5/ABCG8 upregulation), raising the cholesterol saturation index above 1 — the primary driver of cholesterol stone formation. Radiolucent (non-opaque) stones are characteristic of cholesterol stones. Options B and C describe pigment stone pathogenesis; option D is incorrect (haemolysis does not reduce the bile salt pool).
Pathogenesis of Pigment Stones
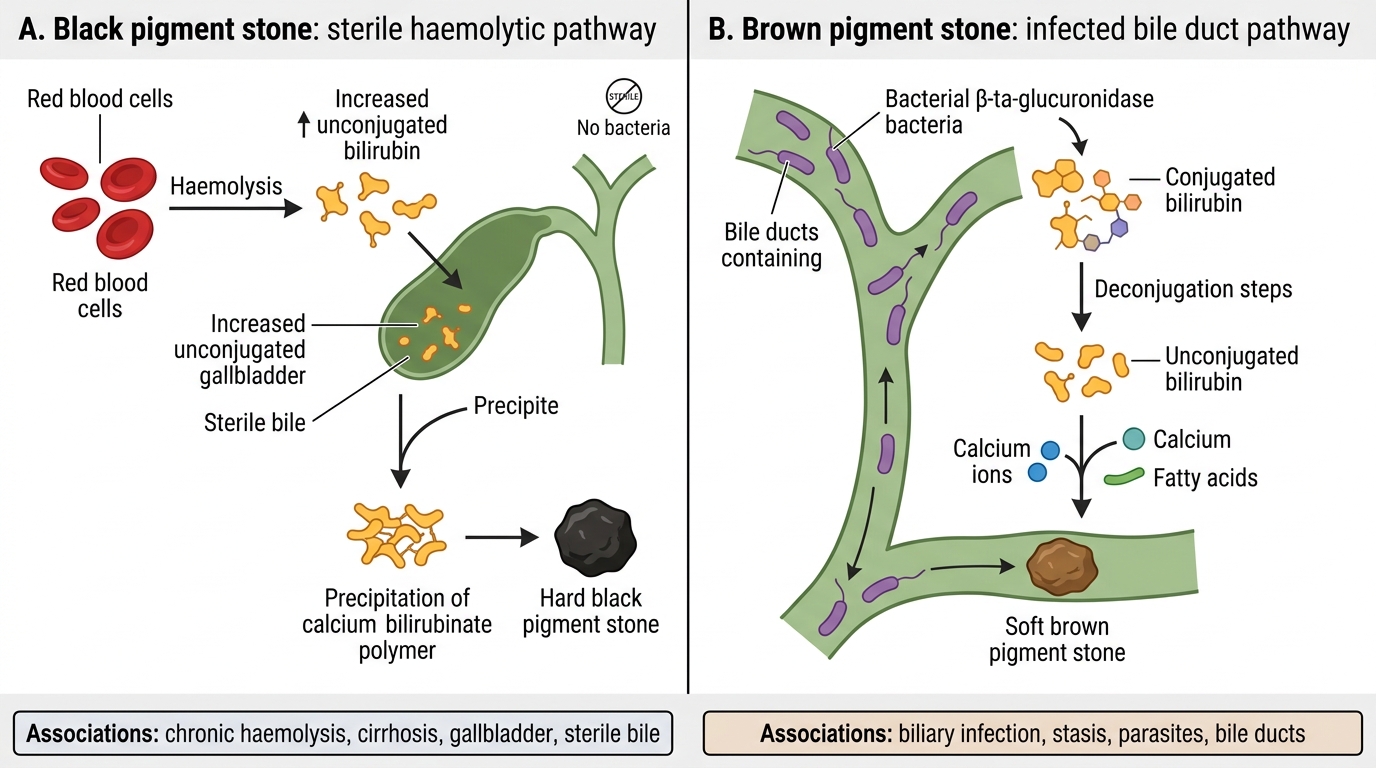
Pathogenesis of Pigment Stones: Black vs Brown
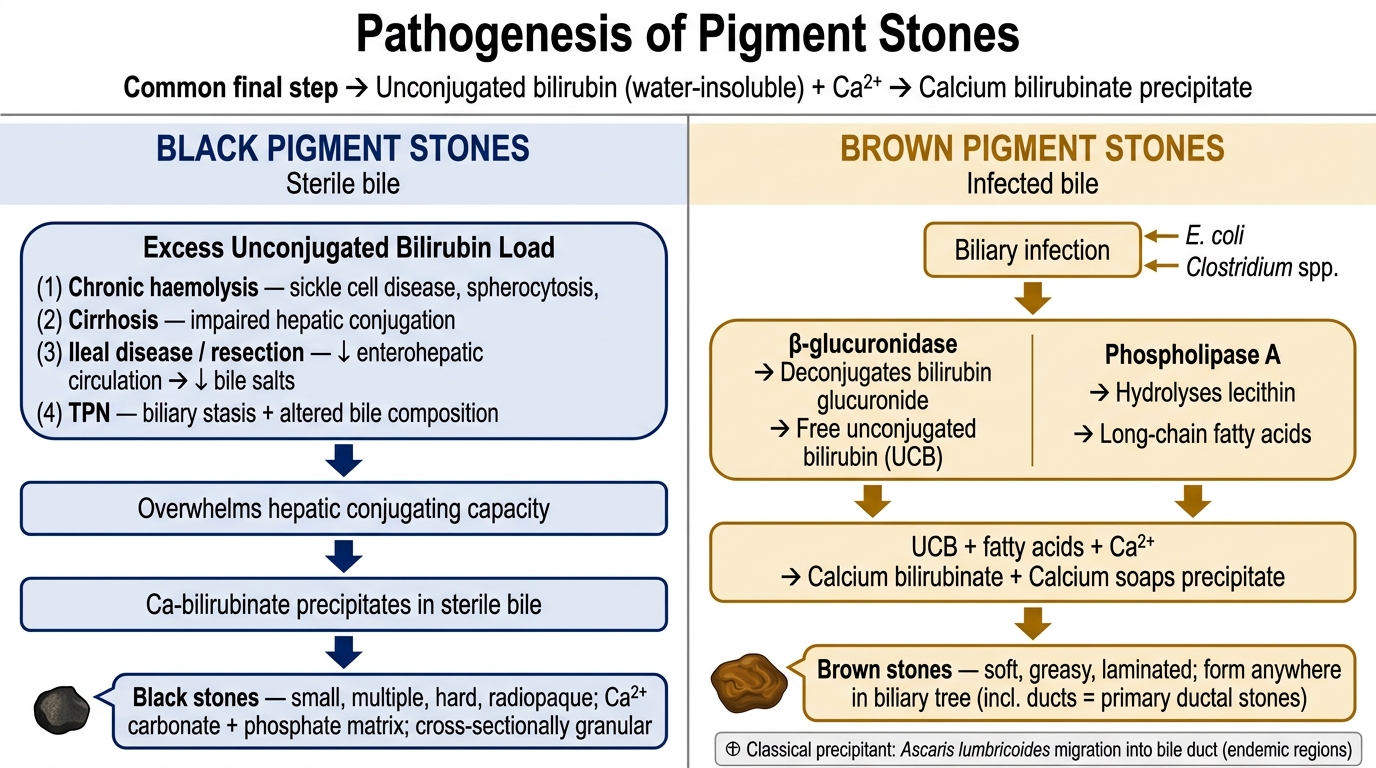
Pigment stones form when unconjugated bilirubin (which is water-insoluble) precipitates in bile as calcium bilirubinate.
Black pigment stones
Form in sterile bile. Excess unconjugated bilirubin load overwhelms hepatic conjugating capacity:
• Chronic haemolysis: sickle cell disease, hereditary spherocytosis, thalassaemia
• Cirrhosis: impaired hepatic conjugation
• Ileal disease/resection: interrupts enterohepatic circulation → bile salt deficiency → relative bilirubin excess
• Total parenteral nutrition: biliary stasis + altered bile composition
Black stones are small, multiple, hard, and cross-sectionally granular. They are radiopaque due to calcium carbonate and phosphate incorporated in the polymer matrix.
Brown pigment stones
Form in infected bile. Bacteria (notably E. coli, Clostridium) produce β-glucuronidase, which deconjugates bilirubin glucuronide → free unconjugated bilirubin → precipitates with calcium. The fatty acid component comes from bacterial phospholipase A hydrolysing lecithin.
Brown stones are soft, greasy, laminated, and may form anywhere in the biliary tree (including bile ducts — primary ductal stones). Ascaris lumbricoides migration into the bile duct is a classical precipitating factor in endemic regions.
Pathogenesis of Black vs Brown Pigment Gallstones