Page 20 of 32
PA24.8 | Cholelithiasis & Cholecystitis — SDL Guide (Part 2)
Morphology of Gallstones and Clinical Presentation
Gallstones: Morphology and Clinical Presentation
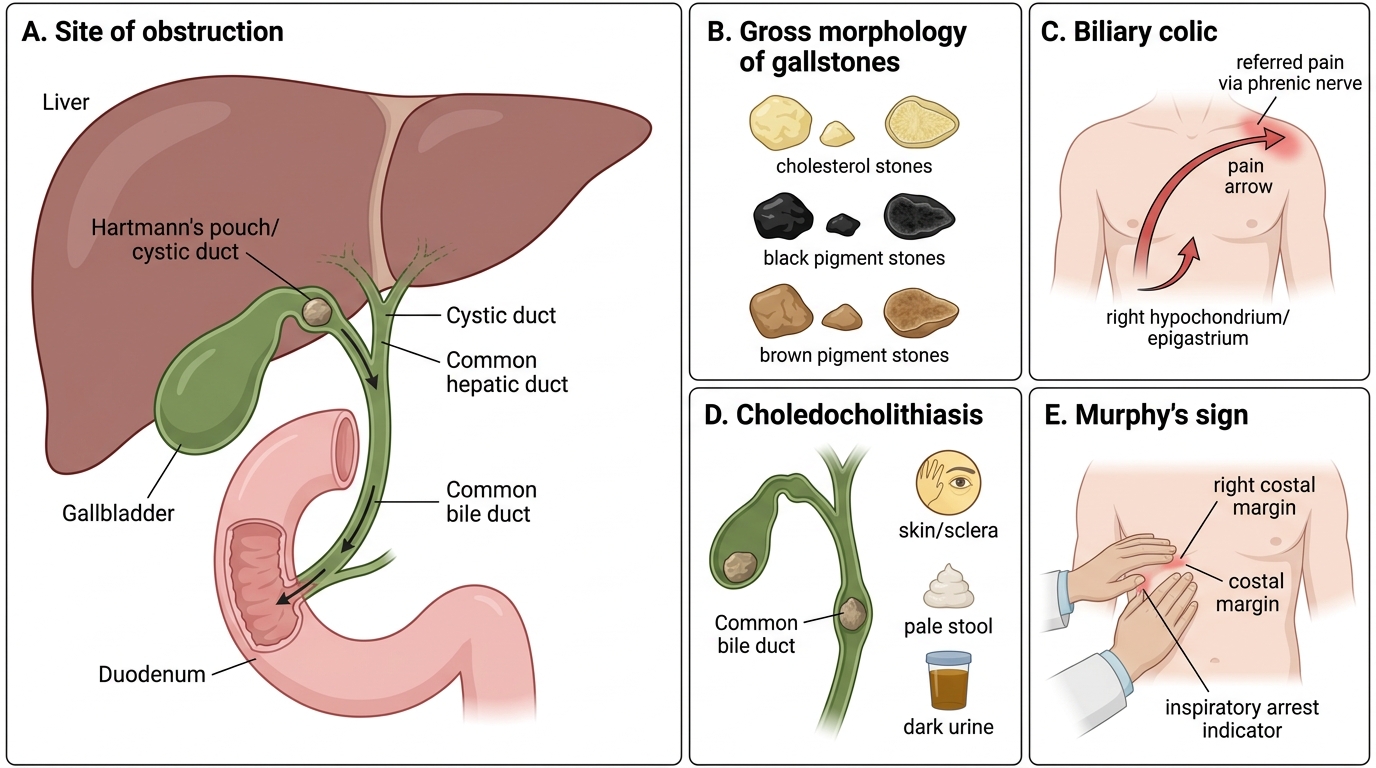
Gross morphology
• Cholesterol stones: pale yellow, round/oval, solitary or multiple, faceted when multiple; cut surface shows radiating crystalline pattern
• Black pigment stones: small, jet-black, multiple, irregular, crumble easily
• Brown pigment stones: soft, tan-brown, laminated, variable size
Clinicopathological correlations
• Asymptomatic: ~80% of gallstone carriers remain asymptomatic for years ('silent gallstones'); annual risk of symptoms is ~1–2%
• Biliary colic: stone transiently obstructs the cystic duct or Hartmann's pouch → right hypochondriac/epigastric pain, colicky, radiates to right shoulder (referred via phrenic nerve), lasts 30 min to several hours, triggered by fatty meals
• Choledocholithiasis: stone passes into the common bile duct → obstructive jaundice, pale stools, dark urine (cross-reference SDL 1: obstructive jaundice pathway)
• Murphy's sign: inspiratory arrest on deep palpation at the right costal margin (gallbladder fundus) — positive in acute cholecystitis
Acute Cholecystitis — Pathogenesis
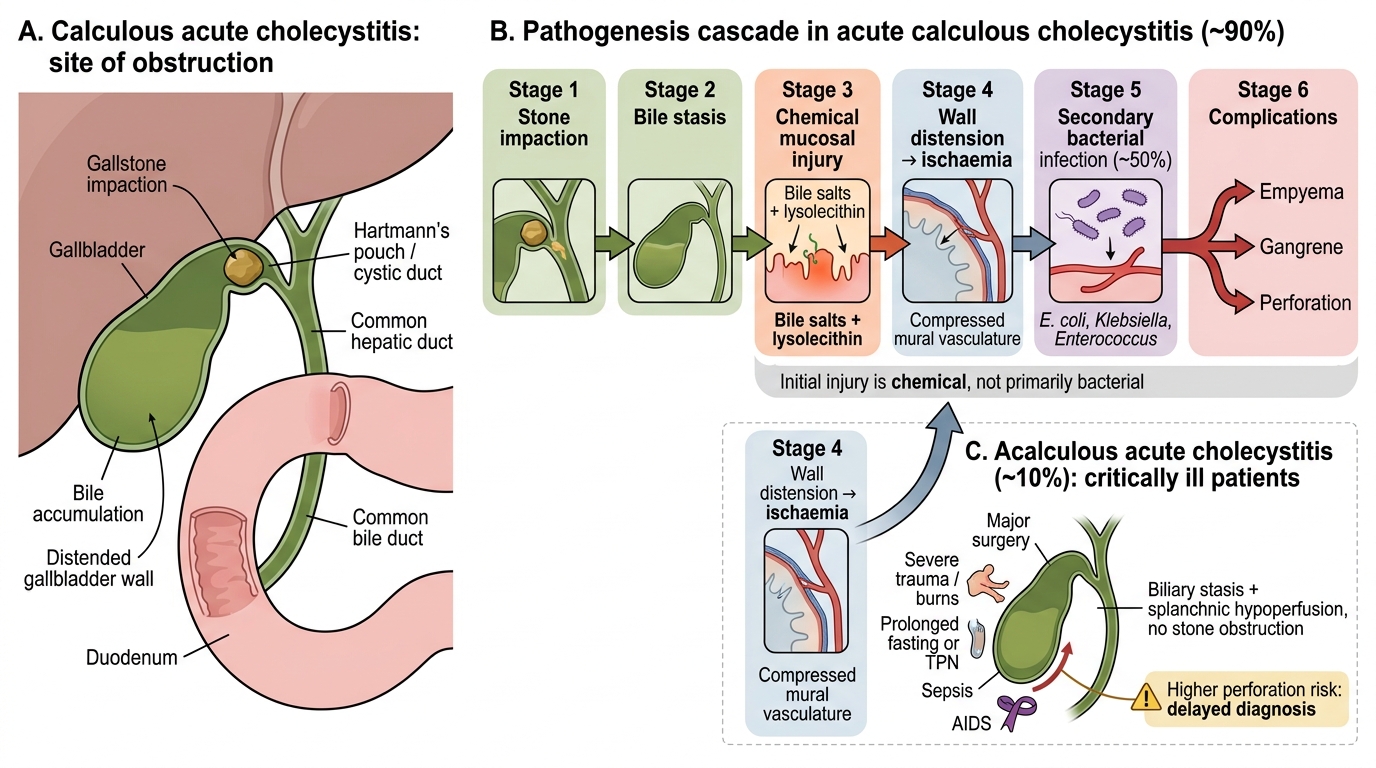
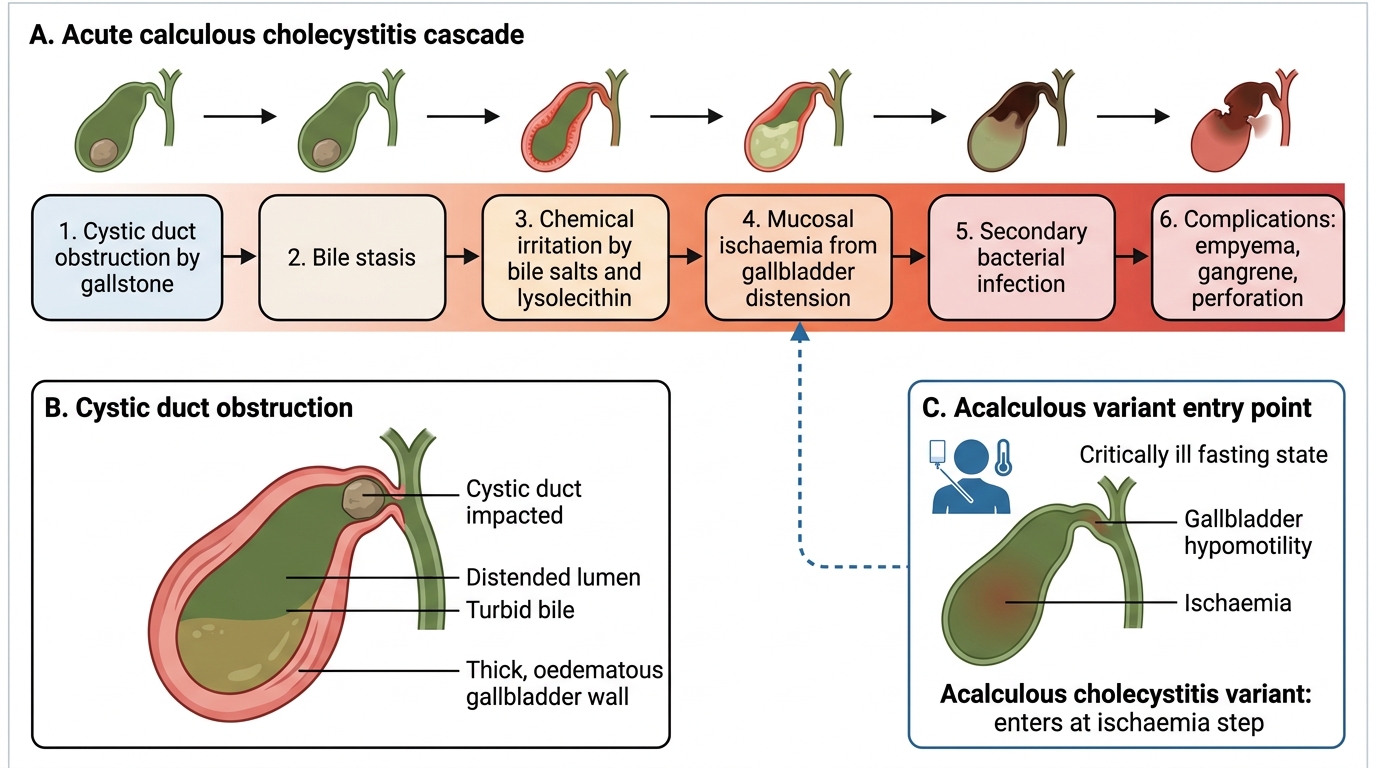
Pathogenesis of Acute Cholecystitis
Acute calculous cholecystitis (~90% of cases) follows obstruction of the cystic duct or Hartmann's pouch by a gallstone. The sequence:
- Stone impaction → bile accumulation behind the obstruction
- Chemical irritation: concentrated bile salts and lysolecithin (from lecithin hydrolysis by phospholipase) damage the mucosa
- Ischaemia: distension of the gallbladder wall compresses mural vasculature → mucosal ischaemia
- Secondary bacterial infection: E. coli, Klebsiella, Enterococcus — superimposed in ~50% of cases via portal bacteraemia or ascending route
Note: The initial injury is chemical, not primarily bacterial; hence even culture-negative acute cholecystitis follows this identical morphological sequence.
Acute acalculous cholecystitis (~10%) occurs in critically ill patients — major surgery, severe trauma, burns, prolonged fasting/TPN, sepsis, AIDS. Pathogenesis: biliary stasis + ischaemia (hypoperfusion of splanchnic bed) without stone obstruction. Carries higher perforation risk because diagnosis is delayed.
Pathogenesis of Acute Cholecystitis
Morphology of Acute and Chronic Cholecystitis
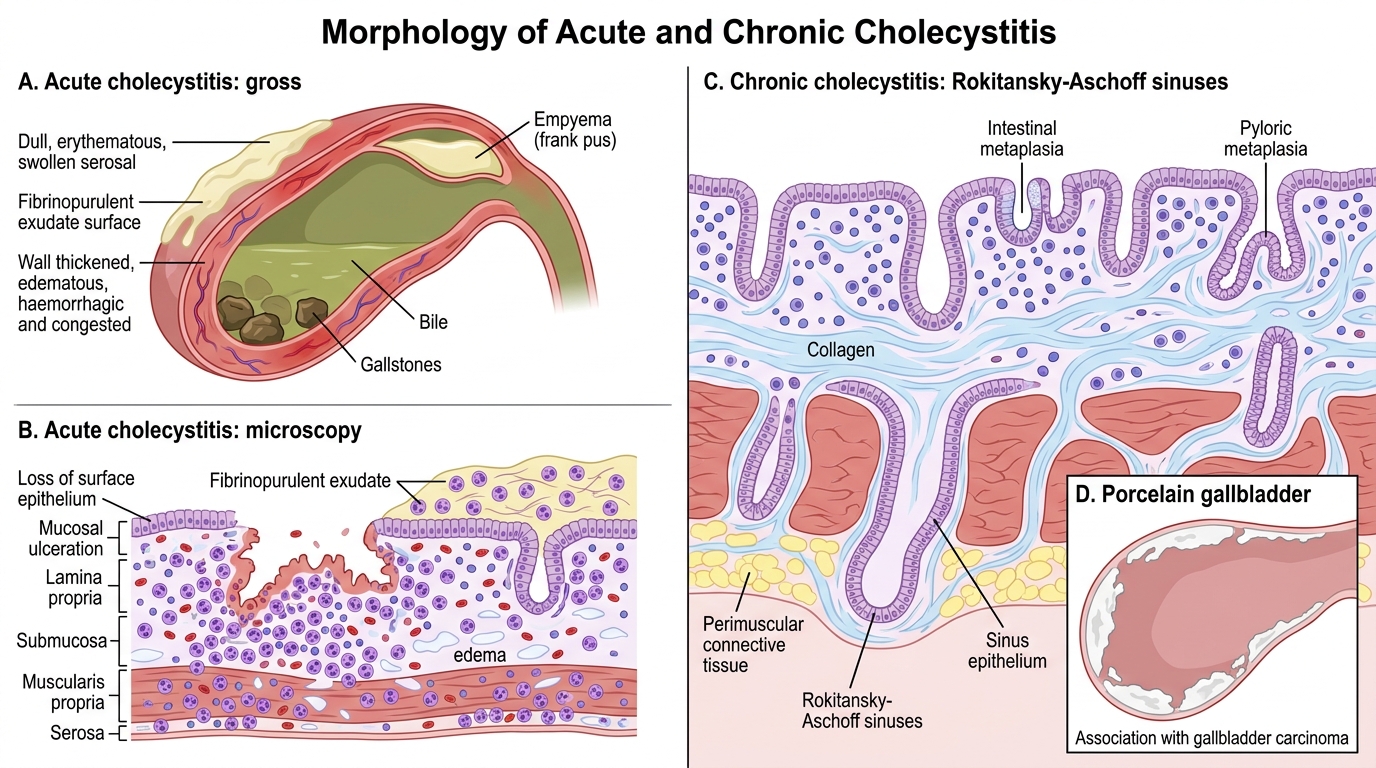
Morphology of Acute and Chronic Cholecystitis
Acute cholecystitis — gross
• Gallbladder enlarged, tense, dull serosa with fibrinopurulent exudate
• Wall oedematous, haemorrhagic, congested
• Lumen contains turbid bile, pus, or stones
• Empyema: lumen distended with frank pus
• Gangrenous cholecystitis: transmural necrosis → green-black discolouration → perforation risk
Acute cholecystitis — microscopy
• Mucosal ulceration with neutrophilic infiltration
• Oedema and congestion of all layers
• Fibrinopurulent exudate on serosa
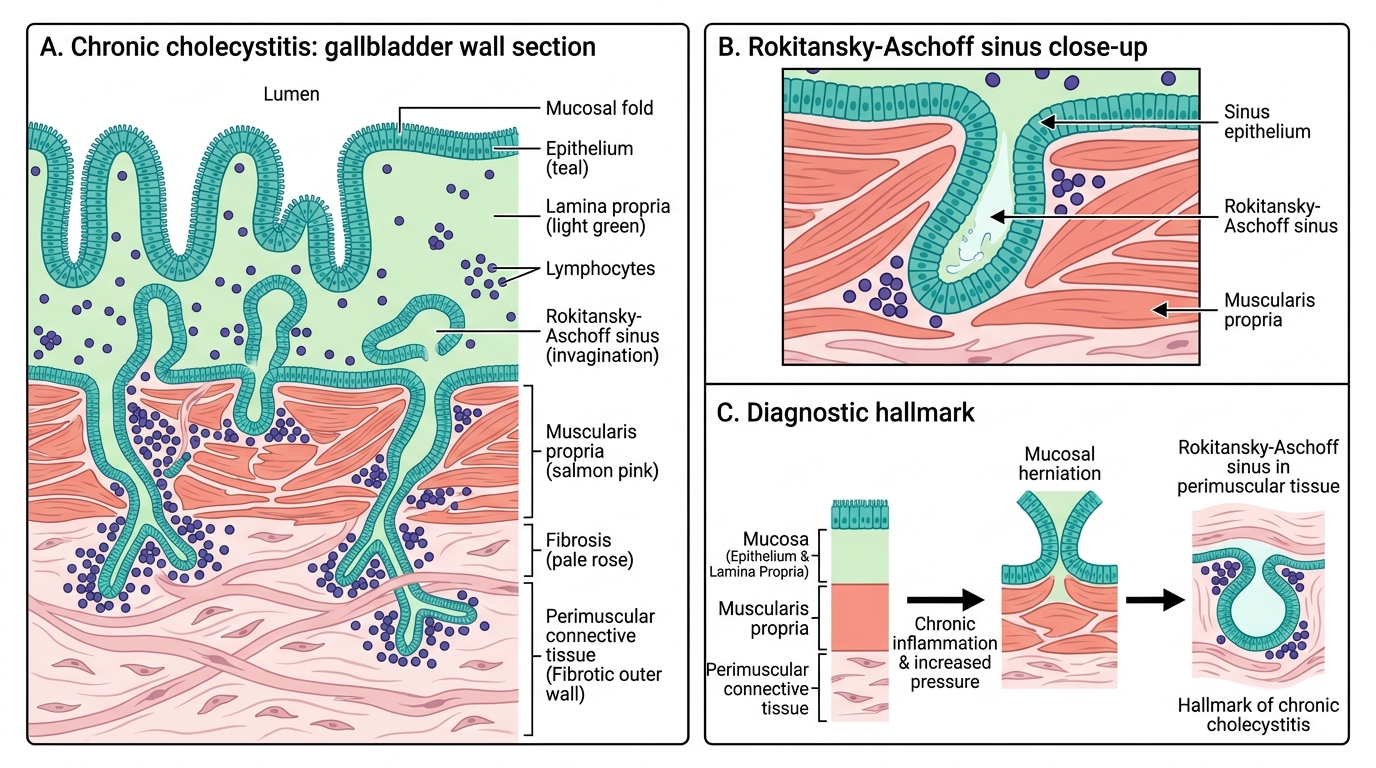
Chronic cholecystitis
Results from repeated bouts of acute inflammation or low-grade stone irritation. Key features:
- Rokitansky-Aschoff sinuses: invaginations of the gallbladder epithelium through the muscularis propria into the perimuscular tissues — result of increased intraluminal pressure over time; characteristic on histology
- Fibrosis and thickening of the wall
- Mononuclear (lymphocytic) infiltrate
- Metaplastic changes: intestinal or pyloric metaplasia
- Porcelain gallbladder: dystrophic calcification of the gallbladder wall on a background of chronic cholecystitis — radiologically detectable; carries association with gallbladder carcinoma (though recent data suggest risk is lower than historically quoted)
Rokitansky-Aschoff Sinuses in Chronic Cholecystitis
SELF-CHECK
On histology, invaginations of the gallbladder epithelium penetrating through the muscularis into the perimuscular connective tissue are termed:
A. Brunn's nests
B. Psammoma bodies
C. Rokitansky-Aschoff sinuses
D. Creola bodies
Reveal Answer
Answer: C. Rokitansky-Aschoff sinuses
Rokitansky-Aschoff sinuses are the hallmark histological feature of chronic cholecystitis. They form due to repeated elevation of intraluminal pressure (from stones, obstruction, or repeated bouts of acute inflammation), causing the mucosa to herniate through the muscularis propria. Brunn's nests are found in the urinary bladder; psammoma bodies are calcifications seen in papillary thyroid carcinoma, meningioma, and serous ovarian tumours.