Page 21 of 32
PA24.8 | Cholelithiasis & Cholecystitis — SDL Guide (Part 3)
Complications of Cholelithiasis and Cholecystitis
Complications of Cholelithiasis and Cholecystitis
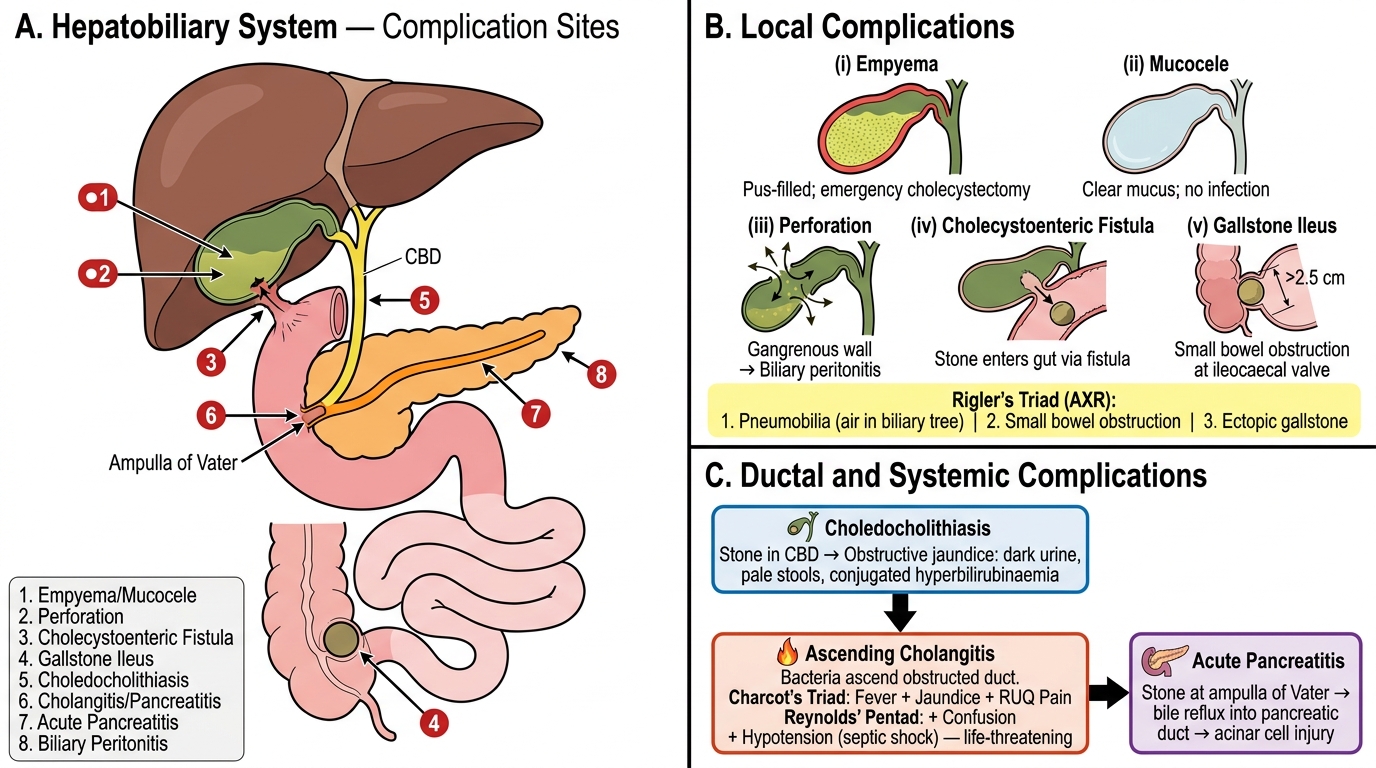
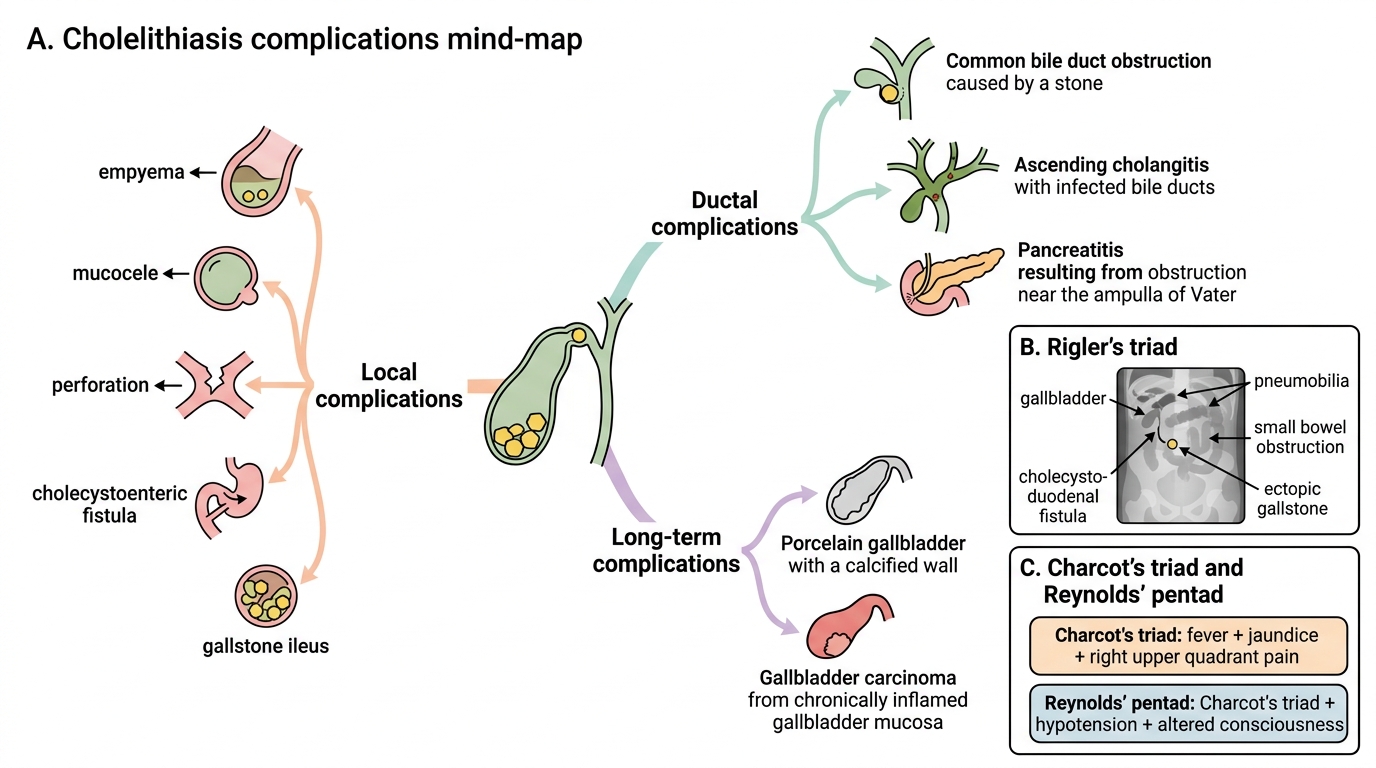
Complications span the local gallbladder to remote systemic effects:
Local complications
• Empyema of the gallbladder: pus-filled, distended gallbladder — requires emergency cholecystectomy; risk of rupture
• Perforation and biliary peritonitis: gangrenous wall ruptures → bile/pus into peritoneum; localised (pericholecystic abscess) or diffuse peritonitis
• Mucocele: chronic cystic duct obstruction without infection → gallbladder distended with clear mucus secretion; wall thin and translucent
• Cholecystoenteric fistula: gallbladder adheres and erodes into adjacent bowel (usually duodenum); allows large stone to enter gut lumen
• Gallstone ileus: large stone (>2.5 cm) enters small bowel via fistula → obstructs at the narrow ileocaecal junction → small bowel obstruction; Rigler's triad on X-ray: air in biliary tree (pneumobilia), small bowel obstruction, ectopic gallstone
Ductal and systemic complications
• Choledocholithiasis: stone in common bile duct → obstructive jaundice (dark urine, pale stools, conjugated hyperbilirubinaemia)
• Ascending cholangitis: bacteria ascend the obstructed duct → high fever, rigors, jaundice (Charcot's triad); Reynolds' pentad adds confusion + hypotension (septic shock); life-threatening
• Acute pancreatitis: stone impacting at the ampulla of Vater → reflux of bile into pancreatic duct → acinar cell injury
Long-term sequelae
• Porcelain gallbladder: calcified, brittle wall → association with gallbladder carcinoma
• Gallbladder carcinoma (see next block)
Complications of Cholelithiasis
CLINICAL PEARL
Charcot's Triad vs Reynolds' Pentad
Charcot's triad (fever + jaundice + right upper quadrant pain) diagnoses ascending cholangitis. Reynolds' pentad adds altered consciousness and hypotension — signalling septic shock from biliary source. This escalation from cholangitis to Reynolds' pentad represents a surgical emergency requiring urgent biliary decompression.
Gallstone ileus teaching point: The X-ray triad (pneumobilia + small bowel obstruction + ectopic stone) occurs because the stone erodes through the gallbladder wall into the duodenum (cholecystoduodenal fistula), allowing gas to enter the biliary tree. Ask for this in any elderly patient with small bowel obstruction and no prior surgery.
SELF-CHECK
A 65-year-old woman presents with small bowel obstruction. Plain abdominal X-ray shows air in the biliary tree and an ectopic calcific opacity in the right iliac fossa. What is the most likely underlying sequence of events?
A. Acute pancreatitis leading to peripancreatic gas tracking into the biliary tree
B. Ascending cholangitis with gas-forming organisms in the bile duct
C. Post-ERCP pneumobilia with concurrent adhesion-related obstruction
D. Cholecystoduodenal fistula allowing a large gallstone to enter the gut and impact at the ileocaecal junction
Reveal Answer
Answer: D. Cholecystoduodenal fistula allowing a large gallstone to enter the gut and impact at the ileocaecal junction
This is the classic presentation of gallstone ileus. Chronic cholecystitis causes adhesion between the gallbladder and duodenum; a large stone erodes through, creating a cholecystoduodenal fistula. Gas enters the biliary tree (pneumobilia), and the stone — too large for the small bowel lumen — impacts at the narrowest point, the ileocaecal junction. Rigler's triad (pneumobilia + SBO + ectopic stone) is the diagnostic radiological pattern.
Gallbladder Carcinoma
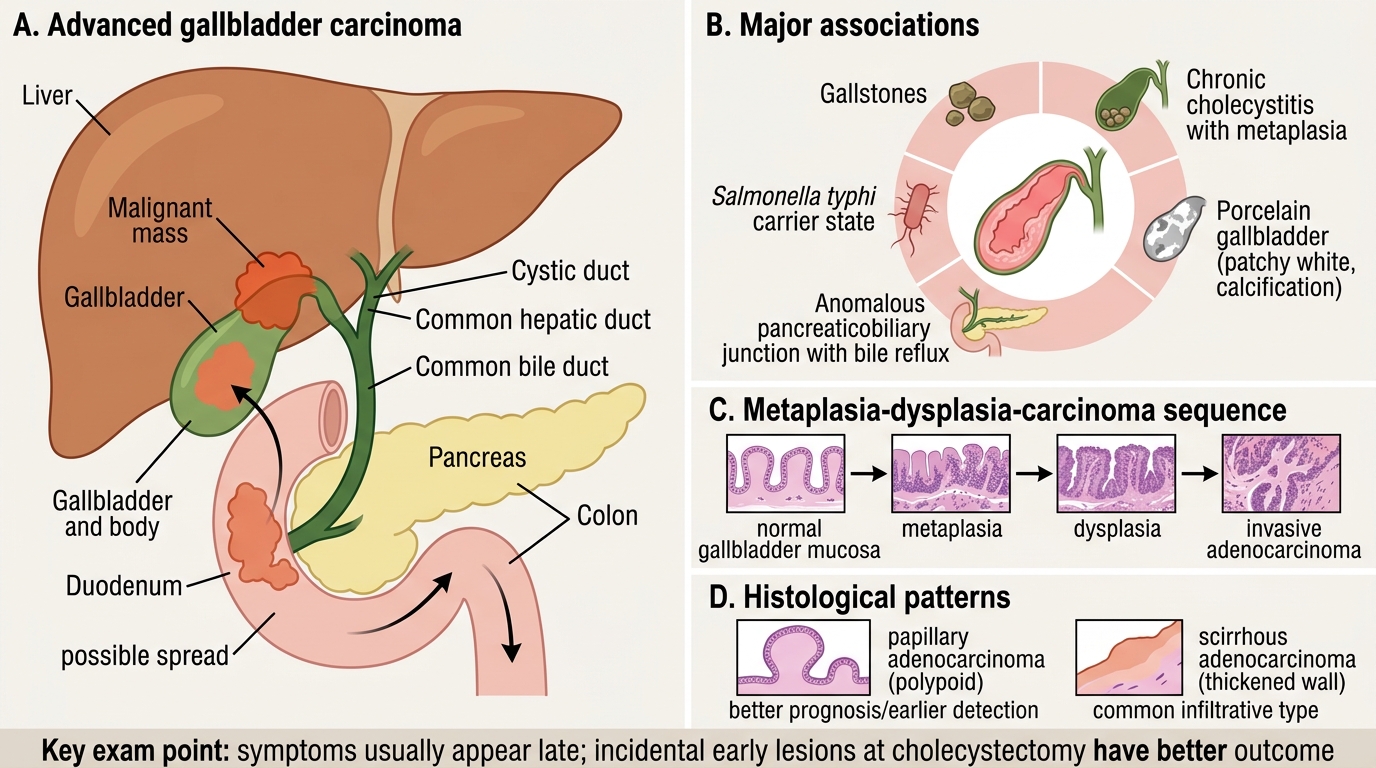
Gallbladder Carcinoma: Associations, Pathology, and Spread
Gallbladder carcinoma is the most common biliary tract malignancy. India has among the highest incidence rates globally, particularly in Uttar Pradesh, Bihar, and West Bengal.
Associations
• Gallstones present in ~70–90% of cases — chronic mucosal irritation, carcinogen concentration, and metaplasia–dysplasia–carcinoma sequence
• Chronic cholecystitis and the associated metaplastic changes (intestinal, pyloric metaplasia)
• Porcelain gallbladder — historically quoted as high risk; contemporary series suggest selective (patchy) calcification carries higher risk than complete calcification
• Anomalous pancreaticobiliary junction (bile reflux into gallbladder)
• Salmonella typhi chronic carrier state (carriage in gallbladder epithelium)
Pathology
• Histological type: adenocarcinoma (~90%) — papillary (better prognosis) or scirrhous (common, infiltrative)
• Papillary carcinoma may be polypoid and detected early
• Most present at advanced stage — direct invasion of liver, duodenum, colon
Prognosis: poor — 5-year survival <5% for most patients; early fundal lesions found incidentally at cholecystectomy have better outcomes.
Key exam point: gallbladder carcinoma is virtually always symptomatic late (right upper quadrant pain, weight loss, obstructive jaundice from common bile duct involvement) — early detection is rare outside incidental cholecystectomy findings.
SELF-CHECK
Which of the following correctly describes the association between porcelain gallbladder and carcinoma risk?
A. Porcelain gallbladder always indicates high carcinoma risk regardless of calcification pattern
B. Patchy (selective) mural calcification carries higher carcinoma risk than complete calcification
C. Porcelain gallbladder is a premalignant lesion with >50% malignant transformation
D. Carcinoma risk is greatest when porcelain gallbladder develops in the absence of prior gallstones
Reveal Answer
Answer: B. Patchy (selective) mural calcification carries higher carcinoma risk than complete calcification
Contemporary evidence has revised the historical overestimate of carcinoma risk in porcelain gallbladder. Complete (diffuse) calcification carries lower risk; selective (patchy) intramural calcification is more strongly associated with underlying carcinoma. The overall malignant transformation rate is much lower than the historically quoted figures (~7% rather than ~22%). Prophylactic cholecystectomy is generally recommended for patchy calcification.
Choledocholithiasis and Obstructive Jaundice
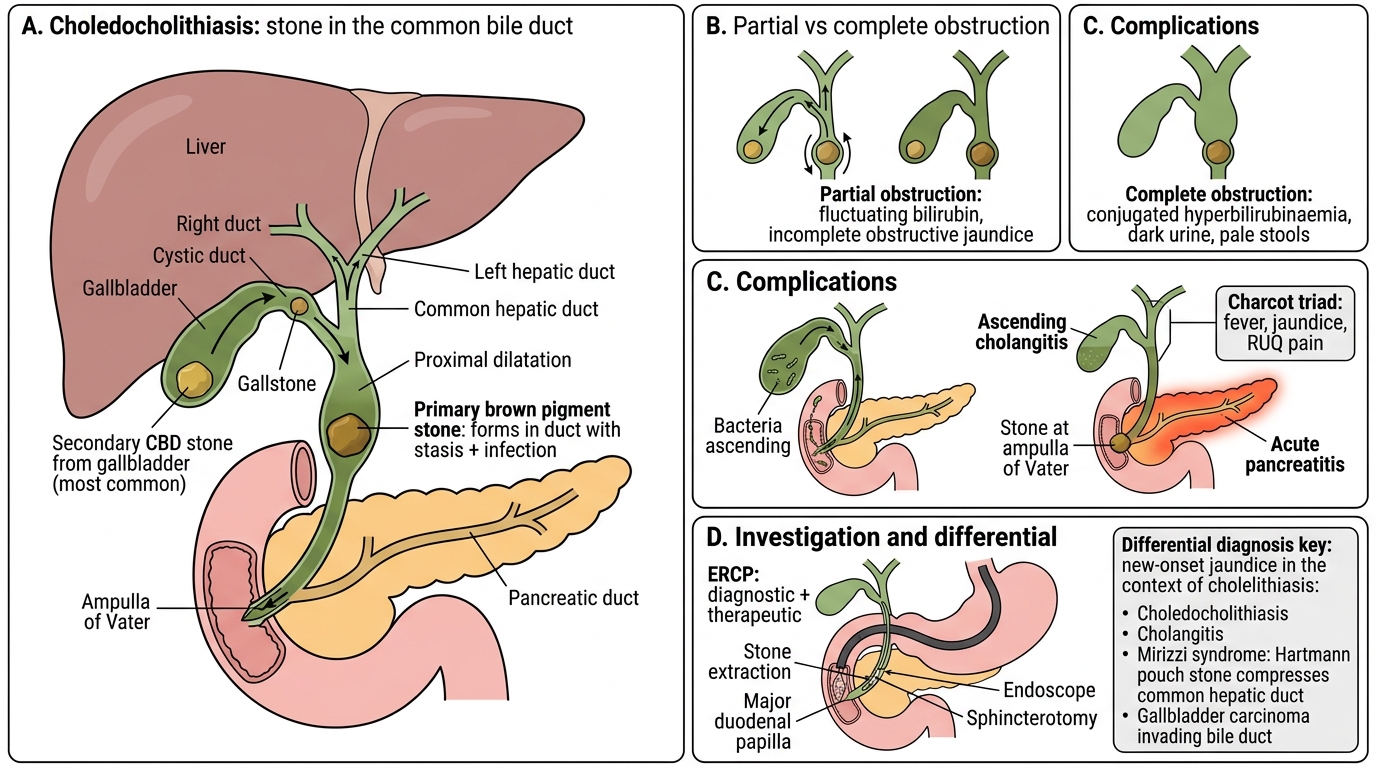
Choledocholithiasis and Obstructive Jaundice
Choledocholithiasis — stone in the common bile duct — may be:
• Secondary: stone migrates from the gallbladder (most common)
• Primary: brown pigment stone forms de novo in the duct (biliary stasis + infection)
Consequences
1. Partial obstruction → incomplete obstructive jaundice (fluctuating bilirubin)
2. Complete obstruction → progressive conjugated hyperbilirubinaemia, dark urine, pale stools (cross-reference SDL 1)
3. Biliary stasis → ascending cholangitis (Charcot's triad)
4. Stone at ampulla of Vater → acute pancreatitis
Investigation note: ERCP (endoscopic retrograde cholangiopancreatography) is both diagnostic and therapeutic — allows stone extraction and sphincterotomy.
Clinical integration: In a patient with cholelithiasis developing new-onset jaundice, the differential includes choledocholithiasis, cholangitis, Mirizzi syndrome (large stone in Hartmann's pouch compressing the common hepatic duct externally), and gallbladder carcinoma invading the bile duct.