Page 23 of 32
PA24.9 | Liver Disease & Tumour Morphology — Practical — SDL Guide
Learning Objectives
- Recognise macrovesicular steatosis and identify the displaced nucleus as the key diagnostic feature in fatty liver.
- Distinguish the cellular changes of acute viral hepatitis — ballooning degeneration, Councilman bodies, lobular disarray — from normal hepatic architecture.
- Describe portal inflammation, interface hepatitis, and ground-glass hepatocytes as markers of chronic hepatitis.
- Identify Mallory-Denk bodies and perivenular fibrosis as hallmarks of alcoholic hepatitis.
- Differentiate the gross and microscopic appearances of cirrhosis, including reticulin and trichrome staining patterns.
- Recognise hepatocellular carcinoma by its trabecular growth pattern, bile production, cellular atypia, and vascular invasion.
- Apply a systematic reading framework — architecture → hepatocyte changes → inflammation/fibrosis → benign vs malignant — to unknown liver slides.
INSTRUCTIONS
Liver biopsies and resection specimens are among the most frequently examined tissues in surgical pathology. The hepatobiliary lesions you will encounter in this practical — fatty change, hepatitis, cirrhosis, and carcinoma — follow recognisable morphological patterns that, once learnt, allow rapid, confident diagnosis. This module walks you through each pattern with gross and histological correlates, building toward a systematic slide-reading strategy you can apply in the examination hall and on the wards.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 18 (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 21 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old man with a long history of alcohol use presents with jaundice, ascites, and a tender hepatomegaly. His biopsy shows swollen hepatocytes, eosinophilic cytoplasmic inclusions, neutrophil infiltrates, and perivenular fibrosis. At the end of this session you will be able to name every one of those findings, grade their severity, and explain how they differ from viral hepatitis seen in the slide tray next to it.
WHY THIS MATTERS
Liver morphology questions appear in both theory and practical examinations at Year-2. More practically, the patterns you master today — steatosis, hepatitis activity grading, cirrhosis staging, and HCC recognition — are the same patterns you will interpret alongside the radiologist and hepatologist in clinical years. The ability to read a liver biopsy report intelligently depends on knowing what the words mean at the microscope level.
RECALL
Before reading on, take 60 seconds to answer these from memory:
- What is the normal relationship between hepatocytes and central veins in a hepatic lobule?
- Where do portal triads lie, and what three structures do they contain?
- What does reticulin stain in the liver, and why would its collapse matter?
If any answer is uncertain, spend two minutes with your Year-1 Physiology / Biochemistry notes on hepatic microanatomy before proceeding — the rest of this session builds on that scaffold.
The Slide-Reading Framework
Systematic Framework for Reading Liver Slides
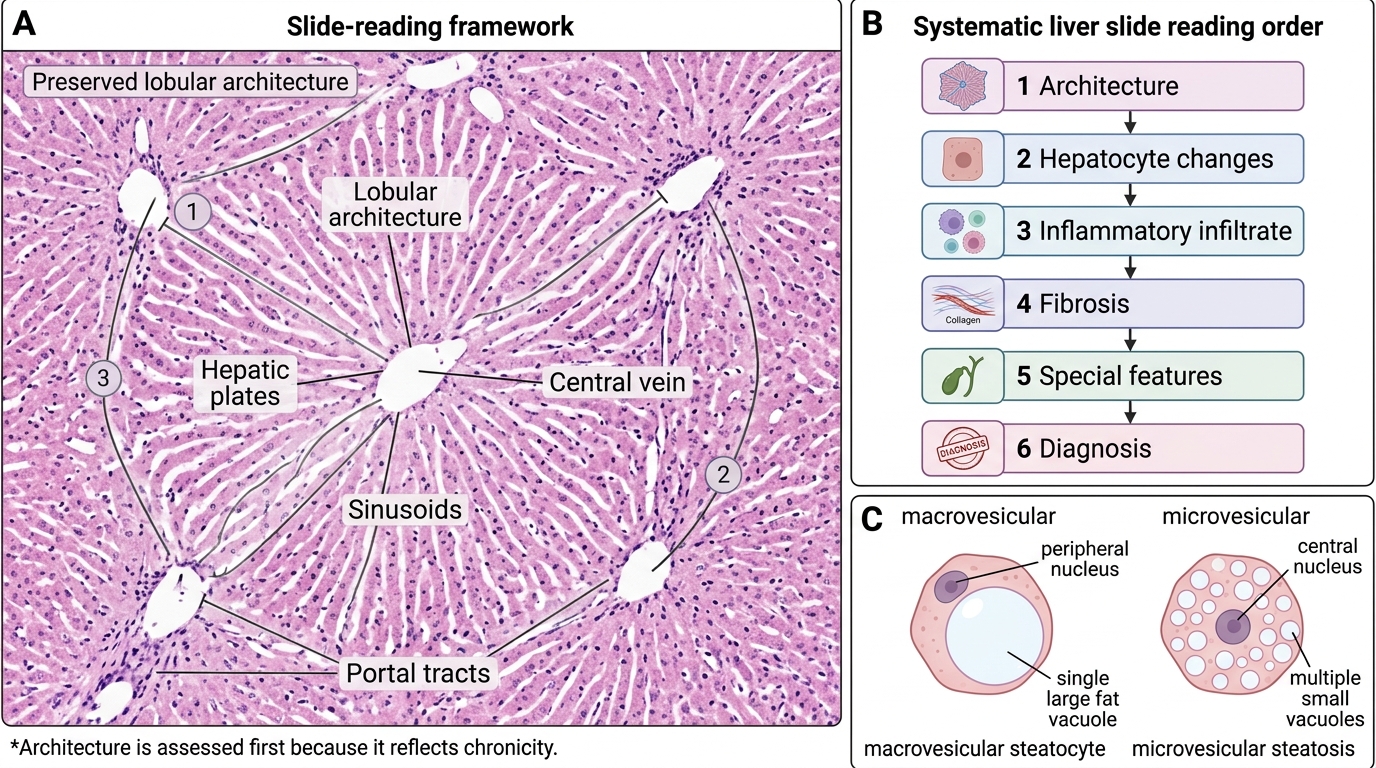
A systematic approach prevents pattern-matching errors. Always read a liver slide in this order:
- Architecture: Is the lobular pattern preserved? Are there nodules surrounded by fibrous bands?
- Hepatocyte changes: Ballooning? Steatosis? Inclusions? Dysplasia?
- Inflammatory infiltrate: Portal only, or lobular? Neutrophils or lymphocytes?
- Fibrosis: Distribution and stage — portal, bridging, or cirrhotic?
- Special features: Bile production, vascular invasion, ground-glass cells?
- Diagnosis: Apply the findings to name the lesion.
This order works because architecture is lost last — it tells you the most about chronicity — while hepatocyte changes and inflammation refine the aetiology.
Fatty Liver (Hepatic Steatosis)
Hepatic Steatosis: Macrovesicular Fatty Change
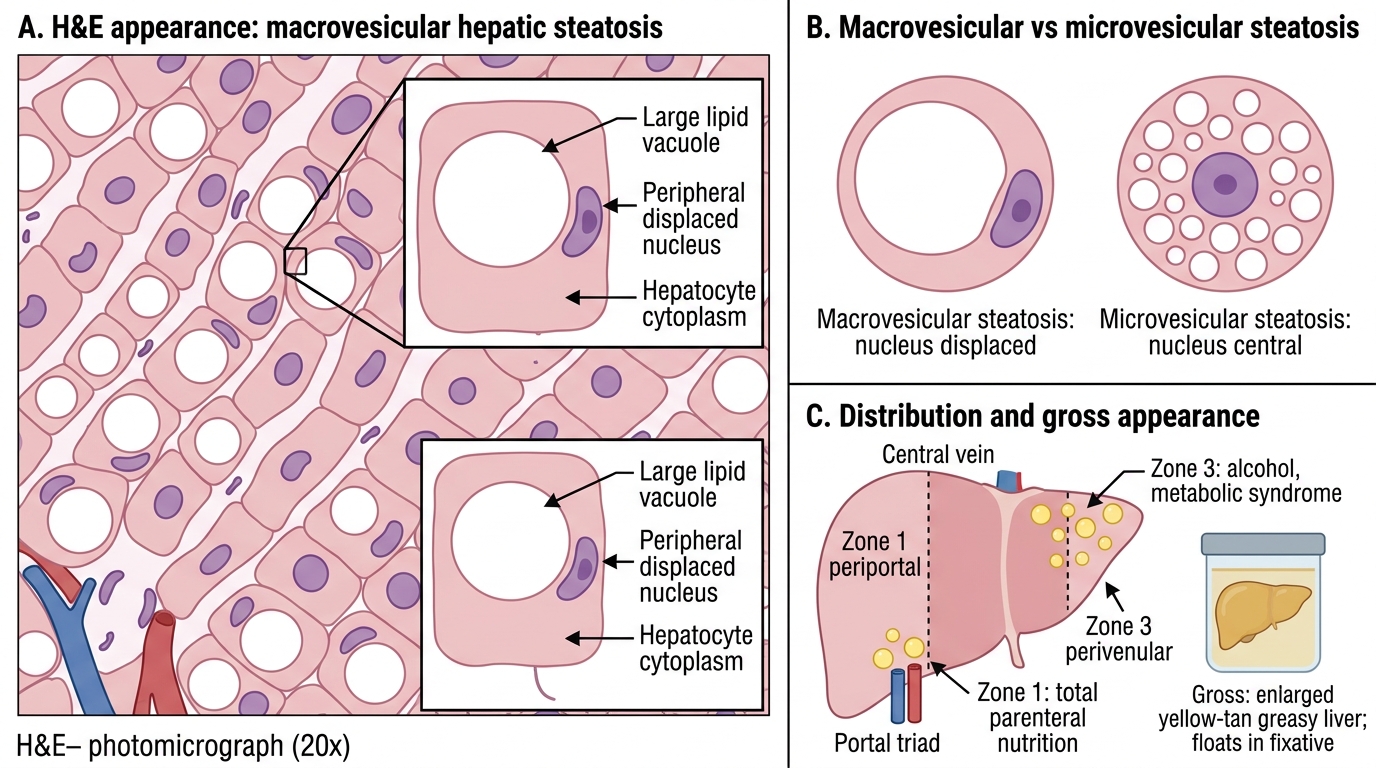
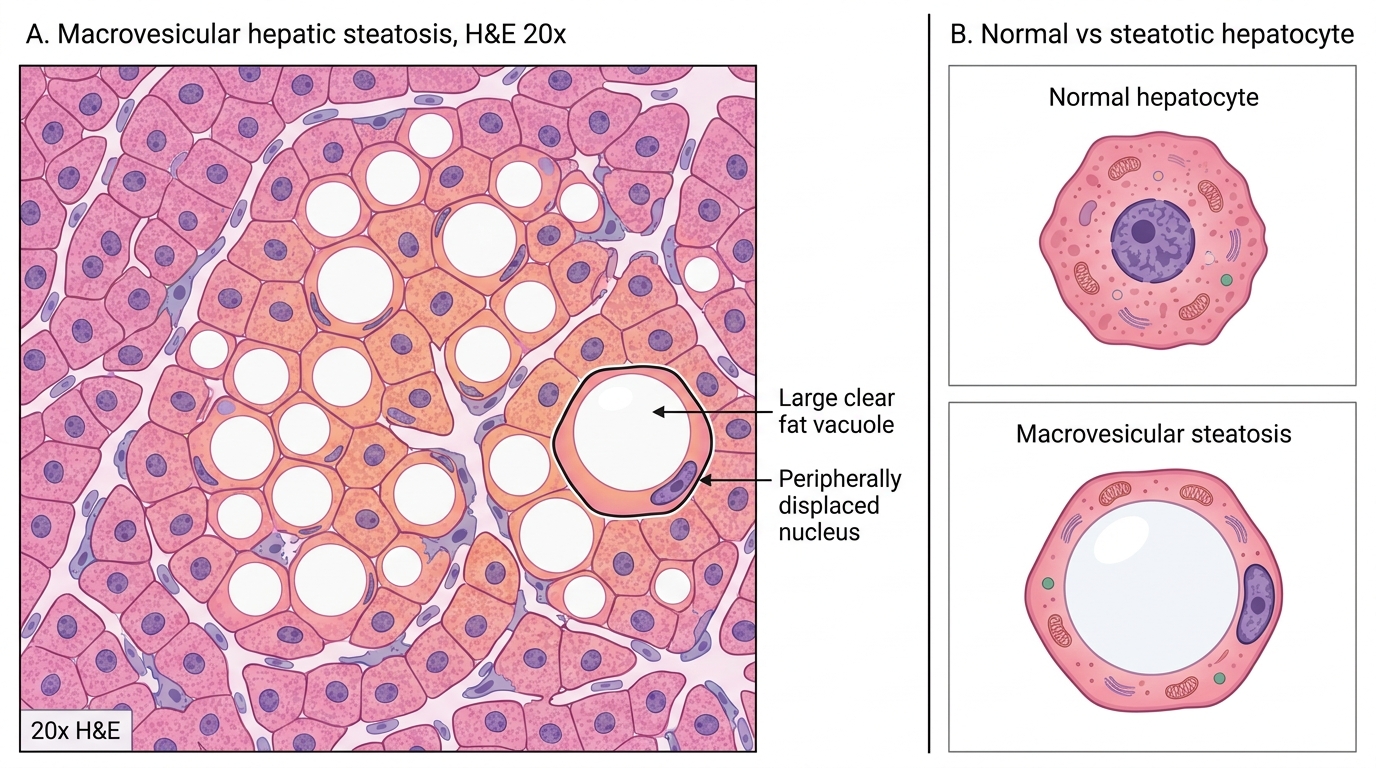
Macrovesicular steatosis is the dominant pattern in alcohol-related and non-alcoholic fatty liver disease (NAFLD). Each affected hepatocyte contains a single large lipid vacuole that occupies most of the cytoplasm and displaces the nucleus to the periphery ("signet-ring" silhouette).
On H&E, fat dissolves during processing, leaving an optically clear, round vacuole within the cell. The key diagnostic detail is the peripherally displaced nucleus — this distinguishes a large fat vacuole from glycogen accumulation (which does not displace the nucleus).
Microvesicular steatosis (multiple small vacuoles, nucleus remains central) is rarer and signals acute fatty liver of pregnancy or Reye syndrome — do not confuse the two.
Distribution matters: perivenular (zone 3) steatosis suggests alcohol or metabolic syndrome; periportal (zone 1) steatosis suggests total parenteral nutrition.
Macrovesicular Hepatic Steatosis on H&E
Gross: liver is enlarged, yellow-tan, greasy, and floats in fixative.
SELF-CHECK
On an H&E section of liver, you see hepatocytes with optically clear cytoplasmic vacuoles. The nuclei are pushed to the cell periphery. Which feature best confirms these vacuoles contain lipid rather than glycogen?
A. Peripheral nuclear displacement by the vacuole
B. Vacuoles of varying size scattered across the lobule
C. Vacuoles that stain red with PAS after diastase digestion
D. Predominant zone-3 (perivenular) distribution
Reveal Answer
Answer: A. Peripheral nuclear displacement by the vacuole
Peripheral nuclear displacement is the single most reliable H&E feature distinguishing macrovesicular fat vacuoles from glycogen accumulation. Glycogen-filled cells also have clear cytoplasm but the nucleus remains central. PAS-diastase (option C) stains glycogen red — positivity rules out lipid. Zone-3 distribution (option D) is an aetiological clue but does not confirm the vacuole type. Varying vacuole size (option B) can be seen in both fat and other changes.
Acute Viral Hepatitis
Acute Viral Hepatitis: Lobular Injury Pattern
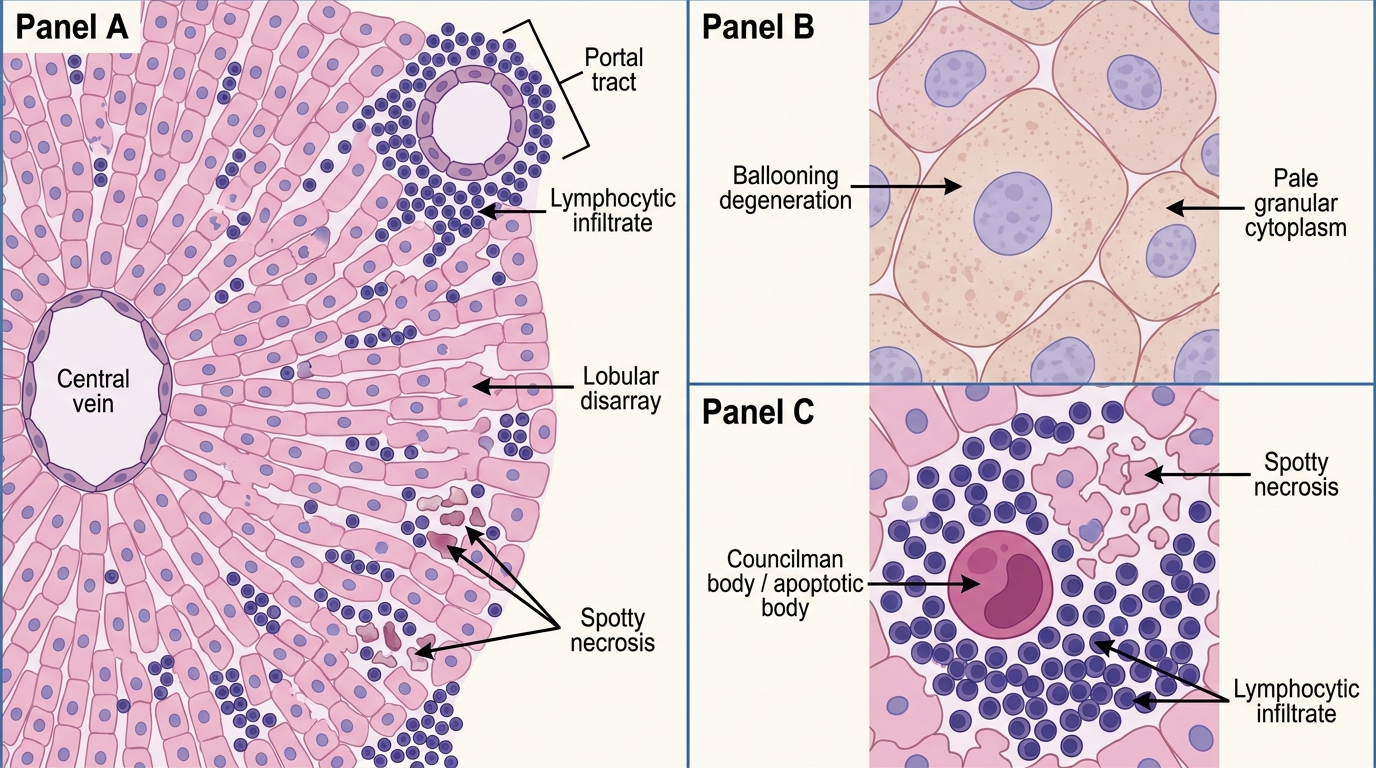
Acute hepatitis from hepatotropic viruses (HAV, HBV, HCV, HEV) produces a stereotyped lobular injury pattern:
Ballooning degeneration — The most visible change: hepatocytes swell dramatically, cytoplasm becomes pale and granular ("feathery"), cell membrane loses its sharp outline. Caused by endoplasmic-reticulum stress and impaired secretory function.
Councilman bodies (apoptotic bodies) — Rounded, deeply eosinophilic, condensed dead hepatocytes, often extruded from the liver plate. They represent hepatocyte apoptosis and are a hallmark of acute viral hepatitis, though not exclusive to it.
Lobular disarray — Loss of the orderly two-cell-thick hepatic plate pattern; liver cells appear haphazardly arranged due to cell swelling and dropout.
Spotty (focal) necrosis — Individual hepatocyte death with inflammatory infiltrate, distributed randomly throughout the lobule. In severe cases, confluent necrosis (bridging, submassive) can occur.
Inflammatory infiltrate: predominantly lymphocytic, both portal and lobular; mild portal expansion.
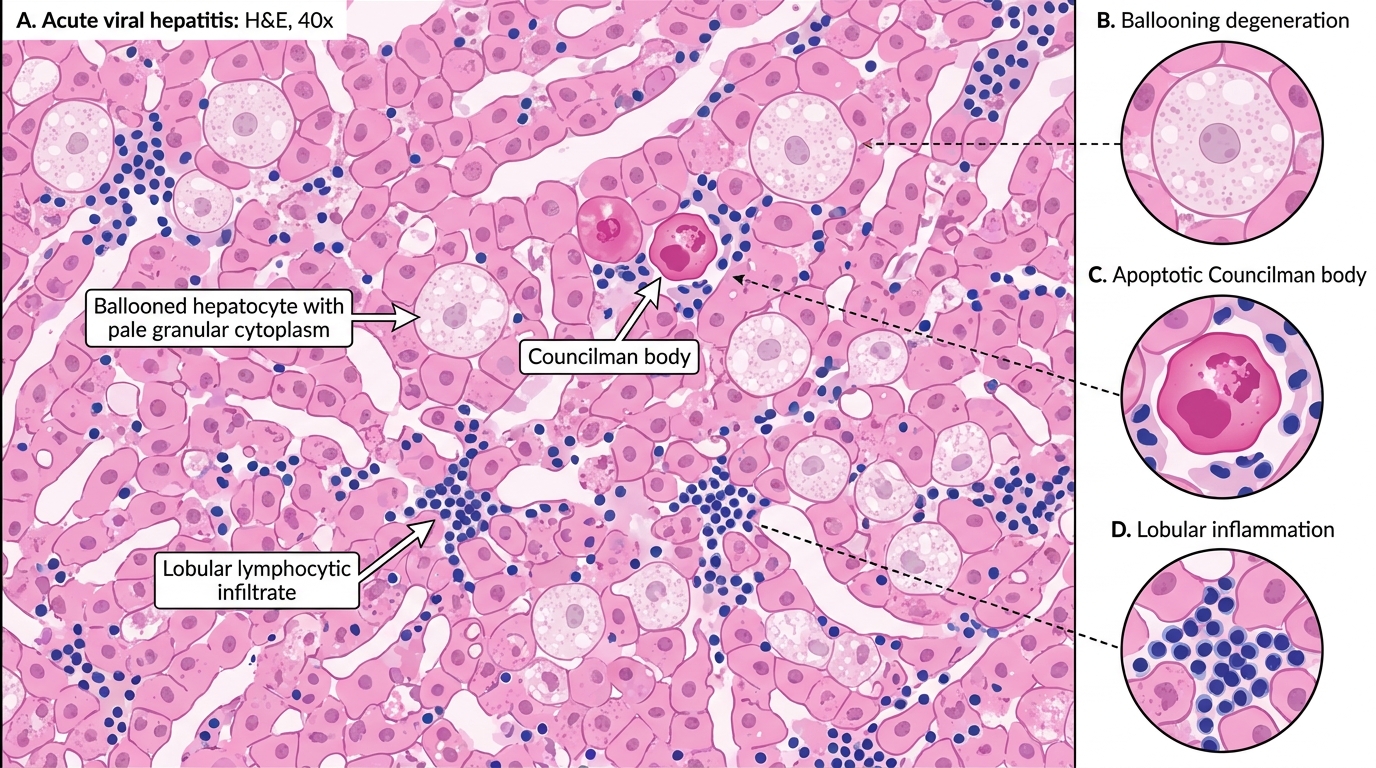
Acute Viral Hepatitis on H&E
Recovery: in HAV/HEV, complete architectural restoration. In HBV/HCV, chronicity is common.
SELF-CHECK
Which combination of histological findings is MOST characteristic of acute viral hepatitis?
A. Macrovesicular steatosis, Mallory-Denk bodies, neutrophil infiltrate
B. Regenerative nodules surrounded by fibrous septa, absent central veins
C. Trabecular growth pattern, bile plugs, nuclear pleomorphism
D. Ballooning degeneration, Councilman bodies, lobular lymphocytic infiltrate
Reveal Answer
Answer: D. Ballooning degeneration, Councilman bodies, lobular lymphocytic infiltrate
Ballooning degeneration + Councilman bodies + lobular lymphocytic infiltrate is the triad of acute viral hepatitis (option D). Option A describes alcoholic hepatitis (steatosis + Mallory-Denk bodies + neutrophils). Option B is cirrhosis. Option C is hepatocellular carcinoma. Recognising these triads is the key to practical diagnosis.