Page 24 of 32
PA24.9 | Liver Disease & Tumour Morphology — Practical — SDL Guide (Part 2)
Chronic Hepatitis
Chronic Hepatitis: Histological Hallmarks
Chronic hepatitis is defined as hepatic inflammation persisting beyond 6 months. The histological hallmarks differ from acute hepatitis:
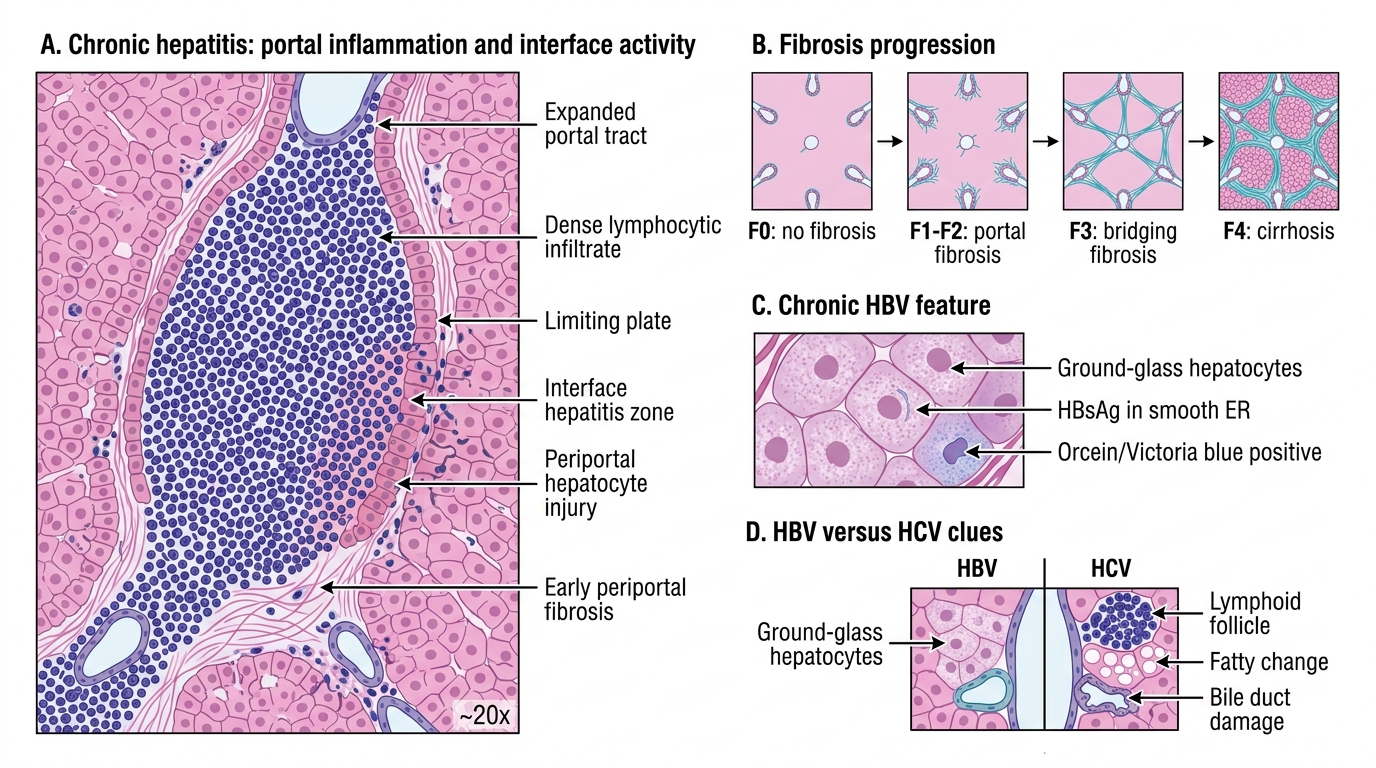
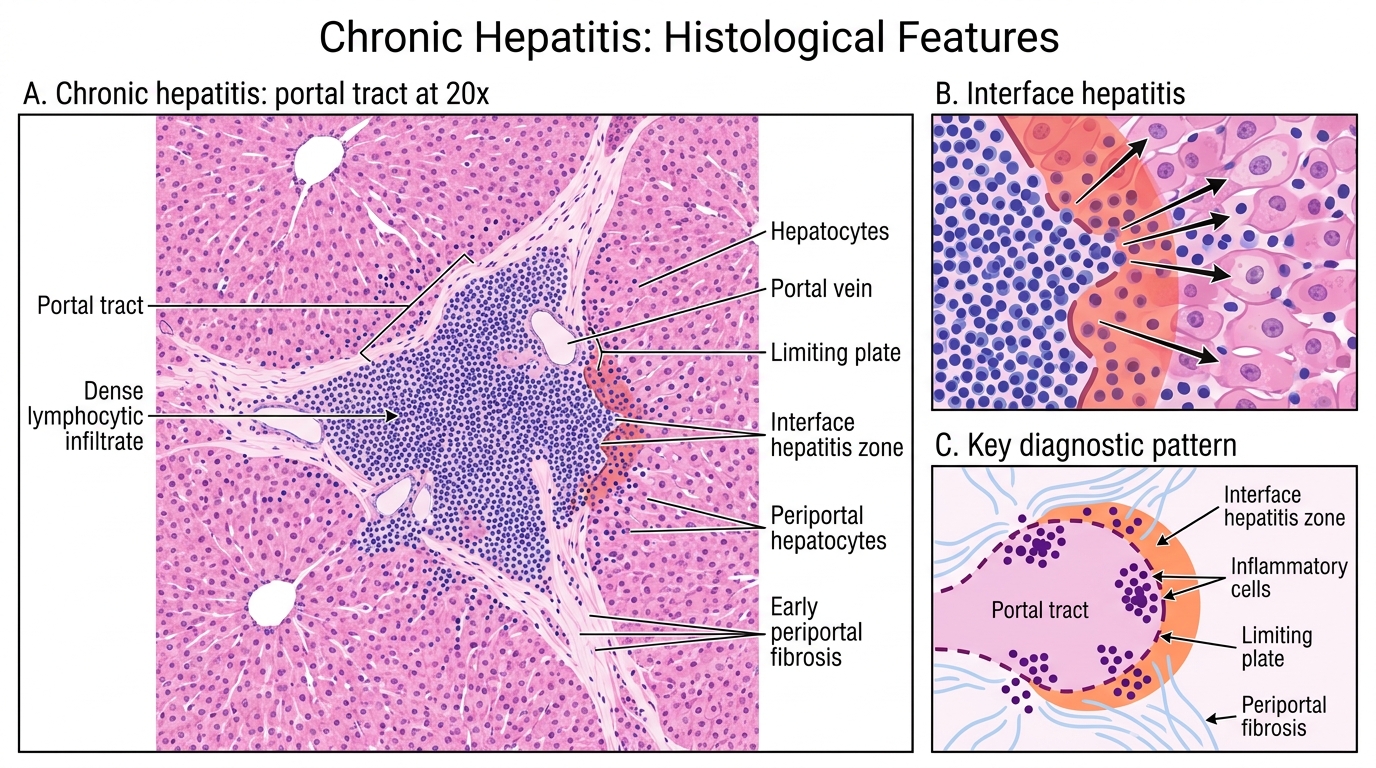
Portal inflammation — Dense lymphocytic (± plasma cell) infiltrate expanding and filling portal tracts. The degree of portal inflammation correlates with disease activity.
Interface hepatitis (formerly piecemeal necrosis) — Lymphocytes spill beyond the portal limiting plate to destroy periportal hepatocytes. This is the active front of immune damage and is the key marker of histological activity.
Fibrosis — Begins as portal fibrosis, extends as bridging fibrosis (portal-to-portal or portal-to-central bridging), and ultimately becomes cirrhosis. Staged 0-4 (Metavir) or 0-6 (Ishak).
Ground-glass hepatocytes — Pale, finely granular cytoplasm due to smooth-ER proliferation filled with HBsAg. Seen in chronic HBV infection. On special stains: positive with orcein or Victoria blue (HBsAg).
HCV tends to cause: lymphoid follicles in portal tracts, fatty change (especially genotype 3), and bile duct damage — a useful discriminator from HBV.
Chronic Hepatitis: Portal Inflammation and Interface Hepatitis
CLINICAL PEARL
The Metavir score combines two numbers: A (activity, 0-3) and F (fibrosis, 0-4). A2F3 means moderate activity with severe fibrosis — almost bridging cirrhosis. When you read a biopsy report with these numbers, the A reflects how inflamed the liver is right now (and therefore how urgently antiviral treatment is needed), while F reflects cumulative structural damage. Activity can improve on treatment; fibrosis beyond F3 is largely irreversible.
Alcoholic Hepatitis
Alcoholic Hepatitis: Key Histological Features
Alcoholic hepatitis (AH) is a histologically distinct pattern of alcohol-related liver injury, different from simple steatosis. The four key features:
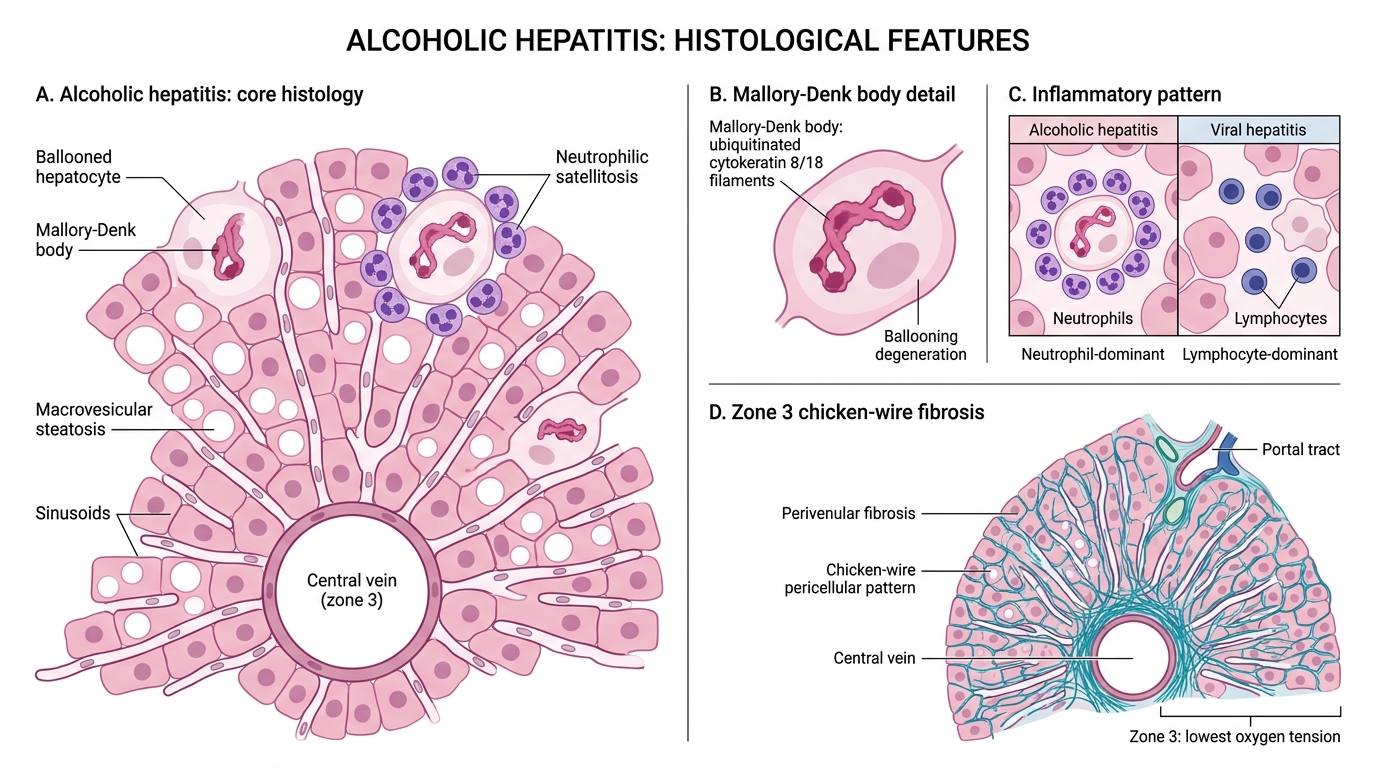
- Mallory-Denk bodies (formerly Mallory hyaline) — Irregular, rope-like, deeply eosinophilic cytoplasmic inclusions within ballooned hepatocytes. Composed of ubiquitinated, misfolded intermediate filaments (cytokeratin 8/18). Not pathognomonic of AH alone (also seen in PBC, Wilson, NASH) but are the most visually striking feature.
- Neutrophilic satellitosis — Neutrophils clustering around Mallory-containing hepatocytes. This neutrophil-dominant inflammation distinguishes AH from viral hepatitis (which is lymphocyte-dominant).
- Perivenular fibrosis ("chicken-wire" fibrosis) — Fibrosis radiating from zone 3 (central vein) outward along the sinusoids, giving a pericellular chicken-wire pattern on trichrome stain. A direct alcohol toxic effect; zone 3 is most vulnerable due to lowest oxygen tension.
- Steatosis coexisting in background hepatocytes.
Severe AH: Mortem de Brouwer lobular inflammation, bridging necrosis, and cholestasis (bile plugs) can develop.
The combination of steatosis + Mallory-Denk bodies + neutrophilic inflammation + zone-3 perivenular fibrosis defines alcoholic steatohepatitis (ASH) — analogous to NASH but aetiologically distinct.
SELF-CHECK
A liver biopsy from a 45-year-old chronic alcohol user shows ballooned hepatocytes containing rope-like eosinophilic cytoplasmic inclusions, with neutrophils clustering around these cells and pericellular fibrosis in zone 3. What are the inclusions?
A. Ground-glass inclusions of HBsAg
B. Mallory-Denk bodies (ubiquitinated cytokeratin aggregates)
C. Councilman bodies (apoptotic hepatocyte remnants)
D. Lipofuscin granules
Reveal Answer
Answer: B. Mallory-Denk bodies (ubiquitinated cytokeratin aggregates)
Rope-like eosinophilic cytoplasmic inclusions in ballooned hepatocytes surrounded by neutrophils in a chronic alcohol user = Mallory-Denk bodies. They are aggregates of ubiquitinated cytokeratin 8/18. Ground-glass inclusions (option A) are smooth, pale, and peri-nuclear, associated with HBV. Councilman bodies (option C) are extruded, rounded, cell-death remnants — not intracytoplasmic inclusions. Lipofuscin is brown, fine-granular, and accumulates with age — not rope-like.
Cirrhosis — Gross and Microscopic
Cirrhosis: Gross and Microscopic Features
Cirrhosis is the end-stage of chronic liver disease, defined by two co-occurring features: extensive fibrosis and regenerative nodule formation. Both must be present; fibrosis alone (even bridging) is not cirrhosis.
Gross appearance:
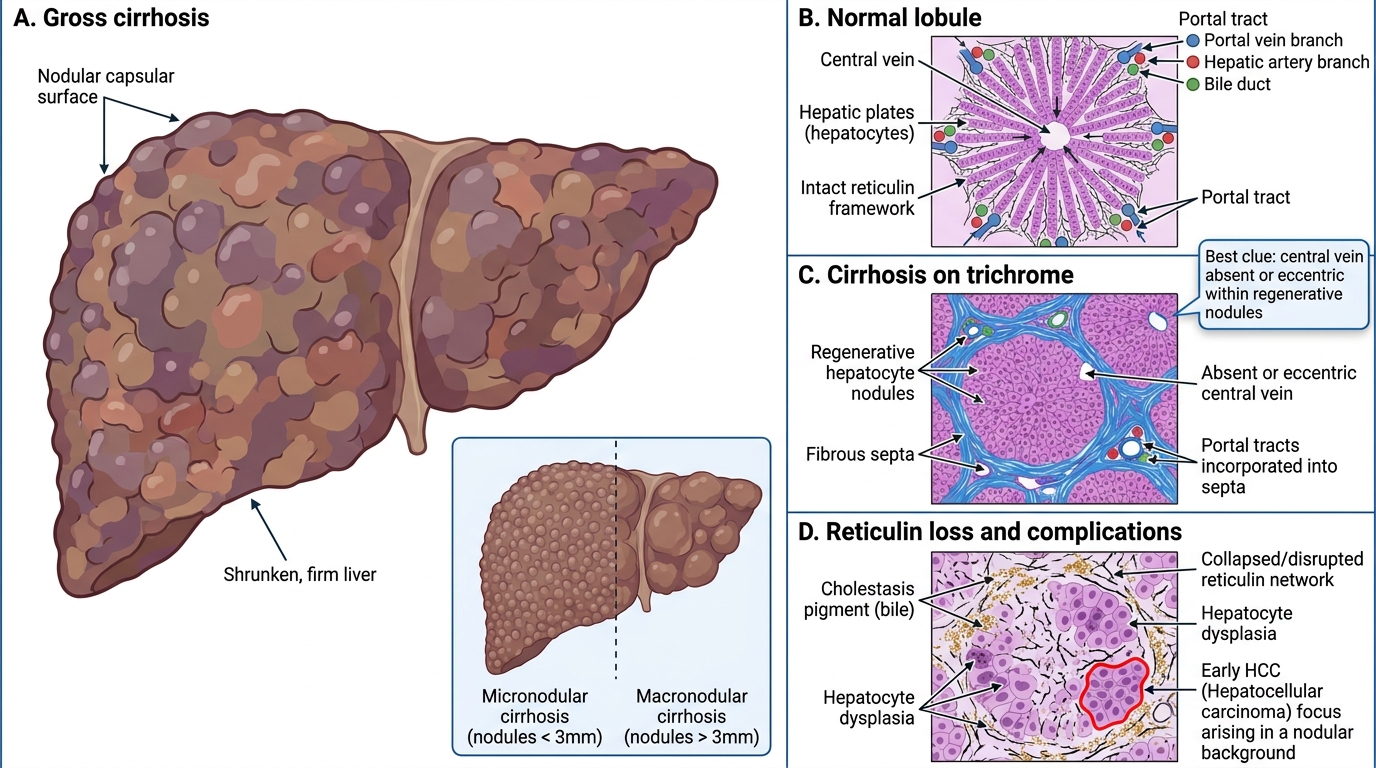
- Micronodular cirrhosis (nodules <3 mm, uniform): alcohol-related, haemochromatosis.
- Macronodular cirrhosis (nodules >3 mm, variable): viral hepatitis (HBV, HCV).
- Mixed patterns exist. Liver is shrunken (end-stage), firm, and has a nodular capsular surface.
Microscopic:
- Regenerative nodules — clusters of hepatocytes with internal blood supply (hepatic arterioles) but no organised central vein → lobular landmarks are lost.
- Fibrous septa — stain blue on Masson trichrome, providing the scaffold around nodules.
- Reticulin stain: collapse of the normal reticulin network within nodules marks loss of liver plate architecture. Intact reticulin = preserved architecture (reactive nodule or partial collapse).
- Portal tracts can be incorporated into septa and become unidentifiable.
Key distinction: in cirrhosis the central vein is absent or eccentric within nodules — this is the single best histological clue that you are looking at a regenerative nodule rather than normal parenchyma.
Complications visible histologically: cholestasis, hepatocyte dysplasia (large-cell and small-cell), and frank HCC arising within nodular background.
SELF-CHECK
On a trichrome-stained liver section, you see irregular blue-staining bands completely surrounding groups of hepatocytes. The central vein is absent within the hepatocyte clusters. What is the diagnosis?
A. Bridging fibrosis (F3) without cirrhosis
B. Massive hepatic necrosis
C. Cirrhosis with regenerative nodules
D. Hepatic amyloidosis
Reveal Answer
Answer: C. Cirrhosis with regenerative nodules
Blue fibrous bands (trichrome) completely surrounding hepatocyte clusters that lack a central vein = cirrhosis with regenerative nodules. The absence of the central vein within nodules is the key differentiator from bridging fibrosis (F3), where the lobular landmarks — though bridged — can still be partially identified. Massive necrosis shows collapse and dropout, not nodule formation. Amyloid deposits in a homogeneous pattern in sinusoidal walls, not as complete nodule-surrounding septa.